

Abstract
Background: The survival benefit of chemotherapy compared to best supportive care (BSC) after percutaneous transhepatic biliary drainage (PTBD) was evaluated in patients with pancreatic or biliary tract cancer. Patients and Methods: A retrospective registry study was conducted at a tertiary-level university hospital. The endpoint was survival measured from the PTBD and the initiation of chemotherapy. Results: Among 158 patients (mean age=74 years, range=43-93 years; 51.9% women), 82 (51.9%) had pancreatic cancer and 76 (48.1%) had biliary tract cancer. After PTBD, 32 (20.3%) patients received chemotherapy and had a median survival of 11.7 months; 126 (79.7%) patients received only BSC resulting in a median survival of 1.7 months. The hazard ratio for survival at 1 year for patients who received chemotherapy compared to BSC was 0.22 (95% confidence interval=0.12-0.41, p<0.001). Conclusion: After PTBD, patients with pancreatic or biliary tract cancer should be critically evaluated by an oncologist to determine whether chemotherapy is possible, as it seems to significantly improve survival compared to BSC.
- Cancer
- chemotherapy
- hyperbilirubinemia
- biliary obstruction
- percutaneous biliary drainage
Hyperbilirubinemia due to malignant biliary obstruction is quite common in patients with advanced pancreatic and biliary tract cancer and the oncological treatment is challenging (1, 2). The first choice for the treatment of malignant biliary obstruction worldwide is endoscopic biliary drainage. Percutaneous transhepatic biliary drainage (PTBD) is a treatment option when endoscopic drainage is not feasible due to duodenal obstruction or previous surgery, or has been insufficient. These patients with PTBD had usually unfavorable outcome; in our retrospective series, the median overall survival after PTBD was 2.6 months (3).
New chemotherapy combinations have shown a positive trend of prolonged survival in patients with pancreatic and biliary tract cancer (4-7). However, hyperbilirubinemia caused by biliary obstruction precludes the administration of chemotherapy, and these patients have typically been excluded from clinical studies (4, 5, 8). There are very limited data concerning the utility of chemotherapy for this patient group with malignant biliary obstruction not suitable for endoscopic biliary drainage and therefore treated with PTBD (9-12).
In the present study, we investigated the benefit of chemotherapy compared to best supportive care after PTBD in patients with pancreatic or biliary tract cancer with hyperbilirubinemia caused by biliary obstruction.
Patients and Methods
A detailed description of the entire study population of 643 patients was published previously (3). The study protocol was approved by our Institution’s Ethics Committee (no. 140/2011). This retrospective sub-analysis included patients with chemotherapy-naïve pancreatic or biliary tract cancer with malignant biliary obstruction who were treated with PTBD and followed-up at a tertiary-level university hospital between 2003 and 2016. Full electronic medical records, including chemotherapy records, were available for that time period.
All drainage procedures were performed with the patient under anesthesia. The procedure was performed by experienced interventional radiologists guided by ultrasonography and fluoroscopy according to previously documented methods (13). A self-expanding metal stent was inserted in 125 (79.1%) patients, and external drainage was used in 33 (20.9%) patients.
The patient population was divided into two groups: Patients eligible to receive chemotherapy, and those treated with only best supportive care after PTBD. We compared the outcomes of these patient groups and the following data were retrieved from the electronic medical records: Age, sex, pre-procedure American Society of Anesthesiologists physical status classification class (14), Eastern Cooperative Oncology Group performance status (ECOG PS) (15), comorbidities, type of cancer, and serum bilirubin level. We recorded the highest bilirubin value observed in the 7 days before the procedure, and the lowest value in the 30 days after the procedure and at the time of evaluation by an oncologist.
Time of death was acquired from death certificates (Statistics Finland) (16). Survival was defined as the interval starting from the PTBD in the group treated with best supportive care, and the initiation of chemotherapy in the chemotherapy-treated group, and ending with the patient’s death or last follow-up.
Statistical analysis. Statistical analyses were performed using SPSS Statistics for Windows, Version 25.0 (IBM Corp, Armonk, NY, USA). Summary data are presented as means with standard deviation, or as medians with 25-75th percentiles (interquartile range, IQR). Between-group comparisons were performed by Student’s t-test or Welch test for continuous data, and the chi-squared test or Fisher’s exact test for categorical data. The log-rank test was used to compare survival times in univariate analyses. We used a multivariable adjusted time-dependent Cox proportional hazards model to avoid and minimize the immortal time bias to determine the impact of chemotherapy treatment on the 1-year survival rate (17). To minimize biases and validate patient groups in the multivariable model, we constructed a directed acyclic graph (DAG) to derive a minimally sufficient adjustment set. The DAG was drawn using the DAGitty tool (18). The DAGitty model indicated that the following parameters should be taken into account in the adjusted Cox model: Patient age (≤70, >70 years), number of co-morbidities (none, 1-2, >2), ECOG PS (0-1, 2, 3-4), bilirubin level after drainage [<60, ≥60 μmol/l; according to a receiver-operating characteristic curve from our previous study (3)], and the type of cancer (pancreatic or biliary tract). The results of the Cox model are presented as hazard ratios and 95% confidence intervals. Two-tailed p-values are reported.
Results
The study group comprised 158 patients, of which 82 (51.9%) had pancreatic cancer and 76 (48.1%) had biliary tract cancer. The diagnosis of cancer was verified by histology in 40 (25.3%) patients, by cytology in 88 (55.7%) patients and by radiology in 30 (19.0%) patients. The median time from cancer diagnosis to drainage was 0.3 months (25th-75th percentiles 0.2-0.7 months).
Patient demographics and clinical characteristics are presented in Table I. The mean age for the whole cohort was 74 years (range=49-93 years). A low American Society of Anesthesiologists class (p=0.008) and low ECOG PS grade (p<0.001) were more common in the chemotherapy group than in the best supportive care group (Table I). The chemotherapy group had a higher proportion of males than the best supportive care group (p=0.003), while patients in the best supportive care group were older than those in the chemotherapy group (p<0.001).
Demographics and clinical characteristics of 158 patients with pancreatic or biliary tract cancer according to therapy after percutaneous transhepatic biliary drainage. Data represent the number of patients (%) unless otherwise noted.
After PTBD, 62 (39.2%) patients were evaluated by an oncologist. Their median bilirubin level after PTBD was 33.5 μmol/L (IQR=18.8-52.8 μmol/l). Thirty-two (51.6%) of these 62 patients received chemotherapy, while 30 patients (48.4%) did not receive chemotherapy for the following reasons: 16 patients had ECOG PS 3, 10 patients had ECOG PS 4 and four patients with ECOG PS 1-2 refused chemotherapy. Ninety-six patients from the study population were not evaluated by an oncologist and their median bilirubin level after PTBD was 90.0 μmol/l (IQR=45.5-229.0 μmol/l; missing values for 11 patients). The main exclusion criteria for evaluation of chemotherapy in addition to high bilirubin level were poor performance status, advanced disease, age, co-morbidities, and patient refusal.
Among the 32 (20.3%) patients who received chemotherapy, 17 (53.1%) had pancreatic cancer and 15 (46.9%) had biliary tract cancer (Table I). The corresponding figures in the best supportive care group were 65 (51.6%) and 61 (48,4%), respectively. The median time for the initiation of chemotherapy after PTBD was 1.8 months (IQR=0.7-4.6 months). Single-agent gemcitabine was the first-line treatment for 76% (13/17) of patients with pancreatic cancer and 73% (11/15) of patients with biliary tract cancer. Combination chemotherapy was given to 24% (4/17) of patients with pancreatic cancer (gemcitabine with oxaliplatin or erlotinib, etoposide with cisplatin, or fluorouracil with oxaliplatin and irinotecan) and 27% (4/15) of patients with biliary tract cancer (gemcitabine with cisplatin). Only two patients with pancreatic cancer and one patient with biliary tract cancer received a second-line treatment. No patient received a third-line treatment.
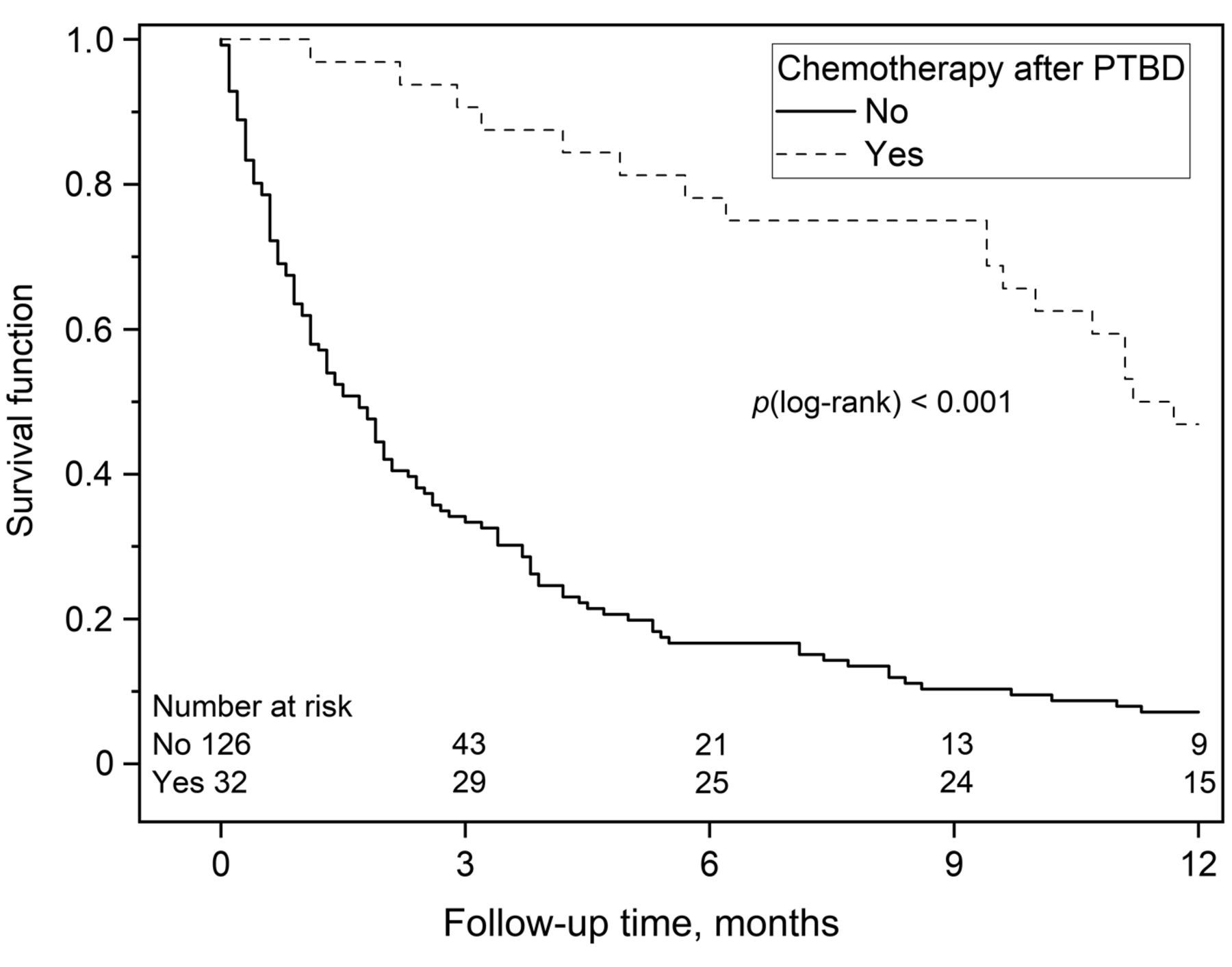
The median survival of the 32 chemotherapy-treated patients was 11.7 months, and 15 (46.9%) patients were alive at 1 year after PTBD (p<0.001; Table II, Figure 1). Both cancer groups gained significant survival benefits with chemotherapy, with a median survival of 11.2 months for the pancreatic cancer group and 15.1 months for the biliary tract cancer group. The median survival of the 126 patients treated with best supportive care was 1.7 months (p<0.001; Table II, Figure 1); 2.0 months in patients with ECOG PS 0-2, and 0.9 months with ECOG PS 3-4 (p=0.216). Nine (7.1%) of the patients with best supportive care were alive at 1 year after PTBD.
Outcome after percutaneous transhepatic biliary drainage (PTBD) in 158 patients with pancreatic or biliary tract cancer.

{kind=link}
Kaplan–Meier survival analysis of 158 patients with pancreatic or biliary tract cancer according to therapy after percutaneous transhepatic biliary drainage (PTBD).
According to the time-dependent multivariable adjusted Cox regression model, the hazard ratio for survival at 1 year was 0.22 (95% confidence interval=0.12-0.41, p<0.001) for patients who received chemotherapy compared to patients who received best supportive care.
Discussion
Our results showed that patients with pancreatic or biliary tract cancer and malignant biliary obstruction treated with PTBD and thereafter chemotherapy had significantly better survival compared to those treated with best supportive care after drainage. In all but one of the previous PTBD studies (19), information concerning chemotherapy was brief, with few or no details about the regimens (9, 11, 20), and the focus has mainly been on the technical aspects of biliary drainage.
In a recent, retrospective study from South Korea including patients with hilar cholangiocarcinoma, chemotherapy was given to 34 patients and best supportive care to 74 patients after drainage (12). In this study, the standard chemotherapy for biliary tract cancer was gemcitabine combined with cisplatin. This combination treatment has been associated with a significant survival advantage compared to gemcitabine alone, without substantial toxicity (5). In our biliary tract cancer group (n=15 patients), only four patients received this combination; while 11 patients received gemcitabine alone. In the South Korean study (12), the median survival was 12.8 months for the chemotherapy-treated group and 6.1 months for the best supportive care group. In our series, the median survival was 15.1 months for patients with biliary tract cancer who received chemotherapy after PTBD and 1.9 months for those who received best supportive care. The outcomes may have been even better for our patients with biliary tract cancer if the gemcitabine-cisplatin combination had been used more widely.
In our study, 13 out of 17 patients (76%) with pancreatic cancer received gemcitabine alone as a first-line treatment. Recently, the combination of nab-paclitaxel and gemcitabine was shown in post-hoc registry analyses to significantly improve the outcome of patients with locally advanced and metastatic pancreatic cancer (6). The median survival of our patients with pancreatic cancer treated with chemotherapy was 11.2 months and with best supportive care 1.3 months. The survival figures with the use of the combination therapy would have been even better (21).
A high bilirubin level can diminish hepatic clearance and alter drug metabolism, increasing toxicity; therefore, hyperbilirubinemia has been considered an exclusion criterion for chemotherapy (8, 22). Limited knowledge is available regarding appropriate chemotherapy dosing and management in patients with higher bilirubin levels. Treatment recommendations for patients with hyperbilirubinemia have been based on small phase I studies or retrospective patient series with heterogeneous study populations (4, 5, 8, 23-26). It has been reported that an initial dose reduction is unnecessary for widely used gemcitabine or capecitabine in patients with biliary tract or pancreatic cancer after successful management of biliary obstruction, even with moderate hyperbilirubinemia (27, 28). Chemotherapy may be considered even with higher bilirubin levels than in daily practice (i.e., <1.5-fold the upper limit of the normal range) (29). An ongoing prospective phase I trial (AIO-PAK-0117 PANCHO) is evaluating the safety and efficacy of a combination of nab-paclitaxel and gemcitabine in patients with metastatic pancreatic cancer and hyperbilirubinemia (21).
There are several ways of calculating survival in different study designs. Recently, much attention has been paid to immortal time bias, i.e., the time between diagnosis and the initiation of cancer treatment, which researchers should be aware of to avoid misleading conclusions concerning the benefits of therapy (30-33). For example, in the South Korean study with hilar cholangiocarcinoma (12), survival was calculated from the date of cancer diagnosis to death or the last follow-up. Using a similar definition, the survival of our patients with biliary tract cancer would have been 18.1 months instead of 15.1 months, which was calculated from the initiation of chemotherapy to avoid immortal time bias.
The main strength of our study was that we included all patients treated with PTBD for malignant biliary obstruction due to pancreatic or biliary tract cancer at the same teaching hospital. To the best of our knowledge, this was the first study analyzing the benefit of chemotherapy in patients with malignant biliary obstruction after PTBD including both pancreatic and biliary tract cancer, the most common causes of malignant hyperbilirubinemia. To avoid misleading conclusions, we constructed a DAG to examine biases related to all possible causal variables (18, 34), and used the time-dependent multivariable analysis, which is accurate in estimating treatment effects and includes all patients in the study (17, 30). According to the DAGitty model, a multivariable adjusted, time-dependent Cox regression model was adjusted for patient age, number of co-morbidities, ECOG PS, bilirubin level after PTBD and the type of cancer. This approach gave a hazard ratio of 0.22 (95% confidence interval=0.12-0.41) for survival at 1 year after PTBD for patients who received chemotherapy, with median survival of 11.7 months compared to 1.7 months for patients who received best supportive care. In the latter group, the survival difference between those with ECOG PS 0-2 and ECOG PS 3-4 was only 1 month.
Our study was a single-center, retrospective study, similar to most previous studies on this topic. During the study period, only one-fifth of the patients in our series received chemotherapy after PTBD. According to the latest knowledge concerning hyperbilirubinemia and chemotherapy (21, 35), more patients in our supportive care group would have been eligible to receive and benefit from chemotherapy after PTBD, therefore, an oncological evaluation is important to identify patients eligible for chemotherapy.
Conclusion
Our results show that patients with pancreatic or biliary tract cancer with hyperbilirubinemia should be critically evaluated by an oncologist after PTBD to determine whether chemotherapy is possible. This approach seems to improve survival significantly compared to best supportive care in these patients. Further studies are needed for developing appropriate guidelines for chemotherapy in patients with cancer with hyperbilirubinemia.
Footnotes
This article is freely accessible online.
Authors’ Contributions
JN: Study design; collection of data; quality control of data; data analysis; article preparation, editing, and review. HS, PO, JS, RK: Study design; quality control of data; data analysis; article preparation, editing, and review.
Conflicts of Interest
The Authors have no conflicts of interest to declare. The Authors had full control of all primary data and agree to allow the journal to review their data if requested.
- Received February 3, 2021.
- Revision received April 23, 2021.
- Accepted April 27, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.