

Abstract
Background/Aim: To assess the concordance between IHC and FISH and its influence on tumor type, grade and lympho-vascular invasion (LVI). Materials and Methods: HER2 immunohistochemistry (IHC) to 45 cases of bladder carcinoma, followed by fluorescent in situ hybridization (FISH) were applied. Results: 31.12% cases were IHC positive. Less than 35% of HER2-negative cases presented LVI and this percent increased to 54.54% for +1 HER2 cases. LVI increases up to 57.14% for +2 HER2 cases and slightly decreased for +3 HER2 cases to 42.85%. IHC/FISH concordance was found for 73.34% cases but 31.57% were previously negative and 36.36% scored as +1 by IHC had gene amplification as shown by FISH analysis. T3 was correlated with HER2-IHC (p=0.05) and HER2-FISH (p=0.01). Conclusion: Improved HER2 assessement is needed for urothelial carcinomas. HER2-IHC scored as 0-2 should be validated by and reclassified according to FISH analysis.
- HER2
- bladder cancer
- immunohistochemistry
- fluorescent in situ hybridization
Between tyrosine kinase family members, human epidermal growth factor receptor 2 (also known as HER2, c ERB B2) is heterogeneously expressed in a variety of human malignancies such as breast (1), gastric (2), ovarian (3), renal (4) or bladder cancer (5). Humanized monoclonal antibody-based therapies targeting HER2 overexpression have been certified by Food and Drug Administration (FDA) and are extensively applied in clinical practice for the treatment of metastatic breast cancer. For other malignancies, monoclonal antibodies targeting HER2 overexpression have not represented a widely accepted therapeutic option due to controversial results reported in the literature (6-8). Among malignancies with certified HER2 overexpression, bladder cancer has limited therapeutic options because of controversies regarding the impact of targeted therapies on patient's survival. Assessment of HER2 overexpression and gene amplification is controversial, no well-established protocol has been used for the stratification of patients with HER2 positive bladder cancers and their inclusion into a particular group which can benefit from trastuzumab therapy. Recently, Tschui and his team (9), tried to identify some morphological features of HER2 overexpressing bladder cancer and reported that the micropapillary type is predominant amongst them (9). Like in other cancer types, the usual method applied to highlight HER2 overexpression is immunohistochemistry, a simple and reliable method to detect protein overexpression in tumor cells (10). Different immunohistochemistry protocols are being applied for breast and gastric cancer (10-12). HER2 immunohistochemistry is applied mostly to the primary tumor and to a lesser extend to the corresponding metastasis (13). Also, limited use of fluorescent in situ hybridization (FISH) restricted to those cases classified as “equivocal” (HER2, +2) by immunohistochemistry contributes to misdiagnosed HER2 negative cases in breast and gastric cancers. Recently, several papers reported that anti-HER2 therapy should not be recommended unless true evaluation of HER2 protein expression and gene amplification, this being sustained by previous implementation of the 2013 ASCO/CAP updated guidelines certified to have an increased positive impact on HER2 classification for breast cancers initially classified as having equivocal HER2 IHC results. These new guidelines significantly increased the benefit of HER2-targeted therapy (14-16). In bladder cancer, the widely accepted fact is that HER2 overexpression characterizes the papillary variant (9). Fluorescent and/or chromogen in situ hybridization methods are recommended in order to validate HER2 immunohistochemistry results, especially for +2 positive cases in bladder cancer. Because of these restricted recommendations no data are available about the evaluation of HER2 gene amplification by FISH, for cases noted as +1 by immunohistochemistry. HER2 protein expression remains a controversial issue regarding score assessment of immunohistochemical specimens. Patients with +3 score are directly enrolled into trastuzumab therapy, while for patients with +2 score, additional ISH methods are recommended for gene amplification detection. For +1 HER2-positive cases, the immunohistochemical staining exists but is now considered irrelevant and there are no recommendations for its verification by FISH. Despite the fact that +1 HER2 score is considered “low”, the protein expression exists however, its impact on the development of drug resistance or on the HER2 phenotype switch between primary tumor and its corresponding lymph node metastasis, as was previously reported in breast cancer, remains unknown (17). Recently the same variability was reported by Park and co-workers in gastric cancer who recommended repeating HER2 assessment for patients with advanced gastric cancer whose primary tumor was initially HER2-negative (18).
The aim of this study was to evaluate neglected aspects of HER2 assessment in bladder cancer, related to tumor type, grade and lympho-vascular invasion. In particular, we aimed to evaluate by FISH all cases assessed for HER2 overexpression by immunohistochemistry, independently from the IHC score. This may increase accuracy in the identification of HER2 positive cases and a better future stratification and selection of patients suitable for trastuzumab therapy.
Materials and Methods
Ethics approval and consent to participate. Ethics Commitee of Victor Babes University of Medicine and Pharmacy Timisoara approved the use of archival parraffin blocks and data regarding histopathology of the tumors for the present study.
Samples description. Fifty cases of archival paraffin embedded tissues of bladder cancer were selected. Cases were previously characterized regarding tumor type, T parameter, grade and presence of lympho-vascular invasion. Two independent histopathologists reviewed the cases and excluded five of them because of poor primary processing (not enough material or improper fixation highlighted by negative immunohistochemistry for Vimentin, clone V9). After re-evaluation, we performed a 3 μm serial section from each of the forty five cases to be used for immunohistochemistry and in situ hybridisation.
Immunohistochemical analysis. All steps of immunohistochemical staining were performed using a fully automated workflow provided by BOND Max Autostainer by using BOND™ ORACLE™ Human Epidermal Growth Factor Receptor 2 (HER2) Immunohistochemical System (Leica MicroSystems, NewCastle, UK) compatible for this automated system and approved by FDA in 2012.
In situ hybridisation was manually performed with PathVysion HER-2 DNA kit and VYSIS FISH probes, following the manufacturer's protocol (Abbott Molecular, USA). Briefly, the sections were dewaxed in xylene for 10 min at room temperature, treated with alchool and dried. These steps were followed by a pretreatment step using Preatreatment solution at 80° C for 30 min. Denaturation of specimens DNA was performed by immersion of the slide in the denaturing solution at 72±1°C for 5 min, followed by dehydration steps in alcohol succesive bathes with a gradually increasing concentration from 70 to 100%. Ten μl of probe mixing was applied to the target area of each specimen and the hybridisation step started by using Dako Hybridiser (DAKO, Cytomation, San Francisco, USA), for 18 h at 37°C. Post hybridisation step included staining with DAPI and storage of the slides in a dark place until used according to the manufacturer's instructions.
Data interpretation. For interpretation of both immunohistochemical and FISH results, we used the standardised scores applied for the assessement of HER2-positive breast cancer. We identified the concordance rate and discordances between IHC and FISH results and we carefully evaluated gene amplification in all cases, including +1 HER2 positive cases.
Statistical analysis was performed by using SPSS 17 software (IBM Corporation, New York, NY, USA) including correlation tests. A p-value of <0.05 was considered significant.
Results
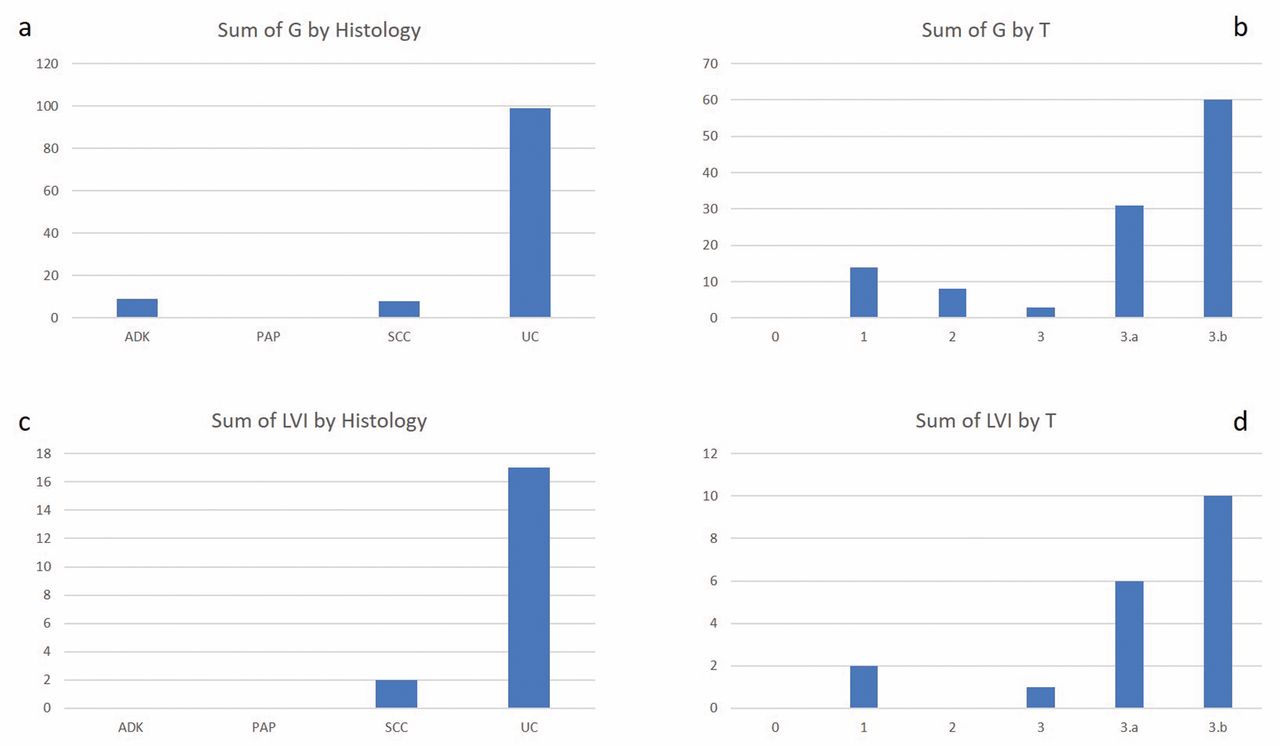
Pathology of the FFPE bladder specimens. Histopathology evaluation identified a study group composed of one bladder papilloma (2.22%), 3 squamous cell carcinomas (6.66%), 4 cases of adenocarcinomas (8.88%) and 37 cases of invasive urothelial carcinomas (82.23%). Except for the papilloma case, we assessed T parameter and grading (G) for each specimen. Staging of primary tumors (T) in bladder cancer identified T1 in seven cases (15.9%), T2 in 3 cases (6.82%), T3a in 12 cases (27.29%) and T3b in 22 cases (50%). Two cases were graded as G1, 12 cases as G2 and 30 cases had a G3 score. Nineteen (42.23%) out of 45 cases presented lympho-vascular invasion observed on routine stained specimens. All data are summarized in Figure 1 and overviewed statistical data are presented in Table I.
Assessment of HER2 overexpression by immunohistochemistry. All cases were analysed by immunohistochemistry for HER2 protein expression. We scored the membrane restricted expression. About one third of cases (31.12%) showed positive expression for HER2 oncoprotein scored as +2 and +3. Nineteen cases did not express HER2 (scored as 0) while 11 cases were evaluated as +1 HER2 (reported by all known scoring systems as being negative, too). From seven cases scored as +3 for HER 2 six were staged as T3A (3) or T3B (3), only one case being staged as T1. Cases scored as +2 for HER2 by immunohistochemistry (n=7) were staged as follows: 3 cases as T1, 3 cases as T3A and one case as T3B. Eleven cases were scored as having a +1 HER2 score assessed by immunohistochemistry. For this group, six cases were characterised as T3B, two cases as T3A and T2, respectively and one case as T1. A dynamic change was registered regarding correlation between lympho-vascular invasion and differential expression of HER2. In the groups considered as negative for HER2-IHC with a 0 score, less than 35 % of cases presented lympho-vascular invasion, and this percent abruptly increased to 54.54% for negative cases scored as +1. The percent of cases with lympho-vascular invasion increased up to 57.14% for +2 HER2 positive cases and slightly decreased in the +3 HER2 positive group to 42,85%.
Descriptive statistics of cases.
Case distribution according with HER2 score assessed by IHC and FISH respectively.
The papillary type of urothelial cancer had the highest and constant expression of HER2 by immunohistochemistry (all cases being positive), confirmed by a high (+3 HER2) gene amplification assessed by FISH.
Impact of concordances and discordances between IHC and FISH analysis in bladder cancer. Usually, for breast cancer, the recommendation to perform FISH is given only for cases scored as +2 by HER2-IHC. No precise recommendations and protocol interpretation is currently given for HER2 assessment in urothelial cancer. Few studies have applied FISH to all cases despite of their previous classification by HER2 immunohistochemical scoring. For urothelial cancer scattered data have suggested that FISH is superior to immunohistochemistry and recommend to be performed in all cases, but this is not widely accepted.
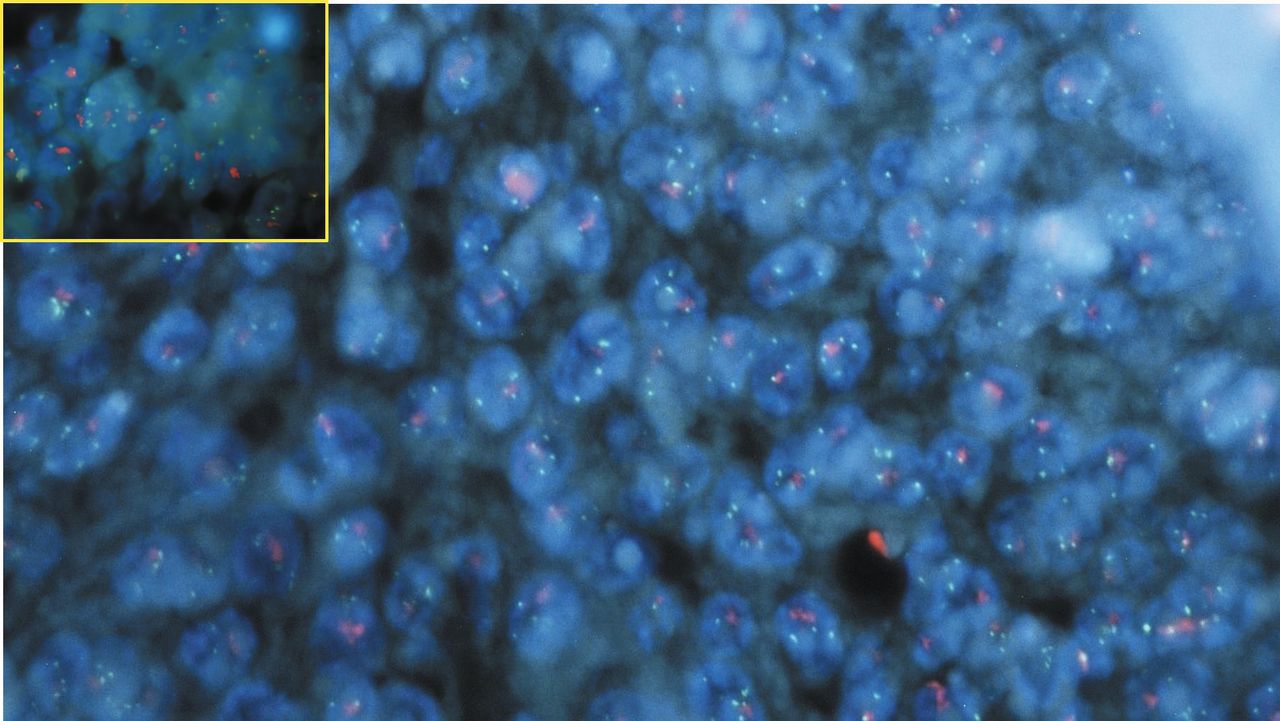
We performed FISH to all cases of urothelial carcinomas focusing on those which are grouped as 0 and +1 after HER2-IHC. Differences between IHC and FISH are summarized in Table II. Concordance between immunohistochemistry and FISH was registered in 33 cases (73,34%). The most unexpected finding was the distribution of another 12 cases regarding discrepancies between IHC and FISH. In the group scored as negative by IHC, we detected 6 cases having HER2 gene amplification by FISH. They represented about 31,57% of cases previously classified as negative by the use of immunohistochemistry, only. From these six cases, 4 showed high amplification noted as +2 and +3 by HER2-FISH scoring. In the cases with +1 HER2-IHC, 36,36% of cases had FISH amplification (from 4 cases, 2 had low amplification scored as 1 and another 2 had 2 or 3). Most of the researchers usually focus on the +2 HER2-IHC group, which is still controversial in HER2 evaluation even in other cancer types. In our study, all seven cases showed gene amplification by FISH (two cases with low amplification and other 5 being highly amplified, Figure 2). All cases from the +3 HER2-IHC group had high gene amplification by FISH (Table III).
Procentual distribution of concordances and discordances between IHC and FISH analysis.
Lymphovascular invasion (LVI) related with T parameter and IHC-HER2 score.

Graphical distribution of case numbers by their relationship with histology, G, T, and lymphovascular invasion (LVI).
{kind=link}
{kind=link}
Fluorescent in situ hybridisation confirmed gene amplification for cases scored as negative (score 0 and +1) for HER2 immunohistochemistry. The most intriguing cases were those with score 0 and high amplification detected by FISH as it happened for the present case.
Analysis of cases declared as negative based on protocols for IHC interpretation of HER2 and reclassified according to gene amplification assessed by FISH.
Based on FISH results we reclassified HER2 positive cases and the percent of positive cases increased from 31.12% (found by IHC) to 51.1% of cases.
Statistical analysis was performed between HER2-IHC and HER2-FISH, T parameter and G. A significant statistical correlation was found between T3 parameter and both HER2-IHC (p=0.05) and HER2-FISH (p=0.01). As observed from these data, correlation between T and HER2-FISH was significantly stronger compared with those between T and HER2-IHC. Case distribution according to T parameter, HER2-IHC score and lympho-vascular invasion are summarized in Table IV. It seems that HER2 has no influence on G parameter, this also being supported by the lack of a significant correlation between these two parameters in the present study.
Moreover, when we performed statistical analysis restricted to those 12 cases which were previously considered as negative IHC.HER2 score (0, 1) or score 2 but with amplification highlighted by FISH, we found that T3 parameter was strongly associated with lympho-vascular invasion (LVI) and FISH-IHC2 amplification, while histology proved to be correlated with IHC.HER2 overexpression only (Table V). When we exclusively analyzed cases classified as having score 0 by IHC we found that LVI is significantly correlated with FISH.HER2 amplification and not with IHC.HER2 score or any other parameters (Table VI).
Significant relationship between LVI and FISH.HER2 amplification for cases previously scored as 0 by IHC.HER2.
Discussion
Receptor tyrosine-protein kinase (RTKs) erbB-2 (CD340) is frequently known as HER 2. It is a proto-oncogene encoded by the ERBB2 gene in humans and is part of a large family of human epidermal growth factor receptors (together with HER1, HER3 and HER4) (19). Thirty years after its discovery and characterisation in breast cancer cells (20), HER2 represents a therapeutic target for more than 30% of metastatic breast cancer cases (21, 22) but the function of this receptor is not fully elucidated yet. The plasticity of this molecular target to form heterodimers not only with other members of the EGFR family but also with other related RTKs seems to be one of the mechanisms responsible for resistance development following specific treatment with humanized monoclonal antibodies against HER2 such as trastuzumab (23).
While for breast cancer there are already developed therapies able to decrease development of drug resistance and to improve the efficiency of targeted therapy against HER2 (24, 25), for other cancer types the expression and role of HER2 in progression and metastasis are not fully elucidated and thus a HER2 based therapy is not well accepted for gastric cancer for example (26).
Urothelial malignancies are among the most neglected cancers regarding the assessement of HER family members. All members of this group are reported to be expressed in urothelial cancer (27), but HER2 has been the most intensely studied, alone (28, 29, 30) or in combination with other HER family members, especially EGFR (31, 32). Several papers reported that HER2 positivity may predict muscle invasion in urothelial cancer of the urinary bladder (33, 34, 35). Based on previous studies regarding HER2 involvement in tumor progression from bladder cancer, this oncoprotein was included in newly designed multiplatform biomarkers designed to be used in clinical practice to predict invasion and reccurence in patients with urothelial cancer (36, 37, 38). Our data support the HER2 role in the local invasion of urothelial tumors, most of the cases scored as +2 and +3 being staged into T3 (a or b) group. Also, HER2 overexpression was correlated with an increase in the percentage of cases identified with lymphovascular invasion on histological specimens assessed in the present study. Our data were in concordance with the only paper found in the literature regarding the interconnection between HER2 overexpression and lymphovascular invasion. Bolenz and coworkers reported that HER2 positivity was significantly associated with the presence of lymphovascular invasion (39) and this oncoprotein overexpression was highly associated with an increased aggressiveness of the tumor and provided independent prognostic information for recurrence and mortality. A recent paper published by the same team (40) reported a complete remission of the urothelial carcinoma following third-line treatment with trastuzumab and gemcitabine in a patient with HER2 positive urothelial cancer initially unresponsive to cisplatin and vinflunine chemotherapies. These evidences are not widely accepted in the field of HER 2 research in urothelial carcinomas (41). Recent data reported that HER2 is overexpressed not only in primary urothelial cancers but also in their corresponding lymph node metastases (29, 42).
Based on previously published data and our own results, the study of the HER2 family in urothelial cancer seems to be a harder battle than cancer itself. There are currenlty more controversies than evidence for the use of HER2 as a therapeutic target in bladder cancer. Several reasons contribute to these unresolved issues in bladder cancer the most important of them being the unproper technical approach used for HER2 assessement together with a lack of a well standardised protocol of its interpretation specifically for bladder cancers overexpressing HER2. Our results sustain an extensive revision of HER2 assessement protocols in bladder based on criteria regarding immunohistochemical and in situ hybridisation use and interpretation as effective tools for HER2 validation as a molecular marker in urothelial cancer subtyping, an issue recently and frequently discussed (43, 44, 45).
Conclusion
New immunohistochemical and FISH protocols should specifically be designed for urothelial carcinomas. IHC should remain the first step in this evaluation. Our results showed that all cases scored as +2 and +3 by IHC were confirmed by FISH analysis having gene amplification and this may be considered a strong reason supporting the patient selection for anti HER2 therapy based on immunohistochemistry only. Negative and +1 HER2-IHC scored cases represent a questionable issue in urothelial carcinomas. Our data support the recommendation of FISH analysis for these groups which seem to be underscored by immunohistochemistry restricted analysis. Cases scored as negative by HER2-IHC but found positive by FISH analysis may explain phenotypic switch in HER2 expression between primary tumor (negative for HER2 by IHC) and corresponding lymph node metastasis (in some cases strongly positive for HER2 by IHC).
Acknowledgements
The Authors would like to thank Dr. Amalia Raluca Ceausu for her technical excellence and to Victor Babes University of Medicine and Pharmacy Timisoara, Romania for its continuous financial and administrative support. Present study was supported by funds kindly provided by Victor Babes University of Medicine and Pharmacy Timisoara, Romania, through P-III-C5-PCFI-2017/2018-03 Internal grant-acronym UROVESSELS.
Footnotes
Conflicts of Interest
No competing interests to declare.
- Received July 18, 2017.
- Revision received August 1, 2017.
- Accepted August 2, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved