

Abstract
The most promising near-term application of circulating tumor cells (CTCs) monitoring relates to the development of targeted cancer therapies, and the need to tailor such treatments to individual tumor characteristics. A high number of new innovative technologies to improve methods for detecting CTCs, with extraordinarily high sensitivity, have recently been presented. The identification and characterization of CTCs require extremely sensitive and specific methods that are able to isolate CTCs with the possibility of cultivation and downstream analysis of in vitro culture of separated CTCs. In this original research paper, we demonstrate that it is possible to isolate human CTCs from a patient with prostate cancer, with subsequent cultivation and proliferation in vitro. We show that the use of a filtration device implemented by MetaCell® can fulfil all the requirements mentioned above. Fifty-five patients with localized prostate cancer have so far been enrolled into the study. CTCs were detected in the blood samples of 28 (52%) out of the 55 patients. We report successful isolation of CTCs from patients with prostate cancer, capturing cells with a proliferative capacity in 18 (64.3%) out of the 28 CTC-positive patients. Direct correlation with Gleason score and T stage was not proven. The cells, captured by a size-based filtration approach, remain in a good state, unaffected by any antibodies or lysing solutions. During the filtration process, no interactions occurred between antibodies and antigens on the surface of CTCs. This biological interaction is specific for immunomagnetic methods. The MetaCell device provides the possibility of reaching virgin CTCs suitable for subsequent cultivation or single-cell analysis. This aspect will have an important impact on the future design of clinical trials testing new drugs against targets expressed on metastatic cancer cells. In addition to measurement of CTC counts, future trials with targeted therapies should also include the assessment of the specific therapeutic target on CTCs.
- Circulating tumor cells
- CTC
- prostate cancer
- cultivation
- minimal residual disease
- MetaCell
- virgin CTC
- biomarker
- culturing
- blood biopsy
Tumor cells can be detected in the peripheral blood by many newly-invented methods. These malignant cells in peripheral blood are described as circulating tumor cells (CTCs), originating from primary tumors or metastases. Prostate cancer was an early area of CTC research due to the presence of several prostate-specific proteins, including prostate-specific antigen (PSA) and prostate-specific membrane antigen.
A great number of new innovative technologies to improve methods for detecting CTCs, with extraordinarily high sensitivity, have recently been presented, including CTC microchips, filtration, quantitative reverse transcription polymerase chain reaction (RT-PCR). However, evidence has emerged that the currently used detection methods lack sensitivity or specificity to track all CTCs. Improvements in CTC capture efficiency, quantification, imaging, and molecular analyses are likely to bring further clinical applications.
The most promising near-term application of CTC monitoring relates to the development of targeted cancer therapies, and the need to tailor such treatments to individual tumor characteristics. The identification of tumor genotypes that inform selection of targeted therapies is usually performed on the initial diagnostic specimen.
Such targeted therapies aim to match the right drug to the right patient through stages of disease progression, from drug sensitivity to the acquisition of drug resistance. Longitudinal monitoring of CTC-derived genotypes may thus provide a non-invasive approach to identifying drug sensitivity- and resistance-associated markers, guiding therapeutic decisions.
The population of CTCs harvested from a peripheral blood specimen may, therefore, be enriched for such cancer stem cells or metastatic precursors. Detailed molecular and functional analysis of such rare cells may provide insight into the biology of cancer metastasis and identify novel therapeutic targets for the treatment and prevention of blood-borne cancer dissemination.
The identification and characterization of CTCs require extremely sensitive and specific methods that are able to isolate CTCs with the possibility of cultivation and downstream analysis of in vitro culture of separated CTCs. In this original research article, we demonstrate that is possible to isolate human CTCs from a patient with prostate cancer, with subsequent cultivation and proliferation in vitro. We provide evidence that the use of a filtration device implemented by MetaCell® can fulfil all the requirements described above.
Materials and Methods
Patients. To date, 55 patients with localized prostate cancer were enrolled into the study. The final diagnoses were defined from histopathology samples. Based on the informed consent the clinical data were collected from all participating patients. The patients' sample characteristics are shown in Table I. Peripheral blood (PB) was collected prior to surgery. For each patient, approximately 8 ml of venous blood was drawn from the antecubital veins and placed into S-Monovette tubes (Sarstedt AG & Co., Numbrecht, Germany) containing 1.6 mg EDTA/ml blood as an anticoagulant. The samples were processed at room temperature using an isolation procedure completed within 24 h after the blood draw.
The Ethics Committee of all participating Universities and Hospitals approved the study protocol according to the Declaration of Helsinki. All patients provided written consent.
CTC enrichment and culture. Recently, a size-based separation method for viable CTC enrichment from unclotted peripheral blood has been introduced (MetaCell®; MetaCell s.r.o., Ostrava, Czech Republic). The size-based enrichment process is based on the filtration of PB through a porous polycarbonate membrane (pores with 8 μm diameter). The minimum and maximum volume of the filtered PB may be adjusted up to 50 ml of fluid. As standard practice, 8 ml of PB from patients suffering with prostate cancer was transferred into the filtration tube. Successive blood transfer in several steps is preferred to prevent the blood clotting on the membrane filter. The PB flow is supported by capillary action of the absorbent touching the membrane filter. Afterwards, the membrane filter kept in a plastic ring was transferred into the 6-well cultivation plate, 4 ml RPMI media was added to the filter top and CTCs were cultured on the membrane in vitro under the conditions of standard cancer cell cultures (37°C, 5% atmosphere of CO2) and observed by inverted microscope. The CTCs were grown in fetal bovine serum (FBS)-enriched RPMI medium (10%) for a minimum period of 14 days on the membrane (Figure 1). The grown cells were analyzed by means of histochemistry [May-Grünwald staining (MGG), Figure 2] and immunohistochemistry using the specific antibodies to prove the cell origin [pancytokeratin 1–Fluorescein isothiocyanate (FITC) conjugated antibody (Sigma Aldrich Chemie Munchen, Germany), cytokeratin 7 antibody (Dako Denmark SA, Glostrup Denmark)] and nonspecific (4’,6-diamidin-2-fenylindol (DAPI) staining (see Figure 3).
Patients' characteristics and CTC examination results.
Alternatively, the enriched CTC fraction can be transferred from the membrane and cultured directly on any plastic surface or a microscopic slide.
Cytological analysis. Each immunostaining experiment included positive control (a positive cell line stained with the specific antibody). The fixed and stained cells on the membranes were examined using light microscopy in two steps: for detailed cytomorphological analysis (×40 magnification). Isolated cells or clusters of cells of interest (immunostained or not) were selected and examined by an experienced researcher or pathologist. CTCs were defined as cells presenting the following: (a) nuclear size of 10 μm or larger; (b) irregularity of the nuclear contour; (c) presence of a visible cytoplasm; (d) prominent nucleoli; (e) high nuclear:cytoplasmatic ratio; (f) plasticity/deformability (growth through the membrane and setting up of new colonies).
Results
Fifty-five patients with diagnosed localized prostate cancer were included in the study. The basic characteristics of the study cohort are shown in detail in Table I. The mean age of the study population was 64 years (range=45-76 years). The pathological and CTC results for the study cohort are detailed in Table I. All tumors in patients were N0, M0, with 65.4% (n=36) of cases being pT2c.
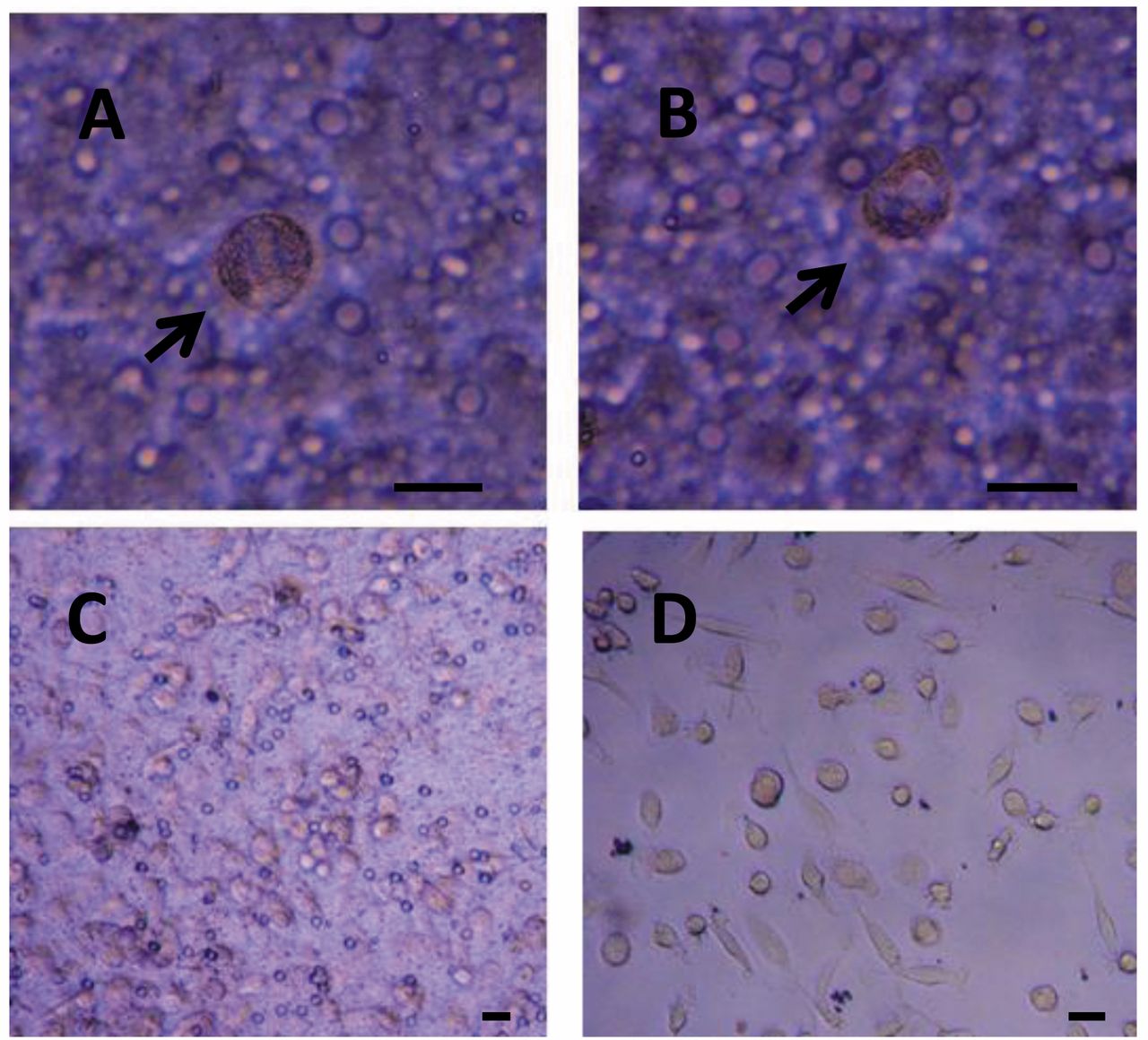
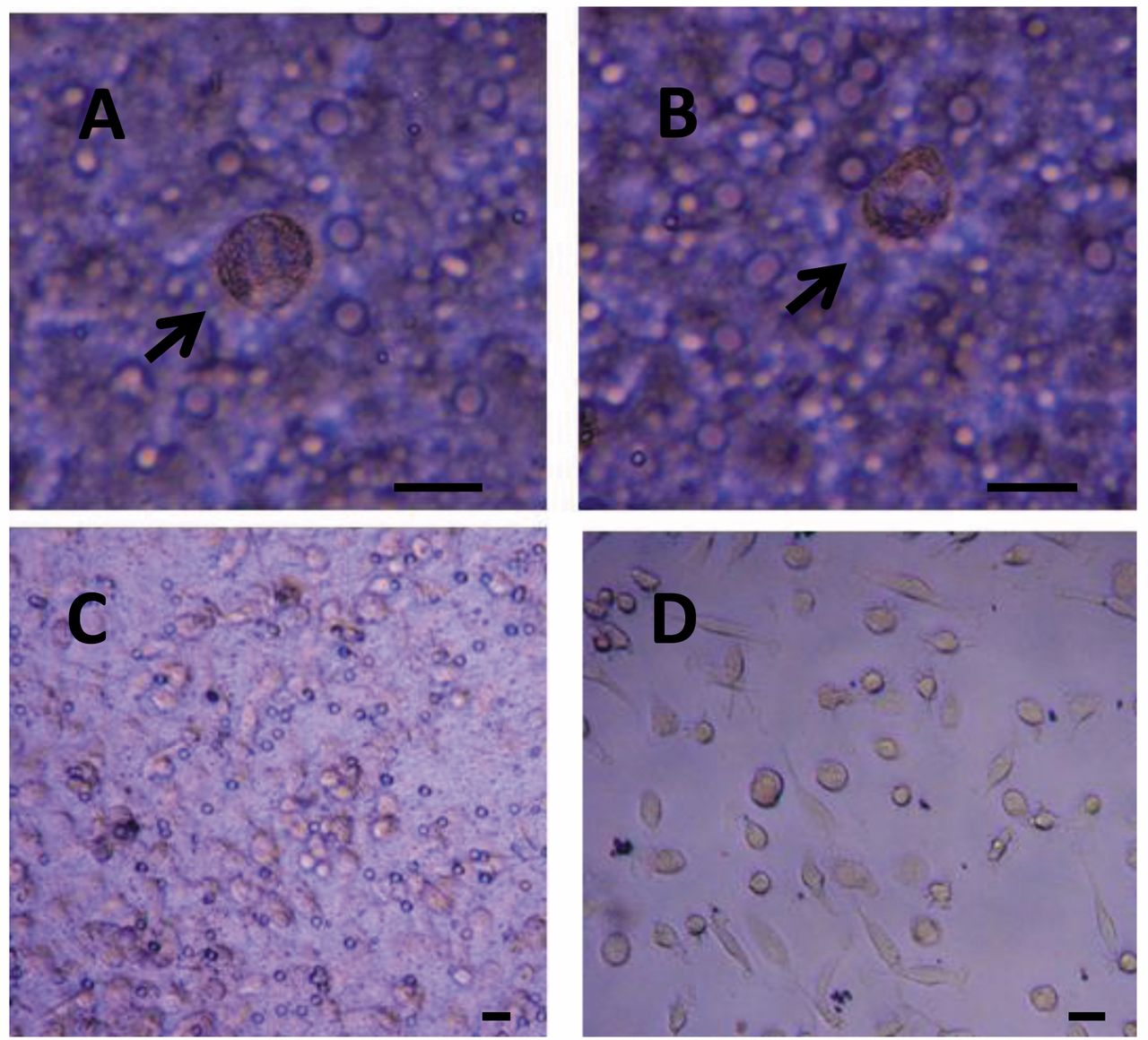
Living circulating tumor cells (CTCs) captured from a patient with prostate cancer 4 h after size-based enrichment on the membrane indicated by arrows (A, B). CTCs after in vitro culture (14 days) on the membrane (C) and growing on the well bottom (D). The bar represents 20 μm.
CTCs were detected in the blood sample of 28 (52%) out of the 55 patients (Table I). The frequency of the CTC positivity is summarized for different T stage sub-groups in Table I. No direct correlation with Gleason score was found (Table I).
We report successful isolation of CTCs in patients with prostate cancer, capturing cells with a proliferative capacity in 18 (64.3%) out of the 28 CTC-positive patients. The cells captured by size-based filtration approach were in a good condition, unaffected by any antibodies or lysing solutions. The CTCs were cultured in vitro for further downstream applications for 7-28 days.
The size of the cells guided us in the process of cancer cell identification even without any additional staining (e.g. MMG). But this standard staining method (MGG) enabled us to identify and analyze the nuclei with nucleoli. Generally, the nucleus itself is bigger than 10 μm and the cells do not present much cytoplasm. The nuclear:cytoplasmatic ratio is relatively high in cancer cells, but this is not the case under in vitro conditions. The CTCs become large and long when in culture, changing the nuclear:cytoplasmatic ratio. The cytoplasm of CTCs is rather pale than dark.
Due to the cell size (>15 μm), nucleus size (>10 μm) and shape and expressive nucleoli visualized by simple DAPI stain in the formerly fixed cells, we were able to detect cancer cells not only on the separating membrane (Figure 1A-C), but also on the plastic bottom of the 6-well plate (Figure 1D). These results indicate that the captured cancer cells display plasticity, enabling them to grow over the separating membrane. Reflecting the shape of the cancer cells in the ‘bottom’ fraction, we may expect that these cells present a fraction of more invasive CTCs. The immunohistochemical analysis showed the abundance of cytokeratin in the ‘membrane’ fraction as well as in the ‘invasive’ fraction, proving the carcinoma origin. We see an enormous potential in gene expression analysis, which, based on the RNA, could reveal the epithelial–mesenchymal character of the detected cancer cells.

Circulating tumor cells (CTCs) captured from a patient with prostate cancer, stained by May-Grunwald stain. A: CTCs growing on the membrane after 14 days in in vitro culture. B: CTCs growing through the membrane on the well bottom after 14 days in in vitro culture exhibiting two different phenotypes, epithelial-like and stem cell-like. Stem cell-like cells form visible cell clumps (see arrows). C: CTCs growing on the membrane after 14 days in in vitro culture. D: CTCs growing through the membrane on the well bottom after 14 days in in vitro culture. An arrow indicates a nucleus with a prominent nucleoli. The cells growing on the bottom exhibit very plastic morphology. The bar represents 20 μm.
Discussion
In our previous animal study, we used magnetic-based separation methods to enrich tumor cells from PB and to set up in vitro cultures (1). The basic principle of these methods is the use of immunomagnetic beads that are bound to antibodies: epithelial cell adhesion molecule (EpCAM), PSA or cytokeratins. For separation of CTCs of human prostate cancer, we used a size-based method because all EpCAM-based enrichment systems share the same limitation; EpCAM expression can be down-regulated during the epithelial-to-mesenchymal transition and there are significant differences in EpCAM expression even in the same type of tumors, including prostate cancer (2). Recent research indicates that this transition might affect tumor cells with stem cell-like properties in particular (3).
PSA is also highly expressed in benign and malignant prostate epithelial cells, which is why it is generally thought of as being prostate-specific (4), but its expression has also been reported in non-prostate tissues such as the pancreas, breast, endometrium, salivary gland, and normal and neoplastic female paraurethral ducts (5). Expression of mRNA for PSA has been shown to be androgen-dependent and to be decreased in more poorly differentiated tumors (6).

{kind=link}
{kind=link}
{kind=link}
Circulating tumor cells (CTCs) isolated from a patient with prostate cancer after in vitro culture (7 days), stained by specific cytokeratin cocktail Pan-cytokeratin 1–FITC and non-specific DAPI. Prominent nucleoli can be seen in the nuclei. The bar represents 10 μm.
PSA is not an ideal marker of treatment response in patients with castration-resistant prostate cancer (CRPC). The question then is whether monitoring CTCs is superior to following changes in PSA levels over time.
In a study on patients with CRPC, post-treatment CTC numbers were a stronger prognostic factor for survival than a 50% decline in PSA (receiver operating characteristic area under the curve: 0.87 vs. 0.62), and the authors suggested that CTC numbers measured at four or eight weeks of therapy can discriminate between favorable and unfavorable outcomes (7). In this case, monitoring CTCs was not only superior to PSA in yielding prognostic information but to also significantly improve models to predict overall survival among patients with metastatic CRPC (8).
CTCs that emanate from solid tumors have a larger diameter and volume than other hematological cells found in the circulation. A portable filter-based device achieved 90% capture efficiency from blood spiked with a prostate cancer cell line and found that it enriched more prostatic CTCs from more patient samples than did the Food and Drug Administration approved CellSearch™ device (9). Experiments with alternative enrichment methods highlight the poor sensitivity of the immunomagnetic techniques, with multiple studies demonstrating the significantly higher capture rates of size-based methods from patients with metastatic CRPC (10). Thus, size-dependent filtration may underestimate the true number of CTCs in a given patient's blood sample.
The most important advantage of filtration methods is the possibility to reach ‘virgin’ CTCs. During the filtration process, no interactions occur between antibodies and antigens on the surface of CTCs. This biological interaction is specific for immunomagnetic methods. The MetaCell device provides the possibility of reaching virgin CTCs suitable for subsequent cultivation or single-cell analysis. This aspect will have an important impact on the future design of clinical trials testing new drugs against targets expressed on metastatic cancer cells. In addition to measurement of CTC counts, future trials with targeted-therapies should also include the assessment of specific therapeutic targets on CTCs.
The presence of CTCs is a known independent prognostic factor for shorter metastasis-free survival (11). Interestingly, there is no significant correlation between the CTC count and the response of the primary tumor to chemotherapy, which is usually used as an indicator of treatment response (12). These results might be explained by the discovery that CTCs can be different from cells of the primary tumor in terms of their genome and protein expression patterns.
Molecular and chemosensitivity analyses will provide new insights into the biology of metastasis only with the possibility of using virgin CTCs or virgin CTC lines for further in vitro experiments.
Acknowledgements
This study was supported by a research grant of the Czech Ministry of Health: IGA NT14441-3/2013 and by a research grant of the Wroclaw Medical University ST-325.
- Received February 26, 2014.
- Revision received May 5, 2014.
- Accepted May 6, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved