

Abstract
Aim: We undertook a prospective phase II study to evaluate the efficacy of S-1 plus trastuzumab combination regimen for human epidermal-growth factor receptor-2 (HER2)-positive metastatic breast cancer (MBC). Patients and Methods: HER2-positive MBC patients received oral administration of S-1 (80 mg/m2/day, days 1 to 28, every 6 weeks) and intravenous weekly trastuzumab (2 mg/kg), according to the results of a prior Phase I trial of our group. Results: A total of 28 patients were enrolled and received a median of 3.5 (range 1-10) cycles of treatment. Overall response rate and clinical benefit rate were 53.6% and 75.0%, respectively. Progression-free survival was 30 weeks. With regard to grade 3 and 4 adverse effects, leucopenia, neutropenia, increase in serum alanine aminotransferase, and diarrhea were observed. Conclusion: Combination of S-1 and trastuzumab was tolerable and had excellent efficacy with good response and disease control in this trial.
- HER2-positivity
- metastatic breast cancer
- S-1
- trastuzumab
- first-line therapy
Trastuzumab, a humanized monoclonal antibody against the extracellular domain of human epidermal growth factor receptor type-2, has shown high clinical efficacy in combination with cytotoxic agents for HER2-overexpressing breast cancer. After this agent was approved, prognosis of the patients with HER2-positive advanced or metastatic disease has become superior to that of estrogen receptor-negative disease (1).
According to the Japanese Breast Cancer Society guidelines (2) and National Comprehensive Cancer network guidelines (3) chemotherapy is recommended for advanced or metastatic breast cancer that is refractory to hormonal therapy. The first and second choices of cytotoxic agents are either anthracyclines or taxanes. The options for the third-line or later treatment comprised of capecitabine, S-1, vinorelbine, irinotecan, gemcitabine, and eribulin. For HER2-positive disease, paclitaxel was the first established cytotoxic agent to be combined with trastuzumab (4). In vitro studies demonstrated additive antitumor effect of the combination with docetaxel, vinorelbine, platinum derivatives as synergistic effects, however fluorinated pyrimidine showed antagonistic effect (5). A similar pre-clinical study using a xenografted HER2-positive tumor demonstrated less effect when trastuzumab was combined with fluorinated pyrimidine agents, therefore, this combination was not commonly used in upfront lines, and clinical data has not been sufficient (5).
Capecitabine combined with trastuzumab was investigated in a prospective analysis of 40 consecutive heavily-treated patients as salvage therapy. Contrary to the in vitro tests (5), clinical outcome of patients treated by the capecitabine-plus-trastuzumab regimen in this study demonstrated a favorable effect of 20% in overall response rate (ORR) and 70% in clinical benefit rate (CBR) with acceptable toxicity (6).
Encouraged by this result of capecitabine, another fluorinated pyrimidine agent S-1 was highlighted as a promising cytotoxic companion for trastuzumab. S-1 was originally developed for the treatment of gastrointestinal tract cancers and has been widely used in Asian countries including Japan, especially as the key drug for the treatment of gastric cancer both in advanced (7, 8) and adjuvant setting (9).
In vitro studies of S-1 in combination with trastuzumab have already shown its favorable efficacy against several cancer cell types (10, 11). In a clinical setting, the result of our phase I trial demonstrated that the trastuzumab-plus-S-1 regimen had fewer serious or unpleasant adverse events, such as alopecia, nausea, vomiting, and febrile neutropenia, compared to other cytotoxic regimens commonly combined with trastuzumab (12). Based on the findings of this phase I study, we underwent the present phase II trial to test the clinical efficacy of S-1 in combination with trastuzumab for metastatic breast cancer (MBC).
Patients and Methods
Patients. Patients with inoperable or recurrent breast cancer from 12 participating Institutions were enrolled in the study, to be treated with S-1 in combination with trastuzumab from February 2007 to February 2012.
A total of 37 assessable patients were required to test the null hypothesis that the true confirmed response rate is at most 30% versus the alternative that it is at least 50%.
Unfortunately, analysis at the point in time was urged by independent data monitoring committee because the accumulation of the cases did not reach to the projected numbers at 5 years after the initiation of the trial.
Women aged ≥20 years with a histological or cytological diagnosis of HER-2-positive (IHC 3+ or IHC 2+/FISH+) MBC were considered to be eligible for the trial. Eligibility required measurable cancer by RECIST criteria version 1.1 (13): baseline left ventricular ejection fraction (LVEF) >55%; an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0-2; expected survival >6 months; adequate organ function defined as hemoglobin >9 g/dl, leukocyte count 3,000-12,000/mm3, neutrophil count >1,500/mm3, platelet count >100,000/mm3, serum total bilirubin level less than the upper level of normal in each institution x1.5, and serum creatinine level less than upper limit of normal. Treatment within one prior chemotherapy regimen was permitted for those with metastatic disease.
Patients with any of the following were excluded: lung metastasis with dyspnea; brain metastasis with symptoms; a second primary cancer; serious concomitant illness; cardiac abnormalities; or cases with possible infection. The protocol was reviewed and approved by the Institutional Review Boards at all participating centers. Written informed consent was obtained from all the patients.
Treatment. Patients received S-1 in combination with trastuzumab according to the recommended dose defined by the phase I trial (12). Trastuzumab was administered intravenously every week. The first dose was 4 mg per kilogram (kg) of body weight and the subsequent doses 2 mg per kg, administered over periods of 90 and 60 min, respectively. S-1 was administered in a daily dose of 80 mg/m2 orally, divided two after meals for 4 weeks, followed by a 2 weeks rest as one course. Study treatments continued until disease progression, appearance of unmanageable toxicity, or patients' request to withdraw from the study.
Safety. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 (14). Hematology and biochemistry assessments were performed before the start of each treatment cycle. LVEF was monitored by echocardiography at least every 12 weeks. Chemotherapy dose adjustments were allowed. Trastuzumab toxicity was managed by treatment interruptions.
Efficacy. The primary end-points were ORR and CBR, that were evaluated according to the RECIST criteria version 1.1 (13) until disease progression. ORR was defined as the proportion of all patients with complete response (CR) and partial response (PR). CBR was defined as the proportion of the patients with CR+PR +stable disease (SD) continued longer than 24 weeks. CR and PR required confirmation at least 4 weeks after first being reported.
The secondary end-points are overall survival (OS); progression-free survival (PFS); safety profile; CBR; and health related quality of life (HRQOL). HRQOL was accessed before starting the chemotherapy and every each course of the chemotherapy by EORTC QLQ-C30 questionnaire (15). The data of each questionnaire were processed along the EORTC QLQ-C30 scoring manual (16).
Results
Patients' characteristics. A total of 28 patients were enrolled. A completed survey form was collected from all patients. All patients were treated with a fixed dose (initial dose: 4 mg/kg, maintenance treatment dose: 2 mg/kg) of trastuzumab in combination with 80 mg/m2/day of S-1. The baseline clinical characteristics are summarized in Table I. The median age was 62 (range 45-78) years. Eight patients had distant metastasis when breast cancer was first diagnosed, and 20 patients had recurrent breast cancer. Fifteen patients had hormonal receptor (HR)-positive (ER+ and/or PR+); 13 patients had HR-negative tumors. The sites of metastatic disease were the bone and/or soft tissues in 24 patients and visceral sites in 17 patients, including duplication. The majority of patients (n=23) received S-1+ trastuzumab treatment as first-line therapy for MBC. Only 2 patients received cytotoxic chemotherapy and 3 patients received trastuzumab monotherapy before registration. Nine patients received endocrine therapy for MBC before registration.
Baseline patient characteristics (N=28).
Efficacy measured by response rate and clinical benefit rate. All the patients had measurable lesions and received the recommended dose according to the result of the phase I trial (12). Three patients achieved CR, 12 patients showed PR, and 10 patients showed SD (6 patients longer than 24 weeks and 4 patients shorter than 24 weeks). A patient resulted in progression without response and 2 patients could not evaluate the efficacy. Therefore the ORR was 53.6% (15/28), and the CBR was 75.0% (21/28) (Table II). In the sub-group of patients without previous cytotoxic chemotherapy for MBC, ORR was 74.3% (15/21). These results of the primary end-points indicate that the combination therapy regimen was highly effective to HER-2-positive breast cancers, especially for patients who had never received cytotoxic chemotherapy for metastatic disease. No difference was demonstrated between the HR positive sub-group and negative sub-group (HR +; CR 1, PR 6, SD 5, PD1. HR–; CR 2, PR 6, SD 5, PD 0, NE 2).
Tumor response (N=28).
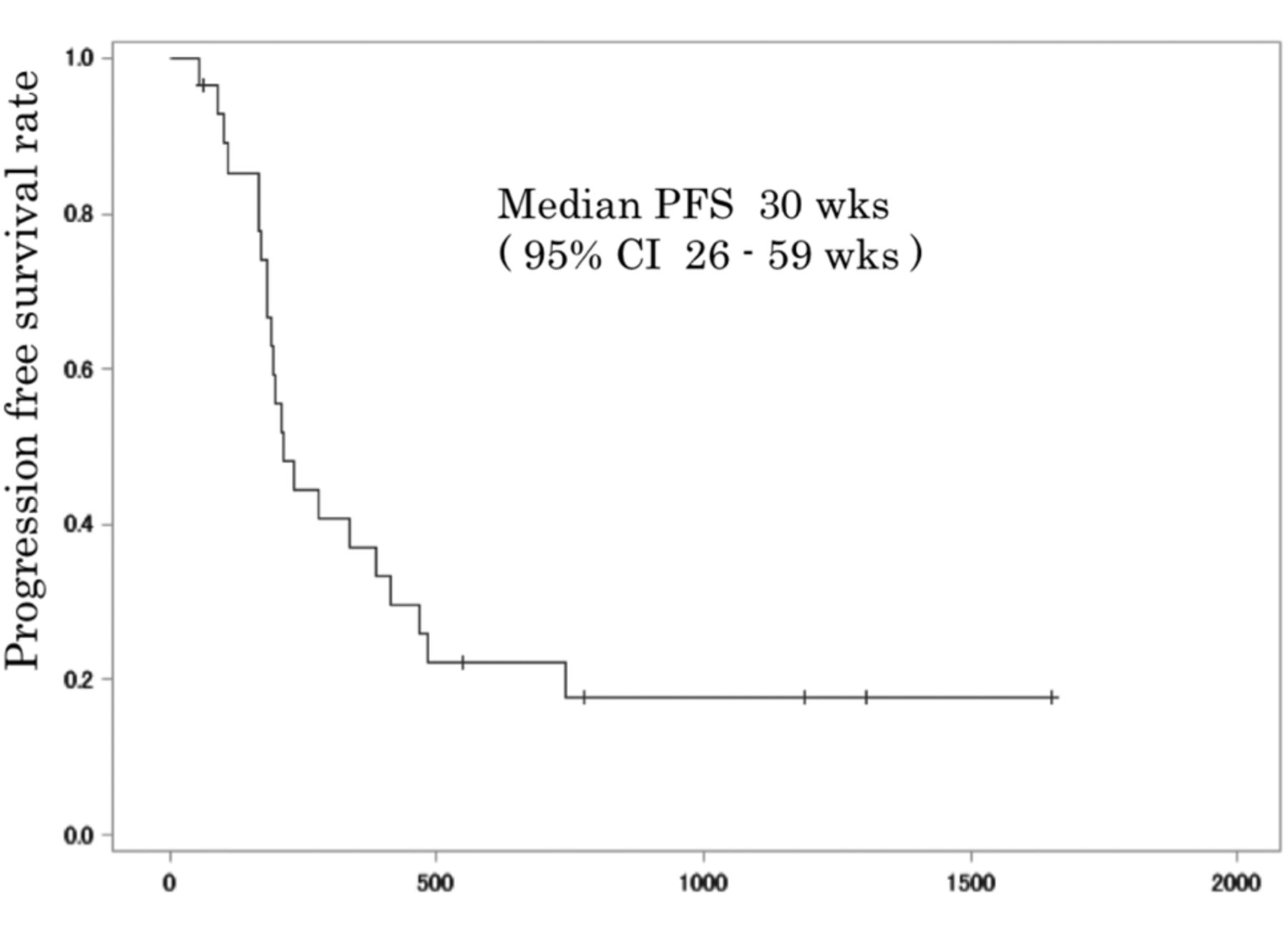
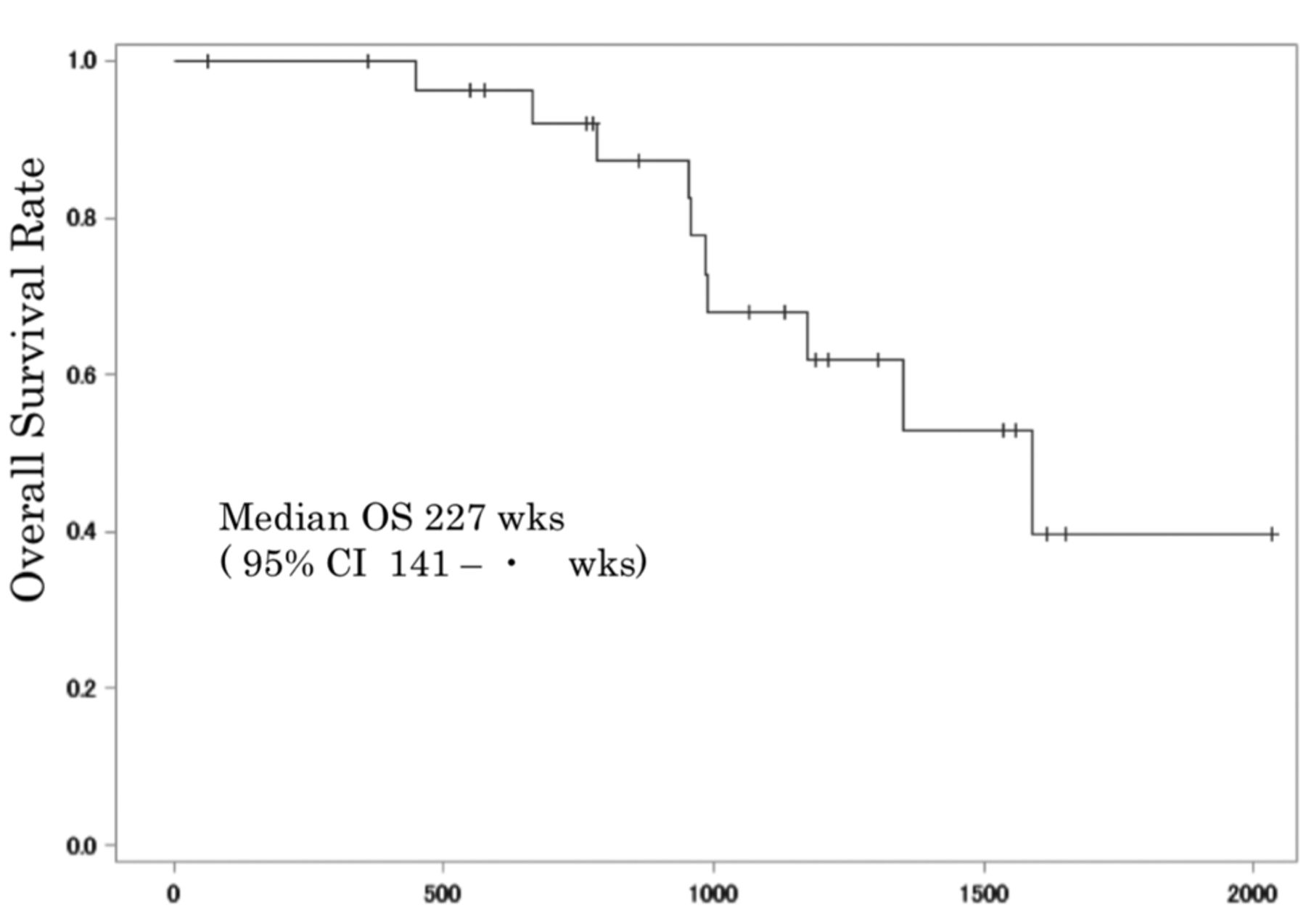
Prognosis estimated by overall and progression-free survival. By the time of data cut-off, PFS events had been observed in 22 patients (79%). Median PFS was 30 weeks (95% CI=26-59 weeks) (Figure 1). Nine out of 10 patients died from breast cancer. Median OS was 227 weeks (95% CI= 141-∞ weeks) (Figure 2).
Toxicity. All the patients were assessed for toxicities during the treatment cycles. No grade 4, and a few grade 3 toxicities were observed in all enrolled patients. Although Grade 3 hematological toxicities were observed in 7 patients including leukopenia and neutropenia, they were not critically severe. With regard to non-hematological toxicities, the most common events were nausea, diarrhea, and elevation of serum alkaline phosphatase. The hematological and non–hematological events in all the 28 patients are listed in Table III.
Clinical benefit response and health-related quality of life. Sixteen patients cooperated with the first and the later questionnaire survey. In this QLQ-C30 questionnaire, Osoba et al. (17) reported that the patients who reported ‘very much’ change for better or worse on a particular scale corresponded to a change greater than 20. Our study demonstrated the patients who showed improvement of QOL with reduction of score more than 20 points were 6.3% in physical function, 12.5% in role function and emotional function, 18.8% in cognitive function, 25% in social function and 0% in general health status.
Discussion
Although the most important objective of metastatic breast cancer treatment is to prolong survival with good patients' QOL (18), chemotherapeutic agents have been chosen in the order of their effectiveness for shrinking tumors, rather than their intensity of side-effects. In line with this objective, less toxic treatment should be chosen in up-front line as long as the treatment could control disease progression. Generally, response and duration of efficacy of the chemotherapeutic agent are better when it administered in up-front line than late line. Therefore, the patients can have more comfortable lifetime if they responded to less toxic therapy. By such a viewpoint, SELECT BC trial that compares OS of the HER2-negative metastatic breast cancer patients administered S-1 or taxanes as the first chemotherapy is ongoing in Japan (19). This study may give a solution for this issue.

Kaplan–Meier Estimates of Progression-free Survival Rates. Bars represent patients whose data were censored.
The present study strongly suggests that combination therapy with S-1 and trastuzumab appears to be an effective treatment option with a manageable toxicity profile for MBC. Efficacy rates of S-1 alone for MBC patients were 21.8% and 41.7% in two Japanese phase II trials (20, 21) and 30% in a retrospective study (22), S-1 is expected to be one of the promising fluorinated pyrimidines for the treatment of breast cancers. It should be emphasized that the rate may improve when the agent is applied at an up-front line of the treatment sequence. Sub-group analysis of the patients who were treated with S-1 relatively early, i.e. in the first and second lines, showed response rates as high as 45.5% (22). This result is compatible to the efficacy rate of taxanes that were used as the standard therapy in first line. Additionally, compared with anthracyclines and taxanes, adverse events such as hair loss are significantly rare, and its oral dosage form is supposed to be helpful in improving QOL of the patients. Actually, the patients whom HRQOL score decreased were few in this series. This result suggested that the combination of S-1 and trastuzumab was useful for maintenance of HRQOL.

{kind=link}
{kind=link}
Kaplan–Meier Estimates of Overall Survival Rates. Bars represent patients whose data were censored.
Common adverse events in the enrolled patients (N=28).
Although capecitabine is another orally-available fluorinated pyrimidine anticancer agent and its efficacy has also been proved by several phase II studies (23, 24), its toxicity profiles are different from those of S-1. Results of a randomized phase II trial comparing these two agents for gastric cancer demonstrated almost identical efficacy but high incidence of hand-foot syndrome and stomatitis decrease the dose intensity of capecitabine in comparison with S-1 (25).
A combination of capecitabine and trastuzumab in HER2-positive breast cancer after failure of previous trastuzumab-containing regimen was investigated in randomized phase III study. One hundred and fifty-six patients were enrolled in the trial, and the combination of trastuzumab and capecitabine showed survival benefit against capecitabine monotherapy although no significant difference was demonstrated (26). Another clinical trial investigating the efficacy and feasibility of the combination regimen after failure of anthracyclines and docetaxel or vinorelbine demonstrated good response rate and favorable impact for prognosis for heavily pre-treated MBC (6).
With regard to S-1 and trastuzumab combination regimen, several case studies reported efficacy of the regimen in heavily pre-treated HER2-positive MBC including trastuzumab treatment in their prior therapy (27-30). According to those anecdotal reports, S-1 in combination with trastuzumab indicated outstanding effects on heavily pre-treated patients without serious toxicity. In a large retrospective study which enrolled 1,468 breast cancer patients, whole adverse events and grade 3 or 4 adverse events of the combination therapy were occurred in 55.9% and 16.1%, which is comparable to that of S-1 alone, 63.5% and 14.6%, respectively (31). Like our result of the phase I trial, toxicity profile of the S-1 plus trastuzumab combination seems to be acceptable.
The present study was in line with previous reports in terms of the safety of the regimen. Our report is the result of the first prospective clinical trial evaluating efficacy of the S-1 plus trastuzumab combination regimen for MBC. With regard to the efficacy of the combination regimen, an ORR of 53.6% and an CBR of 75.0%, obtained from this phase II study should give a strong support to apply this regimen for a common clinical practice.
In conclusion, combination of trastuzumab and S-1 is an effective regimen with feasible toxicity and valuable to maintain patient's HRQOL. This combination therapy can be considered as a new standard option of the first- or second-line chemotherapy in patients with HER2-positive MBC.
Acknowledgements
This work was supported, in part, by a non-profit organization Epidemiological & Clinical Research Information Network (ECRIN). The Authors are grateful to Ms. Mai Hatta for her excellent data management as the clinical research coordinator.
Footnotes
-
This article is freely accessible online.
-
Conflicts of Interest
Tsutomu Takashima and Yasuo Miyoshi have received grants from Taiho Pharmaceutical Co. Ltd.
- Received February 20, 2014.
- Revision received May 8, 2014.
- Accepted May 9, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved