

Abstract
Aim: We investigated effects of gemcitabine-based adjuvant chemotherapy (GEM) on prognosis of patients with gallbladder cancer. Patients and Methods: We retrospectively analyzed outcomes of 36 patients who underwent radical resection for gallbladder cancer from 2001 through to 2012, using χ2 for prognostic factors and Kaplan–Meier estimator and log-rank tests for survival data. Results: The GEM group had higher rates of lymph node positivity and distant metastasis, higher UICC stage and fewer R0 resections; their 5-year survival rate (60%) did not significantly differ from that of the controls (70.0%), nor was GEM a significant prognostic factor in univariate analysis. However, among patients who underwent R1 and R2 resections, GEM significantly improved prognosis in both univariate and multivariate analyses. Median survival of the R1/2 GEM group (66.4 months) was significantly better than that of controls (5.4 months) (p=0.002). Conclusion: GEM improved prognosis of patients with gallbladder cancer after R1/R2 resections.
- Gallbladder cancer
- curability
- gemcitabine (GEM)
- adjuvant chemotherapy
The efficacy of adjuvant chemotherapy for gallbladder cancer is currently unclear. Few studies have described the effect of adjuvant chemotherapy on biliary tract cancer (BTC) (1, 2), and only one phase III trial of adjuvant chemotherapy for BTC patients has been published. Clinical BTC research is limited by the small number of patients, and by the variety of cancers (bile duct, gallbladder and ampulla vater) which may differ in biological character (2). In this retrospective study, we focused exclusively on gallbladder cancer, and the therapeutic role of GEM in treating it.
Patients and Methods
Patients. We retrospectively analyzed survival and characteristics of 36 patients who underwent radical resection for gallbladder cancer at the Kawasaki Medical School from 2001 to 2012. All patients gave their informed consent for surgical treatment. Out of these 36 patients, 7 underwent GEM with or without other drugs. Five of 7 patients underwent GEM monotherapy (six 28-day cycles: 1,000 mg/m2/day gemcitabine on days 1, 8, and 15) (3). One of the 7 patients was treated with GEM and S-1 (each 21-day cycle: 1,000 mg/m2/day gemcitabine on day 1 and 8; 60-100 mg/body oral S-1 according to body-surface area (<1.25 m2, 60 mg/day; 1.25≤to<1.5 m2, 80 mg/day; ≥1.5 m2, 100 mg/d) on days 1 through 14)(4). Another of the 7 patient was treated with GEM and cisplatin (each 21-day cycle: cisplatin 25 mg/m2 followed by gemcitabine 1,000 mg/m2 on days 1 and 8) (5-7). 11 patients out of the 36 patients, 11 underwent R1 or R2 resections according to UICC definition (8). The mean follow-up period of this study was 29.7 months.
Statistical analysis. Statistical analysis and graphical presentations were performed with JMP 9 software (SAS Institute, Cary, NC, USA). Patients' characteristics were analyzed using the Mann–Whitney U-test and χ2 test. Significance of prognostic factors was analyzed by χ2 estimators of the proportional hazard model. Survival curves were constructed using the Kaplan–Meier product-limit method and were compared using the log-rank test. p<0.05 was considered statistically significant.
Results
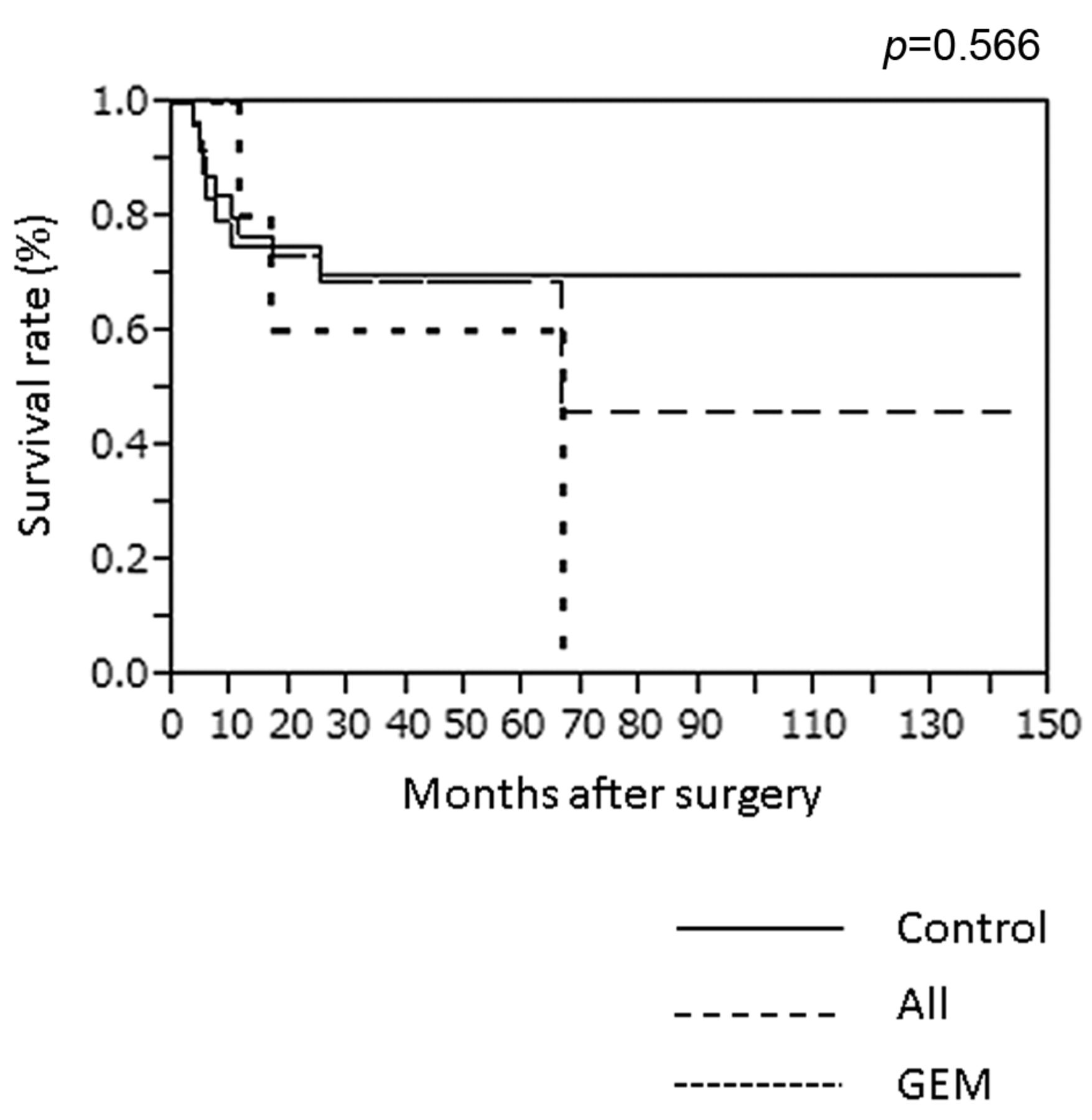
Patients' characteristics. Patients treated with GEM (GEM group) showed higher UICC stage (p<0.001), higher rates of lymph node metastasis (N1, p=0.004), distant metastasis (p=0.003), peritoneal metastasis (p=0.031) and liver metastasis (p=0.003), and a lower rate of R0 resection (p=0.009), than patients who did not receive adjuvant chemotherapy (control group) (Table I) (8). Despite the advanced stage of disease in the GEM group, the two groups did not significantly differ in overall survival rate (OS), with 5-year survival rates of 60.0% for the GEM group and 70.0% for the control group (p=0.566; Table I and Figure 1).
Patients' characteristics.
Univariate and multivariate analyses. We performed univariate and multivariate analyses of prognostic factors for 36 patients (Table II). Lower R0 resection rate, higher clinical stage, higher T-factor and positive lymph node metastasis (N1; as defined by UICC) were found to significantly predict worse prognosis by univariate analysis (8); out of these, higher T-factor and lymph-node metastasis were found to significantly predict worse prognosis by multivariate analysis (Table II). GEM was not a significant prognostic factor for the 36 patients (Table II).
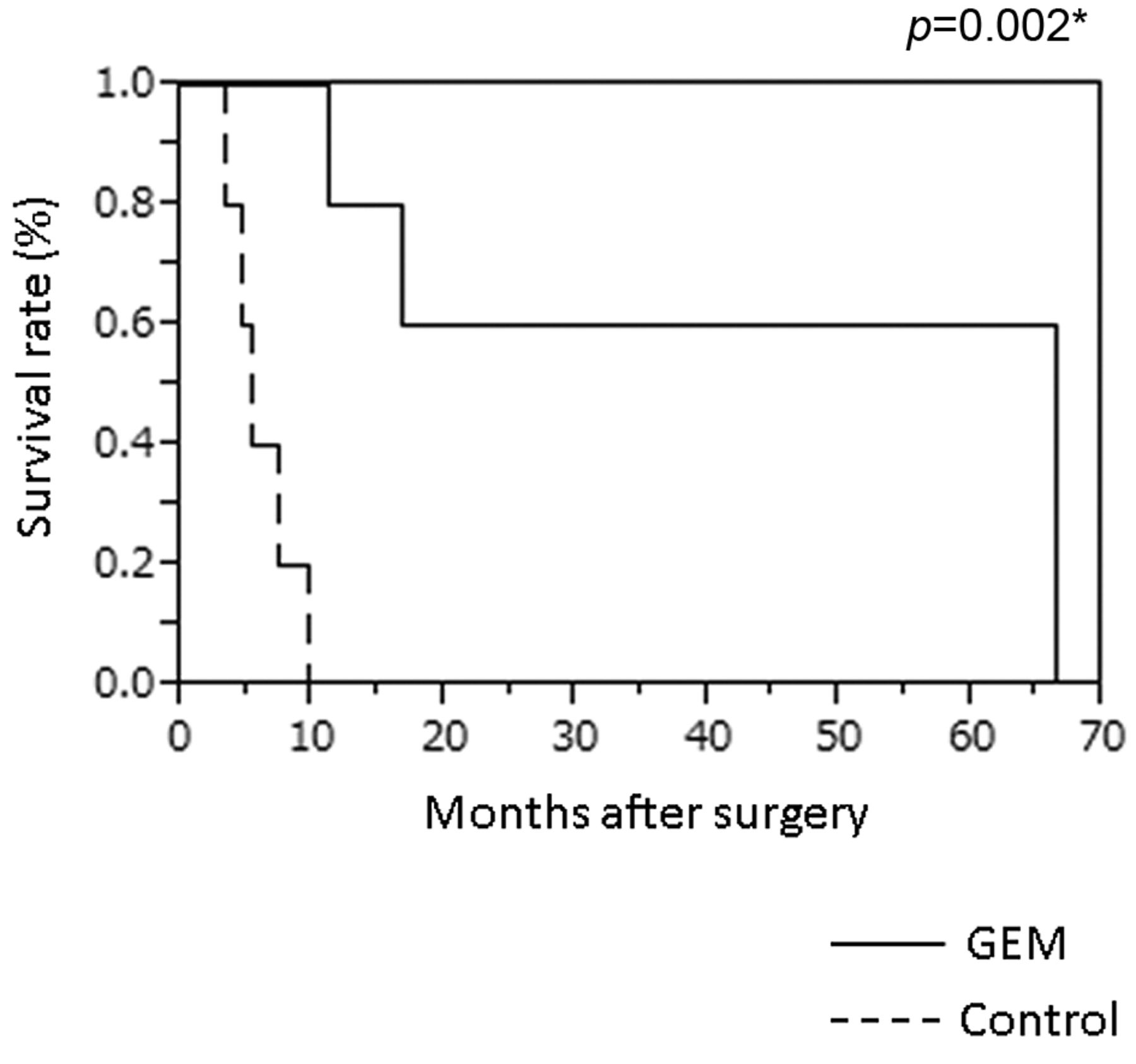
Univariate and multivariate analyses of prognostic factors for patients who underwent R1 and R2 procedures. Univariate and multivariate analyses for patients with R1 and R2 procedures. In univariate analysis of prognostic factors for 11 patients who received R1 or R2 resections (Table II), lymph node metastasis and liver metastasis significantly predicted worse prognosis, and GEM predicted better prognosis (Table III). However, out of these 3 significant predictors in univariate analysis, only GEM remained significant in multivariate analysis (p=0.020; Table III). Accordingly, the GEM group's MST (66.4 months) was significantly better than the control group's MST (5.4 month) (p=0.002) (Figure 2).
Discussion
We found that GEM was an independent significant prognostic factor for patients with gallbladder cancer with R1 or R2 curability (which itself predicts better prognosis).
The effects of adjuvant chemotherapy on BTC patients are not widely investigated (1); the aforementioned 2002 study from Takada et al. (9) is the only phase III randomized control trial to evaluate adjuvant chemotherapy for BTC patients. This study included not only BTC patients (118 with bile duct cancer, 112 with gallbladder cancer and 48 with ampullary cancer), but also 158 patients with pancreatic cancer. Survival of patients who were treated with MF therapy was compared against survival of patients treated with surgery-alone. The MF therapy improved prognosis of patients with gallbladder cancer (p=0.037), but not that of patients with pancreatic, bile duct, or ampullary cancers. Interestingly, the 5-year survival rates of patients who underwent non-curative resections for gallbladder carcinomas was better in the MF group (8.9%) than in the control group (0%) (p=0.023); whereas among patients who underwent curative resections for gallbladder cancer, survival did not significantly differ between the two groups. As with the Takada study, GEM improved survival after R1 or R2 resection. We did not analyze patients who underwent R0 procedures because we had only 2 patients who received adjuvant chemotherapy after R0 resection.
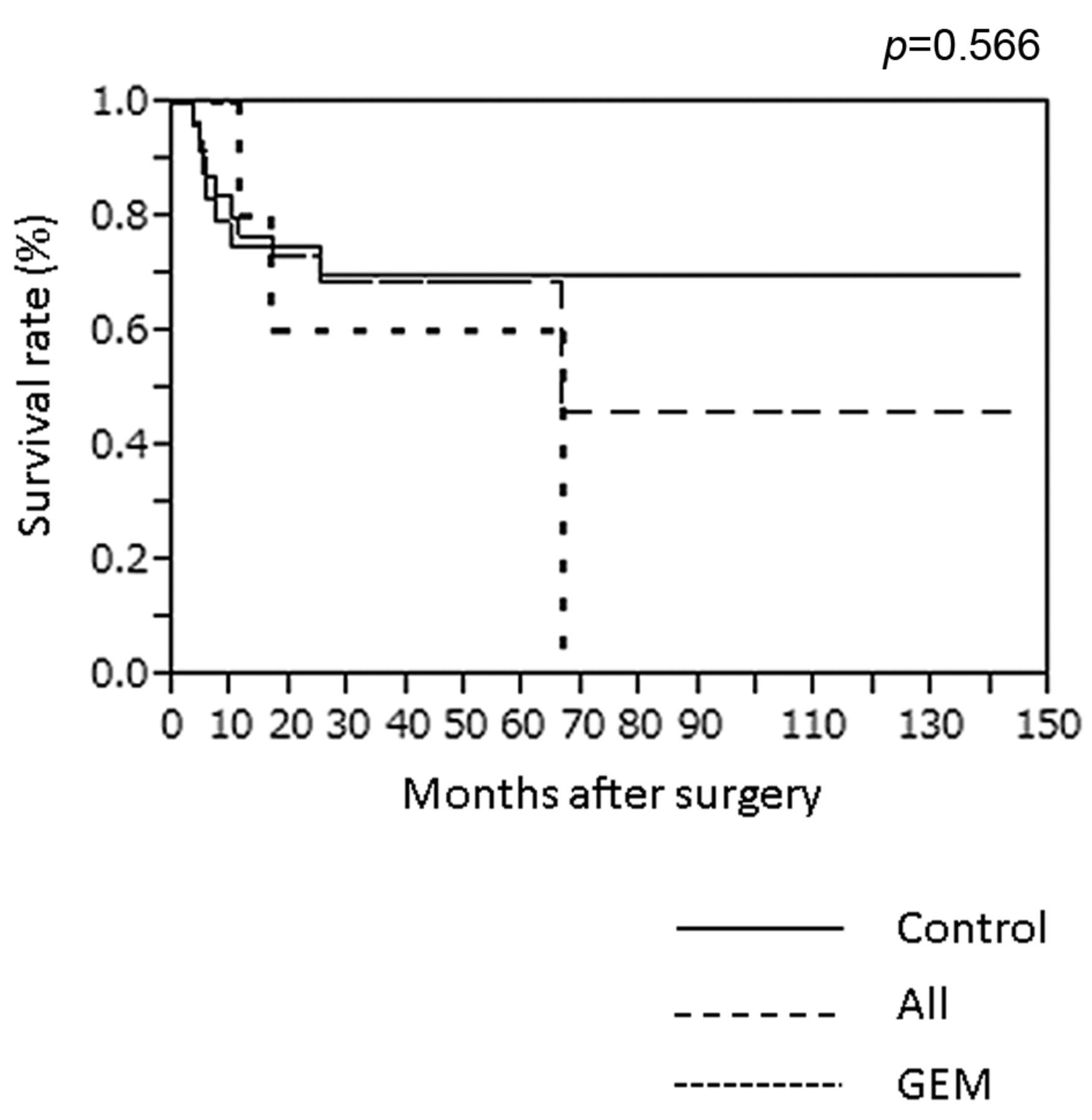
Overall survival rate of patients with gallbladder cancer after radical surgery. Overall survival rates of all patients, those treated with gemcitabine-based adjuvant chemotherapy (GEM), and the control group were compared. p=0.566 for the GEM group vs the control group. p<0.05 was considered statistically significant.
Univariate and multivariate analysis of prognostic factors.
Univariate and multivariate analysis of prognostic factors for R1 and R2 patients.
Our results were also consistent with those of Murakami et al., who retrospectively analyzed hilar bile duct cancer (10) in 42 patients, and found GEM to be a significant, single independent predictor of better prognosis (p=0.035) with 5-year survival rates of 57% and 23% for the GEM and control groups, respectively (p=0.026) (10). Another retrospective analysis from the Murakami group compared patients who received an adjuvant combination of gemcitabine and S-1 (GS) for UICC stage II BTC with patients without adjuvant chemotherapy (control group), and found GS-based adjuvant chemotherapy (p<0.001) and surgical margin status (p=0.003) were independent prognostic factors, with 5-year survival rates of 57% and 24% for GS and control groups, respectively (p<0.001) (11). However, prognosis of the GEM and control groups did not differ in our current study, possibly because the GEM group had more advanced gallbladder cancer than the control group in our study.

{kind=link}
{kind=link}
Overall survival rate of patients with gallbladder cancer after R1 or R2 resections. Overall survival rates of patients treated with gemcitabine-based adjuvant chemotherapy (GEM) and the control group after R1 or R2 resection were compared. p<0.05 was considered statistically significant.
Recently, two groups reported on the effects of gemcitabine–cisplatin combination chemotherapy on un-resectable BTC (2, 5-7). The National Cancer Research Network of UK organized the advanced BTC (ABC)-01 (phase II) and ABC-02 (phase III) studies (5, 6), which were both composed of two arms: one with gemcitabine–cisplatin combination chemotherapy, and one with gemcitabine monotherapy. Patients treated with combination therapy had significantly longer mean survival time (11.7 months) than those treated with gemcitabine-alone (8.3 months) (p<0.001) (6). The ABC study was confirmed by the BT22 trial in Japan (7), which showed median survival time for the combination arm (11.2 months) to be significantly longer than the monotherapy arm (7.7 months) (p=0.139) (7). In the present study, survival of R1 and R2 patients was improved although we mainly used gemcitabine monotherapy as adjuvant chemotherapy. The BT22 and ABC studies suggest that we might further improve survival of patients with patients with gallbladder cancer by using a combination of cisplatin and gemcitabine as adjuvant therapy.
Effects of adjuvant radiotherapy are also controversial. Although 3 retrospective studies have reported that adjuvant radiotherapy improved prognosis of patients with microscopically-positive margins (12-14), Pitt et al. organized a prospective study showing that adjuvant radiotherapy did not improve survival of patients with hilar bile duct cancer (15).
The effects of adjuvant chemo-radiotherapy on BTC are also debated. Hughes et al. and Lim et al. showed significantly improved OS from adjuvant chemo-radiotherapy, whereas Nakeeb et al., Krishnan et al. and Zhou et al. did not find a difference (16-20), and Gold et al. and Kim et al. found a limited effect (21, 22). Clinical research on BTC is complicated by the relatively few patients and the variety of origins, bile duct, gall bladder and ampulla vater. A prospective multi-Institutional joint investigation could overcome these difficulties.
This report is the first to focus exclusively on GEM adjuvant therapy in gallbladder cancer. Wider use of gemcitabine-based adjuvant chemotherapy could improve survival of patients with advanced gallbladder cancer, who currently have poor prognoses. A well-designed randomized prospective multi-Institutional joint investigation is warranted to improve the prognosis of these patients.
Footnotes
-
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received February 24, 2014.
- Revision received April 22, 2014.
- Accepted April 23, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved