

Abstract
Aims: To evaluate the role and expression of vascular endothelial growth inhibitor isoform 174 (VEGI 174) in the microvessels and its correlation with microvessel density (MVD) and prognosis of clear cell renal cell carcinoma (CCRCC). Materials and Methods: Immunohistochemical analysis was performed in 98 cases of renal cell carcinoma and paired normal kidney tissues for VEGI 174 and CD34. The clinical, pathological and follow-up (median follow-up: 54.5 months) information were recorded and analyzed against the VEGI174 and MVD expression. Results: There was an inverse correlation between VEGI 174 and MVD (r=−0.420, p<0.05) in normal human renal tissues and CCRCC specimens. Compared to normal kidney tissues, the expression of VEGI 174 was significantly lower in CCRCC (0.420±0.151 vs 0.107±0.063, p<0.01, respectively). On the contrary, MVD was higher in CCRCC specimens than in normal renal tissues (72.020±31.709 vs. 53.480±11.071, p<0.01, respectively). The expression of VEGI 174 in G1+G2 tumors was significantly higher than in G3 tumors (0.132±0.055 vs. 0.044±0.025, p<0.05, respectively). There was also a statistical significance in the expression of VEGI 174 in patients of different ages (<60y, 0.102±0.054 vs. ≥60 years, 0.117±0.083, p<0.01, respectively). However, between the staining of VEGI 174 and other pathological parameters (gender, tumour size and stage), there were no significant statistical differences (p>0.05). In addition, MVDs did not differ statistically by pathological grade, stage, gender, age or tumor size (p>0.05). Four patients died of CCRCC-related conditions during follow-up. However, no relationship between the expression of VEGI 174/MVD and overall survival was found in the study (p>0.05). Conclusion: VEGI 174 has a significant role in angiogenesis in CCRCC, and appears to be a negative regulator of aggressiveness during the development and progression of CCRCC.
- Vascular endothelial growth inhibitor 174 (VEGI 174)
- microvessel density (MVD)
- prognosis
- clear cell renal cell carcinoma
Recent years have witnessed the increase in the incidence of renal cell carcinoma (RCC), which now accounts for 2%-3% of all adult malignant neoplasms and is the most lethal of the common types of urological cancer (1). In urological cancers, 30%-40% of patients with RCC would die from RCC-related causes, while the corresponding rates are 20% for patients with both prostate and bladder carcinomas (2, 3). Since the 1980s, based on all ethnic groups and both sexes, there has been a steady increase in the mortality rate from RCC, and the incidence of advanced tumours has also grown (4). Of all patients newly-diagnosed with RCC, one-third present with synchronous metastatic disease, while an additional 20%-40% with localized tumour at diagnosis will eventually develop metastases (5-7). Furthermore, 70%-80% of all RCCs are clear cell RCC (CCRCC) (8, 9).
CCRCC is unresponsive to traditional chemotherapies, highly resistant to radiation therapies, and lacks the hallmark genetic features of solid tumors (10). Targeted agents have dramatically changed the treatment of metastatic RCC. Targeted therapy, including anti-angiogenesis and anti-proliferation treatments, has assumed an important role in the treatment of metastatic RCC. Angiogenesis, the process of new blood vessel formation, is one of the most important factors in both progression and metastasis of cancer (11). Although the complicated mechanism of angiogenesis is not yet totally understood, it appears that the initiation or termination of the process is a result of a balance between positive and negative regulators of angiogenesis (12). The imbalance of pro-angiogenic and anti-angiogenic factors leads to abnormal production of vessel, including structural and functional defects (13). Tumor neovasculature, mostly defective is critical to the continued and controlled growth and spread of solid tumors including RCC. Anti-angiogenic therapy has shown promise in the treatment of patients with metastatic RCC. Most drugs block the vascular endothelial growth factor (VEGF) pathway, as VEGF is one of the most dominant pro-angiogenic growth factors in the tumour microenvironment (14). For example, sunitinib, a Food and Drug Administration (FDA)-approved agents, can directly target the VEGF pathway (15, 16). Nevertheless, these inhibitors are also associated with significant toxicities related to off-target inhibition that are detrimental to the patient's quality of life, even thought provide superior efficacy and tolerability (17, 18). Moreover, single angiogenic inhibitors only have partial benefits for patients in view of the complex etiology of RCC (19). Combination therapy of chemotherapy and anti-angiogenic therapy has been shown to be more toxic and yet not necessarily more effective than sequential immunotherapy (20). Therefore, it is very important to find new and more effective targets.
Vascular endothelial growth inhibitor (VEGI) is an endogenous angiogenesis inhibitor which negatively-regulates the neovasculature and is a potentially therapeutic agent for the treatment of disease conditions involving angiogenesis (21, 22). To date, mRNA of VEGI was found in most normal tissues, e.g. prostate, bladder, tumor tissues (breast cancer and colon cancer) and cell lines, e.g. human endothelial cell cancer cell lines (23). A few studies have shown the anti-tumour activity of VEGI in human cancer, including lung, colon and breast cancer (22, 24, 25). Previous experiments implied that the anti-tumour effect of VEGI may come from suppression of neovasculature associated with tumors (24, 26). Different from VEGF, VEGI exerts its function via distinct signaling pathways that would result in the termination of angiogenesis (25). Furthermore, there was an inverse correlation between the expression of VEGI and pathologicalal grade in renal cell carcinoma as shown in our previous study (27). In the current study, we evaluated the possible relationship of VEGI and neovasculature in RCC. VEGI has three isoforms, VEGI 174, 192 and 251. VEGI 174 expression markedly decreased in CCRCC and was linked to pathological grade and stage (28). In addition, inhibition of tumor angiogenesis was evident from much decreased microvessel density (MVD) (22). Therefore, we hypothesized that VEGI 174 in CCRCC tissues may influence the formation of MVD, play a role in tumor pathogenesis and display correlation with patient prognosis, for this reason we conducted the present study.
Materials and Methods
Materials. Specimen of sporadic CCRCC were collected from the Department of Urology, Beijing Chaoyang Hospital, Capital Medical University (Beijing, China) between 2005-2011. A total of 98 pairs of renal tumor tissues and matched normal kidney tissues was collected. None of the enrolled patients had received preoperative immunotherapy or renal arterial embolization therapy. The average age of the 98 CCRCC cases was 53±12 years. Seventy-four (75.5%) patients were male and 24 (24.5%) female. In addition 70 patients were below 60 years of age (71.4%); 66 (67.3%) tumors were less than 7 cm in size. Regarding the tumor grade, 32 (32.7%) were G1, 38 (38.7%) G2 and 28 (28.6%) G3; and 84 (85.7%) cases were pT1+pT2, and 14 (14.3%) pT3+pT4 pathological stage. Every specimen was immediately stored at −80°C. All protocols were reviewed and approved by the local Ethics Committee of the Beijing Chaoyang Hospital of Capital Medical University and all patients gave their written informed consent. The clinical and pathological characteristics of the patients are given in Table I.
Polyclonal mouse anti-human-VEGI antibody (LS-C40892) and monoclonal mouse anti-human-CD34 antibody (LS-B5262) were purchased from Lifespan Bioscience, Inc. (Seattle, WA, USA). PV-9000 polymerization peroxidase anti-mouse/rabbit IgG two-step immunohistochemical detection kit from ZSGB-BIO (Beijing, China).
Immunohistochemical staining of CCRCC specimens. The nature of the samples was independently-verified by two pathologists and histological typing and grading were carried out according to Fuhrman's nuclear grading system. The sections showing adequate amount of viable tumor without haemorrhage, necrosis or inflammation were selected. Frozen specimens of CCRCC tissue (n=98) were cut at a thickness of 6 μm using a cryostat (Leica CM 1900; Leica Microsystems UK Ltd., Buckinghamshire, UK). After fixation, the samples were probed an antibody against VEGI (1:1500) or CD34 (1:200) following blocking with horse serum, and labelled with a biotinylated secondary antibody, and subsequently visualized using Vectastain Universal Elite ABC kit (Vector Laboratories, Peterborough, UK).
The relationships between VEGI, MVD and pathological parameters of the patients.
Evaluation of immunohistochemical staining. The expression of VEGI 174: Each section was examined using ×100 optical fields (10 fields per location) and the mean optical density was analyzed by analysis software Image-Pro Plus (Rockville, MD, USA) to quantify the expression of VEGI 174. MVD: MVD was evaluated according to previously-described criteria (29). The tumor sections stained by CD34 antibody for labelling of endothelial cells were screened under light microscopy. Eight most highly staining areas (hot spot) at ×400 magnification were selected. MVD was the mean number of vessels in each hot spot in an area of 0.23 mm2.
Clinical follow-up. All of the patients were followed up every 3-6 months for two years postoperatively. After that, every patient was followed-up on a yearly basis. The last date of follow up was November 1st, 2012, and median follow up for the population studied was 54.5 months (range, 20-89 months).
Statistical procedures. The differences of expression of VEGI 174 and MVD in normal kidney and RCC tissues was analyzed by an independent-sample t-test. Spearman correlation was used described the association between VEGI 174 and MVD. Comparisons of VEGI 174/MVD by different gender, age, tumour size, nuclear grade and tumour stage were carried out using independent-sample t-test. Kaplan-Meier method was used to analyze overall survival curves. The cut-off value for definition of the immunohistochemical marker subgroups was the median value. Statistical significance was defined as p<0.05. IBM SPSS Statistics 18.0 was used for the analyses.
Results
Correlation between VEGI 174 and MVD. Expression of VEGI 174 protein (brown staining) was primarily observed in the cell cytoplasm in CCRCC (Figure 1B-D). Meanwhile, the yellow staining of vessels (CD31) is shown in Figure 1F. Compared with normal kidney tissues, the expression of VEGI 174 was significantly lower in CCRCC (0.420±0.151 vs. 0.107±0.063, p<0.01, respectively) (Table II), while MVD was higher (53.480±11.071 vs. 72.020±31.709, p<0.01, respectively) (Table II). The spearman correlation suggested the inverse correlation between VEGI 174 and MVD (r=−0.420, p<0.05) (Figure 2).
VEGI and MVD in normal kidney tissue and CCRCC.
Relationships between VEGI 174, MVD and pathological parameters. As shown in Table I, the expression of VEGI 174 in G1+G2 tumours was significantly higher than in G3 (0.132±0.055 vs. 0.044±0.025, p<0.05, respectively). There was also statistical significance in the expression of VEGI 174 in different ages (<60rs years, 0.102±0.054 vs. ≥60 years, 0.117±0.083, p<0.01, respectively). However, between the staining of VEGI 174 and other pathological parameters, there were no statistical significant differences.
MVD according to different pathological parameters are also showed in Table I. The differences in MVD gender, age, tumor size, grade and stage had no statistical significance.
Correlation between VEGI 174/MVD and overall survival. The correlation between the expression of VEGI 174/MVD and overall survival is showed in Figure 3. The tumour-free survival rate was 96% (94/98) during 54.5 (range, 20-89) months. Only four patients died due to CCRCC during follow-up. We did not find a significant correlation between VEGI 174/MVD and overall survival (p>0.05).
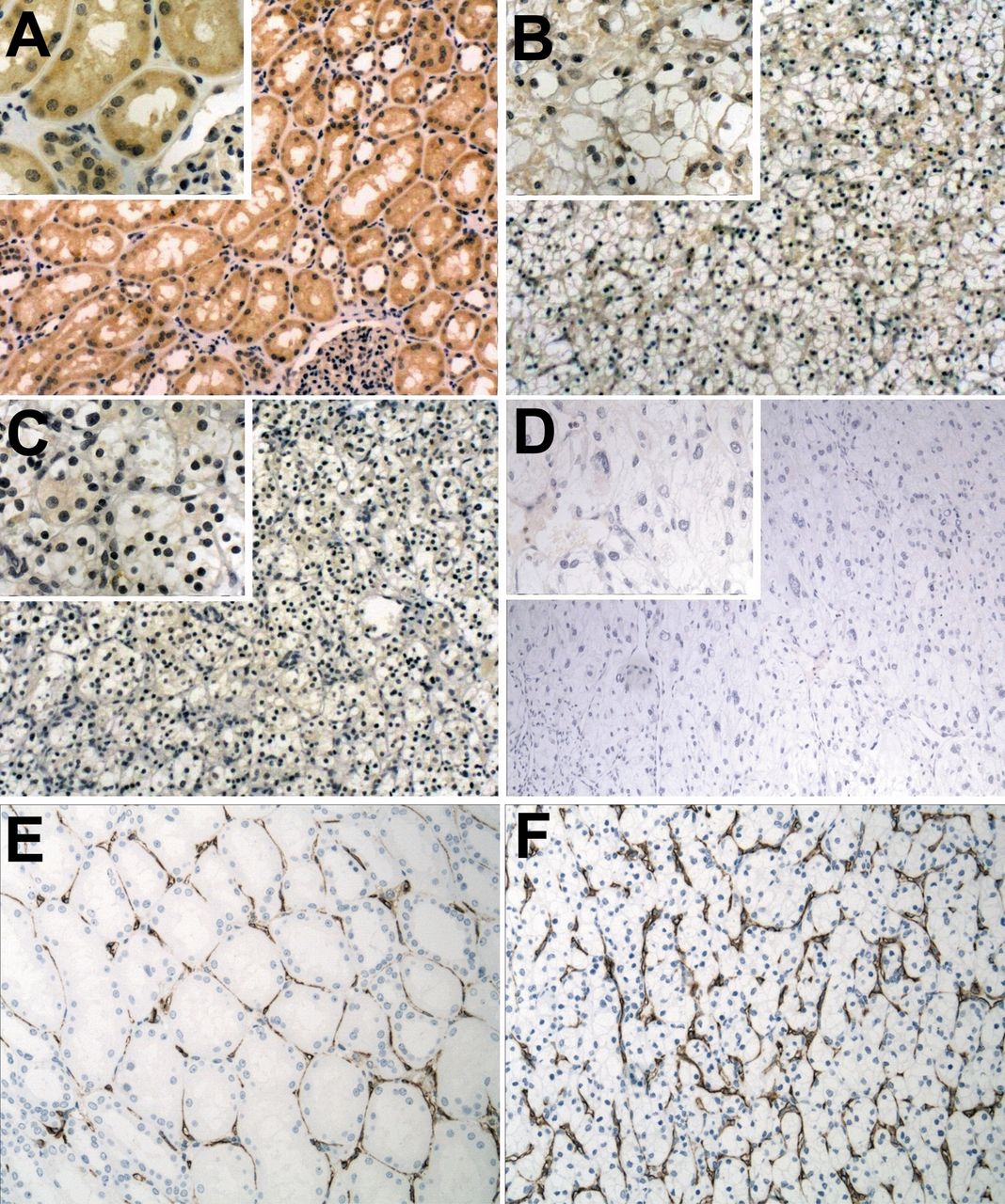
The expression of VEGI and MVD in normal and CCRCC tissues. A-D: Immunohistochemical staining of normal kidney tissue and CCRCC tissue. A: Normal kidney tissue. The VEGI protein was found to be well-stained in the cytoplasmic area (brown staining). B, C and D: G1, G2 and G3 CCRCC tissues, respectively. VEGI was only weakly-stained in the tumor cell. E and F: The expression in vessels (yellow staining) was higher in F than E.
Discussion
The growth and the growth rate of solid tumours depend on pathological angiogenesis (30), a hallmark of cancer. Different from physiological angiogenesis, the pathological condition, once initiated, is prolonged and on-going with no termination despite the formation of new vessels (22). Tumor microvessels develop by sprouting (angiogenesis) or intussusception from pre-existing vessels (19). Anti-angiogenic therapies have, thus, been in the spotlight for the past two decades, with some already been used in clinical practice.

Correlation between VEGI and MVD. Our results show an inverse correlation between VEGI 174 and MVD, r=−0.420, p<0.05.
As a member of the tumor necrosis factor superfamily, VEGI (also known as tumor necrosis factor superfamily member 15 (TNFSF15) and TNF ligand related molecule 1 (TL1) was first reported in 1997 (33). In an experiment of recombinant VEGI-174 treatment of ABAE cells, ABAE cells developed a network of capillary-like tubules after stimulation by VEGF or fibroblast growth factor-2 (FGF2), while VEGI-174 totally inhibited capillary formation, but did not lead to cell death (32). Moreover, it has also been shown that VEGI is a key component of a molecular mechanism that inversely modulates endothelial progenitor cell (EPC)-supported vasculogenesis through regulation of the relative levels of membrane-bound Flt1 and soluble Flt1 in EPC (33).
The secreted soluble form of VEGI 174 has been demonstrated to be a potent anti-angiogenic factor through inhibiting proliferation of endothelial cells (34). The growth of colon carcinoma cells (murine colon cancer cells, MC-38) can be suppressed by VEGI 174 both in vitro and in vivo (25, 35). Meanwhile, Paulina et al. demonstrated that VEGI 174 inhibits tumour vasculogenesis and tumour growth in Lewis lung carcinoma (24). Patients with breast tumours expressing decreased levels of VEGI 174 had a higher local recurrence rate, shorter survival time and poorer prognosis than patients expressing high levels of VEGI 174 (36). Studies have also shown that expression of VEGI is lower in bladder and prostate carcinomas and can suppress motility and adhesion of tumor cells (37, 38). Importantly, in in vitro experiments, VEGI had no inhibitory activity on the growth of cancer cells (25, 39). Together, these studies imply that the anti-tumour effect of VEGI originates from the influence on the vasculature associated with tumour, but not necessarily any direct activity on cancer cells.
Despite RCC being a highly vascularised tumor and there being an inverse correlation between VEGI and pathologicalal grade, the relationship of VEGI and neovasculature in RCC remains unknown. We investigated the role of VEGI in microvessels by immunohistochemical staining in RCC. Our findings indicate that the expression of VEGI protein correlates inversely with the MVD. VEGI 174 protein levels were lower in RCC tissues than that in normal renal tissues, while MVD was higher (Table II). All the results are consistent with previous reports forn breast and colon carcinomas, as well as partially validates our hypothesis that the antitumour effect of VEGI is based on its influence on vasculature in RCC.
VEGI 174 marginally differed by gender, age, tumour size, pathological grade and stage showed different expressions, however, statistically significant differences were only found for grade and age. The expressions of VEGI 174 in different nuclear grades were cross-checked in some other studies (27, 28). Our results further verified that the higher the pathological grade, the lower the expression of VEGI 174. Lee et al. (elaborated that RCC in young patients was associated with poorer prognosis (40). Combined with our findings of weaker expression of VEGI 174 in younger patients (<60 years), it could indirectly indicate that VEGI 174 is a negative regulator of tumour aggressiveness during the development and progression of CCRCC. In addition, there were no statistical differences in expression of VEGI 174 by pathological stage or tumor size. Further analysis in patients with more malignant pathological features, also supports the inverse correlation of VEGI 174 expression and aggressiveness of RCC.
A correlation between MVD and tumor aggressiveness has been established for several malignancies. However, the results are controversial for CCRCC. While some studies have shown inverse correlation between MVD and nuclear grade or pathological stage (41-43), others revealed no correlation (44-47). In our study, no association was noted between angiogenesis and any of these pathological parameters. These findings are contradictory to the hypothesis that an increasing MVD indicates worsening of cancer progression. Certain hypotheses may explain this paradox. Firstly, in the normal kidney, the tubules are closely associated with blood vessels. RCC imitates tubule differentiation. Therefore, the high MVD of carcinoma tissue may be considered to reflect the normal structure, function and tissue organization of the renal tubule system (41). Secondly, the decreasing MVD in high-grade RCC reflects the inability of tumour neovascularization to keep pace with the proliferation of tumor cells in grade 3 tumours (48). Insufficiency in these mechanisms leads to a reduced metabolic supply, resulting in extensive necrosis, a morphological finding that is very characteristic of large RCC (49). Low MVD has been also reported to be associated with tumor fibrosis and the development of large-diameter vascular channels (50). It is therefore plausible that poorly-vascularized tumors may become hypoxic and necrotic.

{kind=link}
{kind=link}
{kind=link}
Survival time in 98 patients with CCRCC. Our results showed that there was no statistical difference between patients with low and high expression of VEGI or MVD, p>0.05.
The present study failed to established a link between VEGI/MVD and the survival of patients, an observation that reflects the controversies in this area. Yildiz et al. and others found MVD in RCC to be inversely associated with patient survival (43, 49, 51). On the other hand, others repported that no statistically significant differences in survival were found for MVD (46, 47). Clearly, there is more to be learned here ideally with a larger cohort and longer follow-up periods.
In conclusion, VEGI 174 has a significant role in angiogenesis in CCRCC, and appears to be a negative regulator of aggressiveness during the development and progression of CCRCC. Despite the limited evidence, it is possible that, as a valuable marker in prognostic nomograms for CCRCC, VEGI 174 might become an efficient target in treatment of patients in the future.
Acknowledgements
This work was supported by the National Natural Science Foundation of China, grant number 81072088, and Cancer Research Wales (WGJ).
Footnotes
-
* These Authors contributed equally in this study.
-
Conflicts of Interest
No potential conflicts of interest are disclosed.
- Received December 5, 2013.
- Revision received December 21, 2013.
- Accepted December 23, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved