

Abstract
Aim: Associations between polymorphisms of the epidermal growth factor receptor (EGFR) and overall survival in patients with advanced carcinoma of the head and neck (HNSCC) receiving cetuximab based palliative treatment, were evaluated. Materials and Methods: HNSCC patients (n=48) received cetuximab +/− chemotherapy. Samples for DNA extraction and clinical data were collected prospectively. Genotyping of four EGF(R) polymorphisms was performed using PCR-based restriction fragment length polymorphism (RFLP). Results: The median overall survival was 10.6 months. The EGFR-R497K polymorphism was significantly associated with overall survival. The presence of at least one K-allele was associated with shorter overall survival. The median survival in these patients was 6.7 months compared to 13.3 months in the patients homozygous for the wild type allele EGFR-497R (p=0.009). Addition of chemotherapy to cetuximab, age and EGFR-R497K polymorphism were independent predictors of overall survival. Multivariate analysis revealed a hazard ratio (HR) for patients with at least one EGFR-497K allele of 3.03 when compared with EGFR-497R homozygous patients (p=0.045). Conclusion: The EGFR-R497K polymorphism is a potential predictor for overall survival in HNSCC patients treated with cetuximab based therapy in the palliative setting.
- EGFR polymorphism
- SNPs
- cetuximab
- head and neck cancer
- PCR-RFLP
The epidermal growth factor receptor (EGFR) is a member of the ErbB family of the tyrosine kinase receptors, which includes ErbB2, ErbB3 and ErbB4. These receptors play a fundamental role in the control of numerous cellular processes such as growth, proliferation, and survival. Activation of EGFR in response to ligand binding results in autophosphorylation of several tyrosine residues, which ultimately results in activation of intracellular signal cascades leading to cell proliferation and survival (1, 2).
Treatment options for metastatic or recurrent squamous cell cancer of the head and neck (HNSCC) were very limited until the introduction of the EGFR antibody cetuximab (3, 4). The addition of cetuximab to radiotherapy significantly improves recurrence rates and overall survival over radiotherapy alone in patients with locally advanced HNSCC (5). Vermorken et al. showed for the first time that patients with recurrent or metastatic HNSCC derive substantial benefit from the addition of cetuximab to the standard chemotherapy of platin/5-fluorouracil, showing 2.7 months longer median survival (7.4 vs. 10.1 months) (6). Despite the observed improvement, overall survival in general remains short and some patients derive no benefit from the addition of cetuximab.
Several reports have demonstrated that the expression and activity of the EGFR is highly modified by several polymorphic regions within the EGFR gene (7-11). These polymorphisms include the -216G/T, -191C/A and R497K polymorphism among others. While the -216G/T and the -191C/A SNPs are located within the EGFR gene promoter and have been demonstrated to alter EGFR gene expression (8), the nonsynonymous common EGFR SNP in codon 497 (R497K) determines EGFR function. Moriari et al. showed that the K-allele of this polymorphism is associated with a decreased function of the receptor (11). The exchange from arginine to lysine leads to a EGFR variant that demonstrates less affinity to EGF and other ligands such as transforming growth factor α and has less mitogenic activity.
The impact of functional EGFR polymorphisms on treatment efficacy in this patient population has not yet been analyzed in depth. The goal of the current study was to identify EGFR polymorphisms in HNSCC patients with recurrent or metastatic disease and to reveal the EGFR genotypes that are associated with the best clinical outcome in cetuximab-containing systemic therapy.
Materials and Methods
Only patients with recurrent or metastatic HNSCC were included in this study. The patients were treated either with cetuximab + chemotherapy (cisplatin or carboplatin plus 5-FU) (82% of cases, 40/48) or cetuximab alone (8 patients) according to standard protocols. The patients characteristics are summarized in Table I. Genomic DNA was extracted from all the 48 HNSCC patient samples. Two single nucleotide polymorphisms (SNP) in the EGFR promotor region (-216 G/T [rs712829] and -191 C/A [rs712830]), one SNP in codon 497 of exon 13 (R497K G→A [rs2227983]) and one SNP located in the 5’ untranslated region at position 61 of the EGF gene (61 A/G [rs 4444903]), were analyzed.
All the polymorphisms were determined by PCR-RFLP techniques. The specific primer pairs, PCR products, restriction enzymes (New England BioLabs) and restriction fragments are summarized in Table II. Restriction fragments were separated on a 3% ethidium bromide–stained agarose gel.
Cox regression analyses included genotypes, age, response and treatment regimen (cetuximab monotherapy vs. cetuximab + chemotherapy). Pharmacogenetic analyses were performed retrospectively. All the patients signed an informed consent for genetic testing and the study was approved by the local ethics committee.
Results
Thirty nine out of the 48 patients were evaluable for complete association analyses (31 patients with combination treatment and 8 patients with cetuximab only).
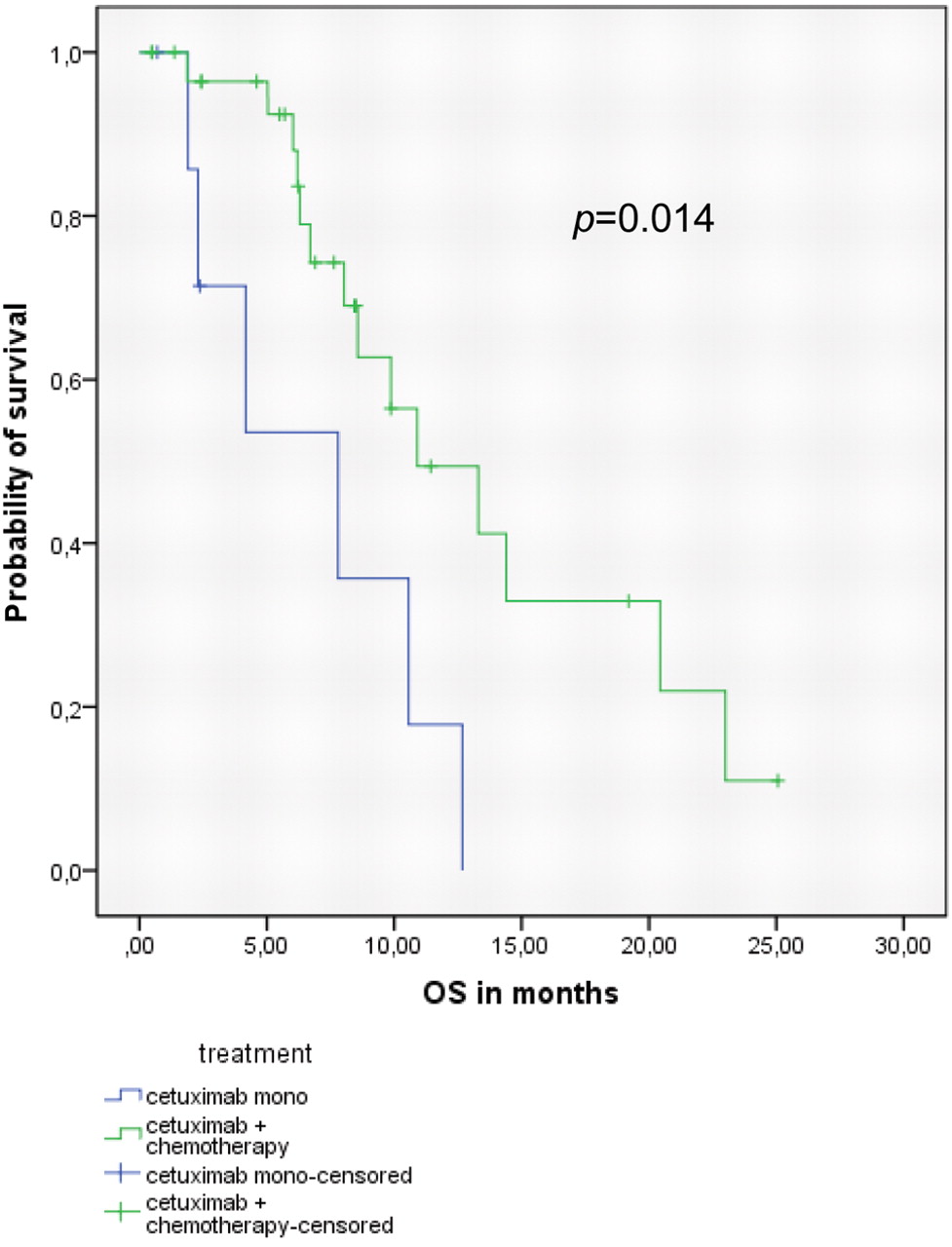
The patients who received cetuximab combined with chemotherapy experienced a statistically significant longer survival with 10.9 months (95% CI 5.6-16.2) than those patients that received cetuximab monotherapy (7.8 months, 95%CI 1.8-13.8) (Figure 1) (p=0.014, log-rank test). The rate of complete and partial remissions for the whole study population was 26% (n=10/39).
The EGFR-R497K polymorphism was significantly associated with overall survival. The presence of at least one variant allele coding for K (lysine) at position 497 was associated with significantly shorter overall survival. The median survival in these patients was 6.7 months compared to 13.3 months in patients homozygous for the wild type allele EGFR-497R (p=0.009; log-rank test) (Table III and Figure 2). No significant association between between EGFR-R497K and response to treatment was observed. The EGF A61G, EGFR G-216T and EGFR C-191A polymorphisms were not significantly associated with overall survival or response in univariate analysis.
Multivariate cox regression analysis revealed the addition of chemotherapy to cetuximab, age and the EGFR-R497K polymorphism as independent predictors of overall survival (Table IV). The patients harbouring at least one EGFR-497K allele demonstrated a significantly increased risk of death independent of age, treatment (cetuximab monotherapy or cetuximab-chemotherapy combination) and response. The hazard ratio (HR) for patients with at least one EGFR-497K allele was 3.03 [95%CI (1.03;8.93)] when compared with EGFR 497R homozygous patients (p=0.045, cox-regression analyses).
Patients' characteristics.
Discussion
The patients with at least one EGFR 497K allele derived significantly less benefit from cetuximab-containing treatment as compared to patients with the common EGFR 497RR genotype. This result was supported by a recent finding in HNSCC patients treated with a combination of cetuximab and docetaxel where HNSCC patients with the EGFR 497RR genotype showed a trend towards longer progression-free survival and increased response (12). However a survival benefit could not be established in that study for second line therapy. The current results also supported the hypothesis that decreased EGFR activity, determined by the R497K variant, may reduce the efficacy of EGFR directed inhibitory therapy. The molecular mechanism responsible for this phenomenon is not yet completely understood. Diminished binding of cetuximab to the EGF receptor structure due to a 497RK or 497KK EGFR genotype appears as a possible explanation. Li and co-workers reported that changes of the amino acid sequence of the receptor, if located in sensitive interaction domains may cause problems for ligands and antibodies such as cetuximab regarding their binding capacity (13).
The patients with the common EGFR 497RR genotype demonstrated increased skin toxicity under the cetuximab treatment in a study by Klinghammer et al. (12), but in the present study standardized information for skin rash was not collected, so a possible association with cetuximab and the EGFR R497K polymorphism could not be confirmed.
Primers and restriction enzymes.
Association between EGF(R) polymorphisms and overall survival (OS) (univariate analysis).
Recently, the importance of the EGFR R497K polymorphism for inhibitory strategies in HNSCC was demonstrated in HNSCC cell lines. Krohn et al. reported that HNSCC cells show differential inhibition to EGFR inhibitors, including cetuximab, depending on the EGFR R497K genotype (14). Interestingly, in vitro the HNSCC cell lines with the EGFR 497K variant tend to be more sensitive. An explanation for this contradictory finding was not provided by the authors. Limited data on the EGFR R479K polymorphism and cetuximab treatment in HNSCC patients are available, however the agreement of the currently presented data and these of Klinghammer et al. (12) supports further reasons for analyses to prove this association.
Interestingly polymorphisms that have been shown to be associated with EGFR expression, including the (CA)n repeat polymorphism in intron 1 of the EGFR (10), do not appear to be related to cetuximab efficacy. In fact, as shown in colorectal cancer, the expression of EGFR as the target of cetuximab is not related to its efficacy (15). Alterations of the EGFR pathway that are located further downstream, namely KRAS-mutations and BRAF-mutations, appear to determine the efficacy of the antibody (15). However, in lung cancer EGFR expression might distinguish between responders and non-responders to cetuximab (16). Therefore genetic polymorphisms that alter EGFR expression may become useful markers in lung cancer.
Multivariate analysis of overall survival (OS).
In HNSCC almost 100% of tumors express EGFR (17), so that genetic polymorphisms that alter this expression may have less impact than for example polymorphisms that impact the structural formula of the receptor, such as EGFR R497K. Klinghammer et al. also included the (CA)n repeat polymorphism in intron 1 of EGFR in their analysis, but could not find any association with clinical parameters for this polymorphism (12). In the current group of HNSCC patients also no associations between EGFR expression-modifying EGFR polymorphisms and clinical outcome with cetuximab therapy, were observed.
Due to the low frequencies of KRAS and BRAF mutations in HNSCC it appears unlikely that those genetic alterations become predictors of cetuximab efficacy in HNSCC (18).
Analyses of EGFRVIII, expression of amphiregulin (19) and the polymorphic Fc gamma receptor IIIa appear to be possible additional candidates for predicting response to cetuximab in HNSCC patients (20).

Association between overall survival (OS) and treatment.
The present study was especially limited by the number of patients and the retrospective nature of the analyses. However, the data were in agreement with other clinical reports in HNSCC patients.
In conclusion, the EGFR R497K polymorphism may be a promising predictor for EGFR directed antibody therapy. It's predictive value for efficacy and side-effects in HNSCC patients under EGFR targeting antibodies should be validated in larger prospective clinical trials.

{kind=link}
{kind=link}
Association between overall survival (OS) and EGFR-R497K polymorphism (p=0.009).
- Received November 21, 2011.
- Revision received December 27, 2011.
- Accepted December 29, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved