


Abstract
Background: Serum dermokine (DK) is a novel biomarker for early colorectal cancer. To our knowledge this is the first study of DK expression in intraductal papillary mucinous neoplasm (IPMN) and pancreatic cancer. Materials and Methods: DK expression in human pancreatic cancer cell lines and tissues was assessed. We compared the sensitivities of common diagnostic markers, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), s-pancreas-1 antigen (SPAN-1), pancreatic cancer-associated antigen (DUPAN-2), and Nation Cancer Center-Stomach-439 (NCC-ST-439) in 26 patients with pancreatic neoplasms. Results: DK was expressed in pancreatic cancer cell lines. Immunohistochemical staining revealed that DK was expressed in atypical and cancerous tissues, but not in the normal pancreatic tissues. Serum DK was relatively high in patients with IPMN. The sensitivities of a serum multimarker test including DK was 76.5% (n=13/17) for IPMA/IPMC/invasive carcinoma derived from IPMN, and 100% (n=9/9) for ordinary invasive ductal carcinoma. Conclusion: Serum DK is a potential biomarker in IPMN and invasive ductal carcinoma, when used in combination with conventional biomarkers.
Pancreatic cancer is diagnosed in most patients once it has reached an advanced stage. The survival rate is limited to 5% because 80-85% of patients have unresectable cancer at the time of diagnosis (1, 2). Ohashi et al. reported intraductal papillary mucin-producing neoplasms (IPMNs) with dilatation of the pancreatic duct in 1982, which have a relatively good prognosis compared with ordinary pancreatic cancer (3). Novel biomarkers and cell biological analysis are required for (IPMN) because of the diverse grades of malignancy. IPMN is suggested to be a pre-cancerous lesion in the pancreatic duct, which is similar to colonic adenoma. IPMN grows slowly but it can develop into invasive ductal carcinoma. Consequently, early-stage diagnosis is important to improve the prognosis for pancreatic cancer. The standard diagnostic serum markers of pancreatic cancer are carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), s-pancreas-1 antigen (SPAN-1), pancreatic cancer-associated antigen (DUPAN-2), and Nation Cancer Center-Stomach-439 (NCC-ST-439). However, these markers are not sufficiently useful to diagnose early-pancreatic cancer. We previously reported that the serum Dermokine (DK) test was beneficial to diagnose early-colonic cancer (4). DK was expressed in colorectal cancer at the early-stage of carcinogenesis including severe adenoma. The expression of DK in pancreatic cancer and IPMN tissues is still unclear.
In the present study, we aimed to clarify the expression of DK in pancreatic neoplasms, including IPMN, and the utility of a serum DK test.
Materials and Methods
Cell culture. A total of six pancreatic cancer cell lines were purchased from RIKEN BioResource Center (Tsukuba, Japan). All cells were maintained in Dulbecco's modified Eagle's medium (Sigma–Aldrich Japan, Tokyo, Japan), supplemented with 10% fetal calf serum.
Serum marker tests in pancreatic neoplasms. The serum concentration of each marker is indicated. The cut-off value of each marker is shown at the bottom. The bold numbers indicate mean of positive cases.
Patients and samples. Serum samples and specimens of pancreatic neoplasms were obtained from patients (n=26) under a protocol approved by the Institutional Review Board of Kyoto Prefectural University of Medicine (KPUM) at the KPUM Hospital from 2006 to 2009. The eligibility criteria of patients were: (i) histologically-proven primary pancreatic tumor; (ii) no active double-cancer (synchronous or metachronous double-cancer); and (iii) no prior chemotherapy or radiotherapy for any other malignancy. Serum samples from randomly selected healthy volunteers were also collected from KPUM (n=25). All patients gave written informed consent, and all aspects of these studies were approved by the Ethics Committees of KPUM.
Blood was collected with the Vacutainer blood collection system (Kyokuto Pharmaceutical Industrial Co. Ltd. Tokyo, Japan). All serum samples were centrifuged (3,000 rpm, 5 min), aliquoted and stored at −80°C. Pancreatic tissues were fixed in 10% paraformaldehyde, and whole-tissue was prepared to make continuous sections along the pancreatic duct. At the Department of Pathology of KPUM, paraffin-embedded sections were subjected to immunohistochemical and hematoxylin and eosin (HE) staining to map for tumor distribution in the whole resected specimen. We analyzed samples of intraductal papillary mucin-producing adenoma (IPMA)/ intraductal papillary mucin-producing carcinoma (IPMC)/ordinary invasive ductal carcinoma derived from IPMN (n=12, cases1-10, 16, and 17) and IPMN with ordinary invasive carcinoma (n=5, cases11-15), as shown in Table I. Subtypes were of gastric type (n=12), intestinal type (n=2) and pancreatobiliary type (n=3), but there was no oncocytic type. One case of very mild dilatation of the pancreatic duct was included as IPMN because of the microscopically aggregated atypical and papillary lesion in the head of the pancreas.
Reverse-transcriptase polymerase chain reaction. For the reverse-transcriptase polymerase chain reaction (RT-PCR) analysis of pancreatic cancer cell lines, total RNA was extracted from the pancreatic cancer cell lines using TRIsure (Nippon Genetics Tokyo, Japan). For detection of DK-γ mRNA and Glyceraldehyde-3-phosphate dehydrogenase (GAPDH), first-strand cDNA synthesis and RT-PCR were performed in duplicate with PrimeScript™ II 1st strand cDNA Synthesis kit (Takara Bio, Otsu, Japan), with oligo-dT primers. PCR was performed with AmpliTaq Gold®PCR Master Mix (Applied Biosystems, Foster City, CA, USA) and PCR Thermal Cycler Dice (Takara Bio), according to the manufacturer's protocol. Primers for the experiment were as follows: DK-γ forward 5’-ATGCCATAAACAAGGACCAGAGAA-3’, reverse 5’-ACACCACC CTCTCATCACTAATCTC-3’; GAPDH forward 5’-ACCTGCC GTCTAGAAAAACCTGC-3’, reverse 5’-CTCCTCACAGTTGC CATGTAGACC-3’.
Antibody preparation. Monoclonal antibody (mAb) generation was performed by Kohjin Bio Co. Ltd. (Sakado, Japan) using the antigen hDK-βΔC-SEAP (His)6, as previously described (4). To detect serum DK-β/γ in patients with colorectal cancer, we established a sandwich Enzyme-Linked Immunosorbent Assay (ELISA) with anti-DK-β/γ mAbs, as previously described (4). We generated anti-DK-β/γ mAb, not anti-DK-γ mAb, because the DK-γ-specific mAb was difficult to generate.
Immunohistochemistry. Paraffin sections (5-μm-thick) of tumor tissues were subjected to immunohistochemical staining for the DK protein with the tyramide amplification method, which uses fluorescyl-tyramide. Antigen retrieval was performed by heating the samples in Dako REAL Target Retrieval Solution (DAKO Japan. Tokyo, Japan), for 40 min at 98°C. Endogenous peroxidases were quenched by incubating the sections for 30 min in 3% H2O2. After a brief wash with phosphate-buffered saline (PBS) (pH 7.2) and 0.3% polyoxyethylene sorbitan monolaurate (Sigma–Aldrich), the sections were incubated for 45 min at room temperature with blocking reagent (Block Ace®; DS Pharma Biomedical Co. Osaka, Japan), to reduce the background signals. Each section was incubated at 4°C overnight with the anti-DK mAb. CSAII (Dako) was used for color development according to the manufacturer's protocols. The sections were counterstained with hematoxylin.
Detection of serum DK by ELISA. We developed a DK-specific ELISA that used an mAb against DK-β/γ. DK-β/γ was captured in 96-well plates for ELISA as follows. First, the captured mAb anti-DK-β/γ (IgG1) was added to each well of a 96-well plate and plates were incubated overnight at 4°C. Wells were then washed with PBS and incubated with PBS, containing 1% Block Ace (DS Pharmaceutical) to block non-specific antibody binding. The serum samples (prepared as described above) were added to each well, and the plates were incubated overnight at 4°C. Horseradish peroxidase-conjugated anti-DK-β/γ mAb (IgG2a) was added and the plates were incubated at room temperature for 1 h. DK was then detected with the tetramethylbenzidine Liquid Substrate System for ELISA (Sigma–Aldrich). The standard used in these assays was recombinant DK-β, expressed in 293/EBNA-1 cells. Standard curves were prepared for each assay. Limit of detection was estimated as 26.3 U/ml as mean of 20-control sample (from 10 separate sources) assay results plus 3-times the standard deviation of the mean. Limit of quantitation was estimated to be 36.7 U/ml as the mean of the same results plus 10-times of the standard deviation. Serum CEA, CA19-9 (Abbott Japan Co., Ltd., Tokyo, Japan) SPAN-1, DUPAN-2, elastase and NCC-ST-439 were quantified at a commercial laboratory (Falco Biosystems Ltd., Kyoto, Japan).
Results
DK mRNA was found to be expressed in human pancreatic cell lines. We performed RT-PCR analysis of DK-γ in six pancreatic cell lines. DK-γ mRNA was expressed in PK-59, NOR-P1, PK-45H, PK-1 and KP4 cells. MIA Paca2 cells did not express DK-γ (Figure 1). The sizes of amplicons were 121 bp for DK-γ and 401 bp for GAPDH.
Immunohistochemistry. Immunohistochemical staining revealed DK expression in IPMNs of gastric type (Figure 2). Multilocular cystic tumor was mainly located in the main pancreatic duct (asterisk) and its branch. The distribution of adenoma is indicated by the blue lines and of carcinoma by the red lines (Figure 2a and b). Although normal pancreatic duct (Figure 2g and h) and mucus cell hyperplasia in the main pancreatic duct (Figure 2c and d) did not express DK, areas of carcinoma exhibited DK expression in the cytoplasm (Figure 2e and f). In carcinoma, DK was diffusely localized in the cytoplasm, as demonstrated by loss of cell polarities and normal structures (Figure 2e). We compared DK expression at a different stage of atypia in the epithelium of the pancreatic duct (Figure 3). In papillary epithelium with mild atypia, DK was not expressed (Figure 3a). DK was expressed in moderate atypia (Figure 3c) and severe atypia (Figure 3e); in severe atypia, DK expression was similar to that in carcinoma (Figure 2e).

Dermokine (DK) expression in pancreatic cancer cell lines. Reverse Transcription Polymerase Chain Reaction (RT-PCR) analysis of DK-γ in six pancreatic cell lines. DK-γ mRNAs were expressed in PK-59, NOR-P1, PK-45H, PK-1 and KP4 cells, but not in MIA Paca2 cells. The sizes of amplicons were 121 bp for DK-γ and 401 bp for GAPDH. DNA fragments were separated by 3% agarose gel electrophoresis.
Detection of serum DK by ELISA. We measured serum DK-β/γ levels in 26 patients with pancreatic neoplasms and compared them with those in 25 randomly selected, healthy volunteers for whom there were full data on their medical condition. To simulate the diagnostic use of this test, we proposed a cut-off value [51 U/ml; derived from the median 36.1 U/ml ± 2 S.D. (14.9 U/ml)]. The median serum DK-β/γ level was slightly higher in IPMA/IPMC/invasive ductal carcinoma derived from IPMN [median=47.2 U/ml, interquartile range (IQR)=27.3-55.9 U/ml] than in healthy volunteers [median=36.1 U/ml, IQR=30.5-37.7 U/ml] (Control in Figure 4a). The specificity of the serum DK-β/γ test was 92.0% in 25 healthy volunteers.
The data of each marker test for pancreatic neoplasms are shown in Table I. The serum concentration of DK was high in eight out of 26 cases (30.8%), six of which were IPMA/IPMC/invasive carcinoma derived from IPMN. CA19-9 was the most sensitive serum marker in both IPMA/IPMC/invasive carcinoma derived from IPMN and ordinary invasive ductal carcinoma (Table II). To examine the correlation of DK with other serum tumor markers, we analyzed the concentration of CA19-9, CEA, SPAN-1 and DUPAN-2 (Figure 4). In most cases, DK was found to be a unique marker for the detection of IPMA/IPMC/invasive carcinoma derived from IPMN (Figure 4b). Serum CEA-, CA19-9-, SPAN-1- and DUPAN-2-positive cases were often also positive for one of the other markers. In our data, six out of 26 patients were double-positive (Figure 4b, bottom left panel). The diagnostic rate was improved to 76.5% (IPMN, n=13/17) and 100.0% (invasive ductal carcinoma, n=9/9), when using DK in combination with the other five tumor markers (Table II). DUPAN-2 is also known as the carbohydrate antigen complex (Lc4), which is complementary to CA19-9.
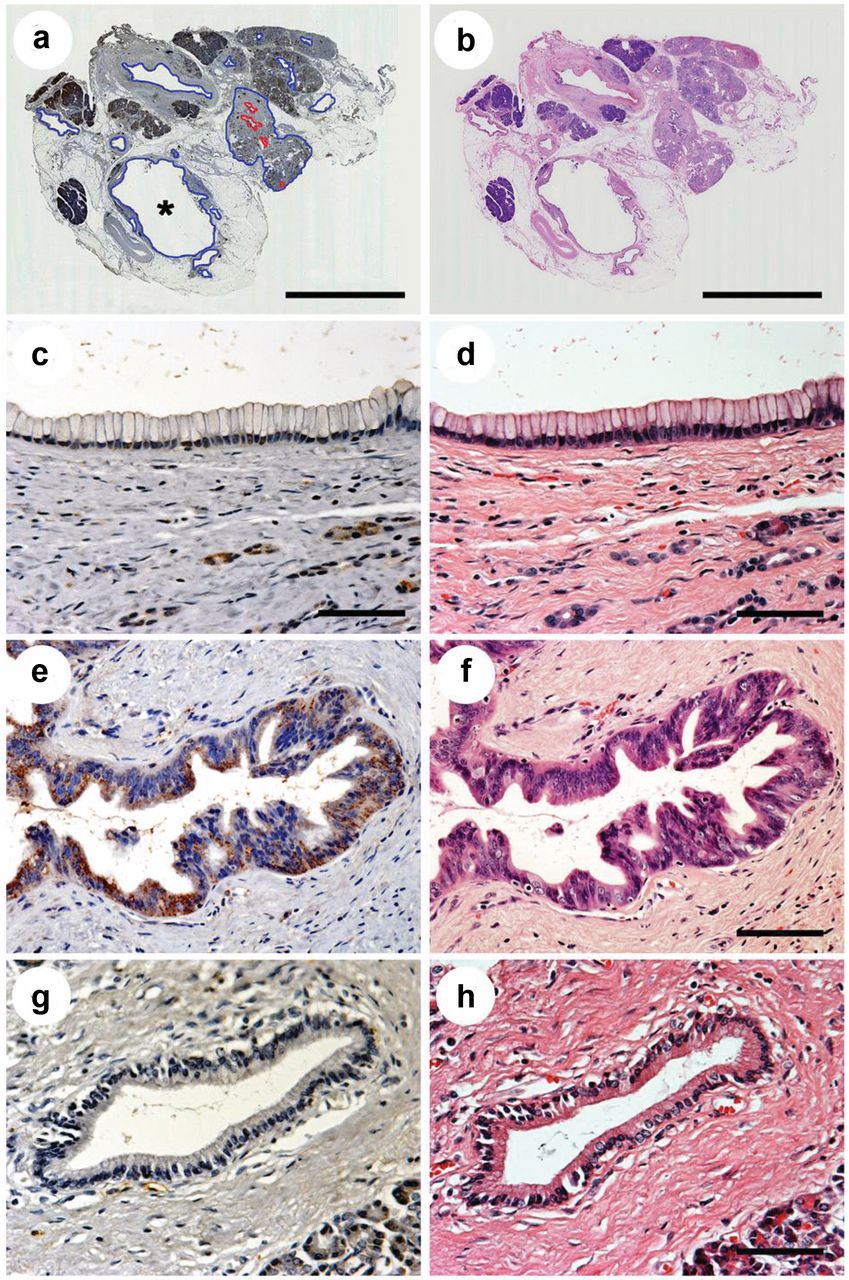
Dermokine (DK) expression in Intraductal papillary mucinous neoplasm IPMN. a, b; Low-power view of IPMN. b; Adenoma (blue lines) and carcinoma in situ (Tis, red lines). c, d; Mucus cell hyperplasia of the pancreatic duct did not express DK. e, f; Carcinomas expressed DK (brown color). DK was mainly located diffusely in the cytoplasm of the carcinoma cells. g, h; Normal epithelium did not express DK. Asterisk, main pancreatic duct; a, DK stain; b, HE stain. a, c, e and g: Immunohistochemical staining of IPMN and the epithelium of pancreatic duct with anti-DK mAb; b, d, f and h: HE stain. Bar, 10 mm (a, b), 50 μm (c-h). The serum concentration of DK was 26 U/ml (within normal limits) in this patient, but expression of DK was confirmed in the tissue.

Dermokine (DK) expression in dysplastic pancreatic duct. a, c and e: Immunohistochemical staining of the atypia of pancreatic duct with anti-DK mAb. b, d and f: HE stain. a, b; Mild atypia did not expressed DK. c, d; Moderately-atypical cells expressed DK in basolateral areas. e, f; In severe atypia, cells lost polarity and cytoplasmic DK of epithelial cells was diffusely localized in the basolateral and apical areas. The localization of cytoplasmic DK was different in the various dysplastic epitheliums. Bar, 50 μm.

Dermokine (DK) Enzyme-linked Immunosorbent Assay (ELISA). a; Serum from 26 patients with pancreatic neoplasms (Intraductal papillary mucin-producing adenoma (IPMA)/Intraductal papillary mucin-producing carcinoma (IPMC)/invasive carcinoma derived from IPMN, n=17; ordinary invasive ductal carcinoma, n=9) and 25 randomly selected volunteers (controls) was subjected to DK ELISA. The cut-off value was 51 U/ml. a; Six patients with IPMA/IPMC/invasive carcinoma derived from IPMN (n=6/17, 35.3%) had a high level of serum DK. b; Comparison of the sensitivity of the diagnostic markers dermokine, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), s-pancreas-1 antigen (SPAN-1), and pancreatic cancer associated antigen (DUPAN-2), according to the histopathological diagnosis. The correlations of the sensitivities for the serum DK test with CA19-9, Span-1 and DUPAN-2 are shown in the panels. DK expression were complementary in IPMA/IPMC/invasive carcinoma derived from IPMN, in CA19-9 (upper left panel), CEA (upper right panel), SPAN-1 (middle left panel) and DUPAN-2 (middle right panel). DUPAN-2- and SPAN-1-positivity coincided with CA19-9-positivity (bottom panels) in most patients. The cuts-off value for each test are indicated by dotted lines.
Discussion
Dermokine was identified as a gene expressed in the spinous and granular layer of stratified squamous epithelium by high-throughput in situ hybridization, and is related to cell differentiation and multilayer structure (5). We have reported on ectopic expression of DK in lesions with high cellularity in colonic adenoma and carcinoma, and its cytoplasmic distribution changes at different stages of carcinogenesis (4). Briefly, the distribution of DK was limited to the apical lesion of adenoma cells, although the location of DK was diffuse in the cytoplasm of carcinoma. Immunohistochemistry revealed that the normal epithelial cells of the pancreatic duct did not express DK (Figure 2). The ectopic expression of DK changed the cytoplasmic distributions, with the loss of cellular polarity (Figure 3). Although the molecular function of DK is still unclear, it was interesting that the cytoplasmic distribution was different in atypical tissues of the pancreatic duct, colonic adenoma and colonic carcinoma, as we have previously described (4). These findings are suggestive of the different manners of carcinogenesis in colonic cancer and IPMN-induced pancreatic cancer. To our knowledge, this is the first study of DK expression in pancreatic neoplasms.
Sensitivities of multimarker tests in detecting pancreatic neoplasms. The serodiagnostic-positive rates for all six markers dermokine (DK), carbohydrate antigen 19-9(CA19-9), carcinoembryonic antigen (CEA), s-pancreas-1 antigen (SPAN-1), pancreatic cancer associated antigen (DUPAN-2), and Nation Cancer Center-Stomach-439 (NCC-ST-439), and their combinations are shown. Serum DK was high in IPMA/IPMC/invasive carcinoma derived from IPMN. CA19-9 was the most sensitive marker for invasive ductal carcinoma and IPMA/IPMC/invasive carcinoma derived from IPMN. Serum tests for all six markers had 100% sensitivity for ordinary invasive ductal carcinoma (n=9/9), and 76.5% of IPMA/IPMC/invasive carcinoma derived from IPMN (n=13/17). This was because the DK test was complementary to the tests for other markers. DK was the best partner for CA19-9 for the diagnosis of pancreatic neoplasm.
There are two hypotheses to explain pancreatic carcinogenesis. The first is pancreatic intra-epithelial neoplasia: the PanIN hypothesis. PanIN lesions are associated with somatic alterations in canonical oncogenes and tumor-suppressor genes. Most notably, early PanIN lesions and almost all pancreatic ductal adenocarcinomas involve mutations in the KRAS oncogene. Thus, it is believed that activation of KRAS mutations is crucial for the initiation of pancreatic ductal carcinogenesis (6). The other hypothesis is that of hyperplasia/adenoma/carcinoma in IPMN. The molecular abnormalities in IPMN are still unclear because some genetic changes are similar but others are clearly different to those of PanIN (7). Recently, Izeradjene et al. have reported that KrasG12D and Smad4/Dpc4 haploinsufficiency co-operated to induce mucinous cystic neoplasms and invasive adenocarcinoma of the pancreas in a mouse model (8). However, IPMN is a disease of the ductal epithelium and represents a spectrum of disease, ranging from benign to malignant lesions in humans. The early detection and characterization of IPMN lesions are important because definitive management is surgical resection for malignant lesions and for benign lesions with malignant potential.
IPMN has been reported to account for approximately 7% of clinically-diagnosed pancreatic neoplasms and up to 50% of incidentally detected pancreatic cysts (9). The incidence of these mucin-producing epithelial tumors of the exocrine pancreas has been increasing (10). This is probably attributed to improvements in technology and diagnostic imaging, as well as to more distinct nomenclature. Although adequate screening tests have not been established to detect malignant IPMN, Nara et al. reported that high levels of serum CA19-9 is a poor prognostic factor in patients with invasive ductal carcinoma derived from IPMN (11).
Computed/tomography, ultrasonography and CA19-9 blood test are widely performed to investigate pancreatic neoplasms, but these procedures are not adequate in terms of cost and specificity. CA19-9 is a terminal structure in various glycoproteins and glycolipids. It is a carbohydrate antigen complex whose expression is dependent on the activity of fucosyltransferase. This means that in 4-10% of the population (Lewis antigen-negative) in Japan, patients are genetically-negative for CA19-9 even if they have a pancreatic neoplasm. In addition, CA19-9 is located in the epithelium of normal pancreatic duct, but its cytoplasmic distribution is limited to apical lesions, similar to CEA in normal colon epithelium. This is one reason for the low CA19-9 concentration in normal structures. Thus, the serum concentration of CA19-9 is high in patients with an inflammatory or cystic disease due to loss of cell polarity, and the presence of abnormal structures. The conventional biomarkers, CEA, SPAN-1 and DUPAN-2 show no correlation with the aggressive nature of IPMN (12).
As shown in Figure 4 and Table I, DK is a unique marker and it improved the diagnostic sensitivity for IPMN and invasive ductal carcinoma. We suggest that a serum DK test might be the best partner for CA19-9 for the diagnosis of pancreatic neoplasms.
In conclusion, serum DK is a potential biomarker in IPMA/IPMC/invasive carcinoma derived from IPMN and ordinary invasive ductal carcinoma of pancreas, when used in combination the with other conventional biomarkers.
Acknowledgements
We wish to thank Toshitaka Sato, Yasuyuki Honda, Yasunori Shimoduru and Masahiko Katayama (EISAI Core Technology Institute, Japan) for their technical assistance with ELISA; Sayaka Katahira-Tayama and Itsumi Ohmori (MTT Program, Tokyo Medical and Dental University) for their technical assistance with quantitative real-time RT-PCR; Akio Yanagisawa (Department of Pathology, Kyoto Prefectural University of Medicine) for their histopathological assistance; and Nagahide Matsubara (Department of Surgery, Hyogo College of Medicine) and Tesshi Yamada (Chemotherapy Division and Cancer Proteomics Project, National Cancer Research Institute, Tokyo, Japan) for being helpful. This work was supported by a Grant-in-Aid for Scientific Research (C) 17591428, the Third-Term Comprehensive Control Research for Cancer conducted by the Ministry of Health, Labor and Welfare of Japan and Charitable Trust Laboratory Medicine Foundation of Japan for Shojiro Kikuchi; a Grant-in-Aid (B)21790267 for Takeshi Matsui; and by the Program for Improvement of Research Environment for Young Researchers from the Special Coordination Funds for Promoting Science and Technology (SCF), commissioned by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) of Japan for Takeshi Matsui.
Footnotes
-
↵* These Authors contributed equally to this work.
-
Conflicts of Interest
The Authors have no potential conflicts of interest to disclose.
- Received April 24, 2012.
- Revision received August 30, 2012.
- Accepted September 3, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.