Article Text

Statistics from Altmetric.com
INTRODUCTION
Recent estimates for cancer incidence and mortality in Europe continue to rank colorectal cancer as the second most common cause for cancer related death. Every year more than 376 000 patients are newly diagnosed with colorectal cancer and approximately 200 000 people die from the disease.1 Even though these numbers show a slight decrease,2,3 partially due to more effective screening programmes, they still represent a major medical and economic challenge. During the past 10 years, intensive clinical studies helped to establish the value of adjuvant therapy for colorectal cancer. The introduction of new chemotherapeutic agents such as irinotecan and oxaliplatin has led to a significant increase in tumour response and median survival. In advanced colorectal cancer, impressive prolongation of overall survival can be achieved through sequential application of combined systemic chemotherapy. In addition, targeted manipulation of molecular tumour mechanisms with new substances such as monoclonal antibodies against the epidermal growth factor receptor or vascular endothelial growth factor shows promising effects. Apart from the encouraging improvement in treatment results, introduction of new drugs and strategies has multiplied the available treatment options, which are much more complex and sometimes confusing in their variety.
This review aims to summarise the current systemic treatment options of colorectal cancer with an additional focus on new classes of targeted compounds recently introduced into clinical management.
TREATMENT STRATEGIES
The only curative strategy in the treatment of colorectal cancer is, and so far remains, complete surgical resection. Despite the fact that approximately 70–80% of patients are eligible for curative surgical resection at the time of diagnosis,4,5 five year overall survival is only 50–60%.6–8 Two out of three patients who undergo curative resection will experience local recurrence or distant metastases. In 85%, relapse is diagnosed within the first 2.5 years after surgery.9 This is mostly related to occult distant micrometastases that will lead to recurrent metastatic disease and are not detectable with the currently available diagnostic tools by the time of the first diagnosis. From diagnosis of metastatic disease, patients with advanced colorectal cancer have a median survival rate of only six months. During this period many patients will suffer from severe physical and psychological tumour associated symptoms that detract from their quality of life.10
Therefore, systemic treatment of colorectal cancer has three major aims:
-
To prevent local recurrence or metastatic disease after complete surgical resection—adjuvant therapy.
-
To prolong survival, control symptoms, and improve quality of life in patients with metastatic disease—palliative therapy.
-
To enable secondary curative resection or increase relapse free survival through preoperative treatment—neoadjuvant therapy.
Figure 1 provides a cumulative overview of the clinical introduction of new systemic therapies and the development of treatment strategies in the field of colorectal cancer.

Time points for clinical introduction of systemic treatments and treatment strategies in colorectal cancer. 5-FU, 5- fluorouracil.
PATIENT APPROACH
Staging
Selecting the optimal therapeutic strategy for a patient newly diagnosed with colorectal cancer depends mainly on accurate clinical and pathological staging. Dukes’ staging system, originally described by Dukes in 192911 and modified by Astler and Coller in 1954,12 is obsolete for clinical practice even though it is still used sporadically. Depth of tumour invasion through the bowl wall, extent of regional lymph node involvement, and the finding of distant metastases remain the major aspects of a valid staging system. The well established basis for colorectal cancer staging and for prediction of five year survival is the tumour-node-metastases (TNM) system of the International Union against Cancer (UICC) (table 1, fig 2).13
Tumour-node-metastases (TNM) staging system for colorectal cancer (survival data from Greene and colleagues14)

A 62 year old patient with rectal cancer. (A) Rectoscopic image of endoluminal tumour. (B) Endoscopic ultrasound showing invasion through the muscularis propria (T3). (C) Schematic view of the mucosal layers and staging patterns.
ADJUVANT THERAPY: COLON CANCER
Who is eligible for adjuvant treatment?
The prerequisite for adjuvant treatment of colon cancer is complete surgical resection of the primary tumour lesion. The aim of adjuvant chemotherapy in colon cancer is to prevent local recurrence or distant metastases and to prolong survival. Several large scale prospective studies demonstrated the beneficial effect of fluorouracil based adjuvant chemotherapy15–18 for patients with stage III colon cancer (any T stage with positive lymph nodes). Pooled analysis from seven clinical trials of adjuvant fluorouracil based therapy showed an increase in the probability of remaining free of tumour recurrence after five years from 42% to 58%; the likelihood of five year overall survival increased from 51% to 64% for patients with stage III disease.9 Since the beginning of the 1990s, chemotherapy with fluorouracil and leucovorin has been widely accepted as the clinical standard in the treatment of patients with stage III colon cancer. Due to the lack of convincing study results it is not routinely recommended in stage II colon cancer (T3 or T4 with negative lymph nodes)19,20 but should be considered for high risk stage II patients. A useful tool for risk evaluation and decision making in the choice of adjuvant therapy is available through the Mayo Clinic website (http://www.mayoclinic.com/calcs). Even though older patients have been underrepresented, in most clinical trials this important group also benefits from adjuvant chemotherapy and should not be excluded from treatment as long as general contraindications are considered carefully.21 Adjuvant radiotherapy is not recommended in colon cancer.22
Adjuvant protocols: fluorouracil-leucovorin based regimens
Fluorouracil based therapies (for example, the MAYO protocol) are well established for patients with stage III disease. Except for a change in treatment duration from 12 to six months,18 these adjuvant therapy regimens have not altered significantly during the past 10 years. Several protocols using the monoclonal antibody edrecolomab23 or levamisole in exchange for leucovorin24,25 failed to demonstrate superiority when compared with the standard fluorouracil-leucovorin treatment. But with the successful introduction of irinotecan and oxaliplatin in the palliative treatment area, these agents became of interest in the adjuvant setting also, raising two major questions: do patients with stage II disease benefit from adjuvant therapy, and which is the most effective treatment protocol in the adjuvant setting?
The camptothecin alkaloid derivative irinotecan and the platinum derivative oxaliplatin are mainly integrated in current adjuvant clinical trials because of their favourable response rates in advanced colorectal cancer. The group of oral fluoropyrimidines promises equal potency but less effort than parenteral fluorouracil application. Also, implementation of targeted therapies into adjuvant protocols is considered additive potentiation of the antitumour effects.
At least four clinical trials are currently investigating the integration of oxaliplatin or irinotecan into adjuvant treatment regimens.
Adjuvant protocols: irinotecan and oxaliplatin
The intergroup trial CALGB C89803, which assigned 1264 patients with stage III disease to receive either irinotecan plus bolus fluorouracil and leucovorin (IFL) or bolus fluorouracil and leucovorin, had to be stopped because of increased toxicity (diarrhoea and myelosuppression) and a high early death rate in the IFL group. After a median follow up period of 2.6 years, IFL therapy did not improve either the probability of recurrence or overall survival.26 The outcome of a European trial (PETACC3/V-307) comparing irinotecan, infusional fluorouracil, and leucovorin (FOLFIRI) with infusional fluorouracil and leucovorin has not yet been reported.
In the MOSAIC trial, 2246 patients with stage II (40%) and stage III (60%) colon cancer received either oxaliplatin, infusional fluorouracil, and leucovorin (FOLFOX) or infusional fluorouracil and leucovorin for six months.27 The FOLFOX treated cohort had a greater likelihood of remaining free of recurrence after four years (76% v 69%; p<0.001).28 This difference was far more evident among patients with stage III disease (70% v 61%; p = 0.002) than among those with stage II disease (85% v 81% percent; NS). In terms of overall survival, a statistically significant advantage of the FOLFOX protocol has not yet been reported. Grade 3 neuropathy (that is, limiting the activities of daily living) occurred in 12% of patients receiving FOLFOX but was consistent in only 1% of patients after one year. These results have expanded the options for treating patients in the adjuvant setting and the FOLFOX protocol may become the new standard treatment. However, the risks and benefits of this more toxic regimen need to be carefully assessed in individual patients.
-
Integration of irinotecan and oxaliplatin into adjuvant protocols is under investigation.
-
The FOLFOX protocol demonstrated its efficacy in the adjuvant setting but overall survival has not yet been improved in the investigated population.
Adjuvant protocols: oral fluoropyrimidines
The use of the oral fluoropyrimidines capecitabine and uracil/tegafur (UFT) in the adjuvant treatment of colon cancer was investigated in two randomised phase III studies. In the NSABP-C06 study, 1608 patients with stage II and III disease were assigned to receive either UFT-leucovorin or fluorouracil-leucovorin. Disease free survival was 66.9% for UFT and 68.3% for fluorouracil-leucovorin. Five year overall survival was 78.7% for both groups. Capecitabine was compared with fluorouracil-leucovorin in the X-ACT trial, including 1987 patients with stage III disease. The capecitabine group showed an improved safety profile and recurrence free survival in stage III patients. No difference was seen in overall survival. Even though there is no study comparing UFT and capecitabine directly, these data allow the conclusion that capecitabine is the favourable agent in this setting due to its superior safety profile and slightly improved disease free survival. Therefore, the MAYO protocol will be replaced by capecitabine. There are no data for incorporation of targeted therapies into adjuvant treatment protocols. Future studies are underway to address this point.
-
Capecitabine appears to be a safe and efficient alternative to fluorouracil in the adjuvant setting.
-
The role of targeted therapies for adjuvant treatment has not yet been evaluated.
Treatment of stage II disease
The impact of adjuvant therapy on stage II disease was addressed in two recent phase III studies. The CLAGB-9581 trial assigned more than 1700 patients with stage II colon cancer to either surgery followed by adjuvant treatment with the monoclonal antibody edrecolomab (17-1A) or surgery alone.29 Results showed that edrecolomab did not appear to prolong overall survival or failure free survival in the treatment group.
The first evidence for the benefit of adjuvant chemotherapy in stage II disease comes from the QUASAR study that randomised 3238 patients to either fluorouracil-leucovorin or follow up after R0 resection (91% stage II, 71% colon cancer) over a period of nine years.30 The rate of recurrence after five years was 22.2% in the treatment group and 26.2% in the control group. Five year overall survival was 80.3% versus 77.4%. Due to the large number of patients, a small but significant advantage of 3% in overall survival was shown for the first time in patients with stage II disease.
-
Adjuvant chemotherapy of patients with stage II disease remains controversial. Treatment decisions should be based on the patient’s individual risk profile.
ADJUVANT THERAPY: RECTAL CANCER
Radiotherapy and radiochemotherapy
While colon cancer has a propensity to recur in distant sites, local recurrence after curative surgical resection is a major problem in rectal cancer. It mainly determines the patient’s prognosis and can lead to extensive local complications such as bowl obstruction and irrepressible pain. Prevention of local recurrence therefore is one of the most important objectives in the treatment of resectable rectal cancer.
Even though introduction of the total mesorectal excision (TME) as a new surgical technique has led to a significant decrease in local recurrence rates,31 it does not produce an acceptable level of local tumour control. Radiation therapy and chemotherapy are administered to improve local tumour control, decrease morbidity, and prolong survival through further reduction of local recurrence.32
For patients with stage II (T3/4 N0) and stage III (TX N1) rectal cancer, adjuvant (postoperative) radiochemotherapy was considered the standard treatment because it improved local control and overall survival compared with surgery alone or surgery plus radiation.33 Neoadjuvant protocols were mainly used for advanced tumours (T4), aiming to achieve subsequent curative resection by decreasing tumour size. This strategy has seen some refinement recently as stage II and III patients appear to benefit from preoperative (that is, neoadjuvant radiation) or radiochemotherapy through improved local tumour control and lower morbidity.34
In the Dutch CKVO 95-04 trial, TME combined with short term preoperative radiation (5×5 Gy) was compared with surgery alone. After a median follow up of two years, local recurrence rate was 2.4% in the radiation group compared with 8.2% in the control group (p<0.001). An improvement in overall survival could not be shown. The conclusions from this important trial were that preoperative radiotherapy reduces the risk of local recurrence in low (inferior margin <10 cm from the anal verge) but not in high rectal cancers and that it is only beneficial in stage II and III tumours.32 A cost-utility analysis conducted by the same study group in later years also showed that preoperative short term radiation is cost effective.35
The recently published German CAO/ARO/AIO-94 trial36 compared preoperative with postoperative long term radiochemotherapy (50.4 Gy/ plus continuous infusion of fluorouracil) in 823 patients with resectable rectal cancer. Local recurrence rate after five years was lower in the preoperative treatment group (6% v 13%; p = 0.006) while the frequency of distant metastases and survival showed no significant difference. Preoperative treatment was associated with an impressive decrease in toxicity (grade 3 or 4 toxic effects 27% v 40% postoperative). Postoperative staging suggested a downstaging effect of preoperative radiochemotherapy and patients with low lying tumours showed an increased rate of sphincter preservation after preoperative treatment.
These data on preoperative radiation and radiochemotherapy lead to the conclusion that preoperative strategies are the favourable treatment option for patients with resectable rectal cancer but further studies comparing short term with long term neoadjuvant radiation are needed. The role of postoperative chemotherapy in patients who undergo neoadjuvant radiation also needs to be clarified. This issue is currently being addressed by the EORTC-study 22921.37 Alternative ways of administering chemotherapy, such as continuous and chronomodulated infusion of fluorouracil, as well as integration of the new drugs capecitabine, oxaliplatin, and irinotecan into neoadjuvant protocols, have yet to be determined in terms of therapeutic relevance.
-
Preoperative treatment strategies are advantageous in the adjuvant setting but further evaluation of application mode and choice of combined chemotherapeutic agents is needed to define standard protocols.
PALLIATIVE THERAPY: COLORECTAL CANCER
The aim of palliative systemic therapy is to improve survival and quality of life in patients with advanced colorectal cancer. Showing superiority compared with best supportive care with regard to overall survival,38 fluorouracil based palliative chemotherapy was the only choice for decades. Fluorouracil can be applied as parenteral bolus or continuous infusion. Because of its favourable safety profile, continuous infusion of fluorouracil has become the clinical standard. The de Gramont (leucovorin 200 mg/m2, bolus fluorouracil 400 mg/m2 followed by a fluorouracil 22 hours 600 mg/m2 for two consecutive days every two weeks) and AIO (weekly fluorouracil 2600 mg/m2/24 hours + leucovorin 500 mg/m2 30 minutes intravenously) regimens are well established infusional protocols with a median survival of >14 months.39,49
-
Palliative chemotherapy prolongs survival and should be available for every patient with advanced colorectal cancer. Older patients without clinical contraindications benefit likewise and should not be excluded from treatment.
Considerable progress has been made during the past 10 years through the clinical introduction of new drugs that are effective in the treatment of advanced colorectal cancer. Implementation of combination protocols using oxaliplatin or irinotecan with standard fluorouracil-leucovorin has led to a significant improvement in overall survival. Today, combination and sequential application of the available agents allows effective treatment even for patients showing progressive disease after initial or even secondary palliative therapy. An additional increase in the effectiveness of systemic therapies can be expected from the new group of drugs targeting specific cellular pathways essential for tumour growth, cell survival, and metastases.
Irinotecan and oxaliplatin in advanced colorectal cancer
The camptothecin derivative irinotecan is acting through inhibition of the enzyme topoisomerase, thereby blocking DNA replication.40 The toxic effects of irinotecan include diarrhoea, myelosuppression, nausea/vomiting, and alopecia. Delayed onset diarrhoea is the most common toxicity and has to be treated immediately with loperamide to avoid serious complications. In secondline therapy after previous application of fluorouracil-leucovorin, monotherapy with irinotecan is superior compared with best supportive care and continuous fluorouracil infusion.41,42 In the firstline setting, a combination of irinotecan with fluorouracil-leucovorin (bolus or continuous infusion) leads to a significant increase in response rate, progression free survival, and overall survival compared with standard fluorouracil-leucovorin.43,44
Oxaliplatin is a third generation platinum derivative. It works synergistically with fluorouracil,45 leads to bulky DNA adducts, and induces cellular apoptosis.46 The toxicity profile of oxaliplatin differs from that of other platin compounds used in medical oncology. The most frequent toxicity includes two dose limiting neurological syndromes: a transient, cold induced, sensory neuropathy characterised by dysesthesias and paresthesias occurring during or soon after infusion, and a delayed dose dependent neuropathy escalating in partial or complete functional loss of sensory function. Neuropathy is reversible in most patients a few months after withdrawal from oxaliplatin treatment.
The effectiveness of oxaliplatin as a single agent in first- or secondline palliative therapy is limited.47,48 Clinical benefit has been demonstrated in combination with infusional fluorouracil-leucovorin (FOLFOX). Several randomised trials have consistently shown that FOLFOX therapy results in superior response rates and time to disease progression in comparison with fluorouracil-leucovorin given as first- or secondline therapy in metastatic colorectal cancer.49–51
-
Irinotecan and oxaliplatin, each in combination with fluorouracil, are the new standard in the palliative treatment of colorectal cancer.
Because of their superior effectiveness, triplet therapies consisting of either irinotecan or oxaliplatin in combination with infusional fluorouracil-leucovorin have become the standard treatment in the palliative situation.
Direct comparison of irinotecan and oxaliplatin in combination with fluorouracil and leucovorin for the initial treatment of metastatic colorectal cancer has recently been reported. In a multicentre trial conducted in North America, 795 patients were randomly assigned to receive either irinotecan + bolus fluorouracil-leucovorin (IFL), FOLFOX, or a combination of irinotecan with oxaliplatin (IROX).52 Patients treated with FOLFOX had a response rate, time to disease progression, and overall survival time that was superior to those observed with either IFL or IROX. An imbalanced availability of secondline agents may have influenced the superiority of FOLFOX because 60% of patients initially treated with FOLFOX subsequently received irinotecan, whereas only 24% in the IFL group were subsequently given oxaliplatin. None the less, these data support the option of oxaliplatin based therapy as firstline combination therapy for patients with metastatic disease.
Two European trials with predefined crossover designs have further addressed this issue. Tournigand et al, whose randomised study included 220 patients, found that a regimen of infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) followed by FOLFOX led to equal response rates and median overall survival times compared with those obtained with the crossover regimen of FOLFOX followed by FOLFIRI.53 In a similarly designed trial involving 161 patients, Grothey et al found no significant differences in efficacy between capecitabine combined with irinotecan and capecitabine combined with oxaliplatin.54 Definitive interpretation of these studies is limited by the small number of patients but the consistency of the results suggests at least equivalence between irinotecan based and oxaliplatin based regimens when combined with comparable fluorouracil therapies.
According to the available data, the optimal sequence of these protocols remains unclear. The choice of initial therapy therefore should take into account the patient’s coexisting medical condition at baseline. For patients with underlying neuropathy, irinotecan based regimens may be more appropriate than oxaliplatin based regimens, whereas for patients with underlying bowel dysfunction, oxaliplatin based therapy may be more appropriate than treatment with irinotecan. Despite the choice of initial therapy, exposure to each of these cytotoxic agents at some time over the course of a patient’s disease has been associated with prolonged survival and should therefore be available for every suitable patient in the palliative situation (fig 3).55

Median overall survival (mOS) correlates with the number of applied substances. Adapted from Grothey et al 2004.55 5-FU, 5- fluorouracil; LV inf, leucovorin infusion.
Oral fluoropyrimidines in the palliative treatment of advanced colorectal cancer
The use of oral fluoropyrimidines substituting parenteral fluorouracil promises an additional advancement of therapeutic options in the palliative situation. Capecitabine and UFT have been compared with the standard bolus fluorouracil-leucovorin regimen in firstline therapy of metastatic colorectal cancer, with two studies for each compound, including more than 2300 patients. UFT demonstrated equal efficacy but shorter progression free survival (PFS)56,57 while capecitabine showed higher response rates and comparable PFS and overall survival.58,59 Median survival did not differ in any of the studies. The advantages of oral fluoropyrimidines are seen in their safety profile and improvement in quality of life through the more convenient mode of application.
The question of whether oral fluoropyrimidines will be able to replace infusional fluorouracil as part of the triple protocols will be answered from the results of several ongoing trials. First results of interim efficacy and safety analysis from a study comparing FUFOX (weekly fluorouracil 2000 mg/m2 24 hour infusion, leucovorin 500 mg/m2, oxaliplatin 50 mg/m2) with CAPOX (capecitabine 1000 mg/m2 twice daily for days 1–14, oxaliplatin 70 mg/m2 on days 1 and 8; every three weeks) in 399 patients showed that CAPOX had a comparable efficacy and toxicity profile to FUFOX in the firstline treatment of advanced colorectal cancer.60 Time to progression was eight months in the FUFOX group and 7.5 months in the CAPOX group. Final data will be presented at the ASCO meeting this year. In a phase II single arm trial including 96 patients with metastatic colorectal cancer, the XELOX regimen (oxaliplatin 130 mg/m2 every three weeks/capecitabine 2000 mg/m2 for two weeks) was used as firstline treatment and showed excellent response rates and median survival (55% and 19.5 months, respectively) with low rates of myelotoxicity.61 These results suggest that oxaliplatin combined with capecitabine is a safe and effective protocol for the treatment of metastatic colorectal cancer. Data from phase III studies investigating this regimen are underway.
-
Oral fluoropyrimidines are on their way towards displacing fluorouracil in standard protocols. However, final data have to be awaited.
Secondary resection of liver metastases following systemic therapy
The new irinotecan or oxaliplatin based combination protocols achieve high response rates, especially in metastases that were initially judged unresectable (fig 4). This increased efficacy of systemic treatment often enables secondary resection of hepatic or pulmonary metastases. For liver metastases, secondary resection has demonstrated equal potential in terms of five year survival rates as primary curative resection (25–35%). Studies addressing this point show that 15–20% of patients with metastatic colorectal cancer are eligible for secondary curative resection.62,63 With respect to this curative option, every patient with metastatic disease receiving systemic therapy should therefore be carefully monitored as the chance for secondary curative resection may develop in the course of palliative treatment.

A 54 year old patient with advanced cancer of the ascending colon. (A) Multiple liver metastasis at first diagnosis. (B) Regression after four months of FOLFOX4 (oxaliplatin, infusional fluorouracil, and leucovorin) + bevacizumab.
-
Secondary resection of metastases as a curative option should be considered in patients with a good response to palliative treatment.
TARGETED THERAPIES
Basic research has led to identification of molecular sites in tumour tissue that may serve as specific targets for therapeutic intervention. Several new drugs that aim to interrupt molecular pathways leading to increased proliferation, escape from apoptosis, angiogenesis, and tumour spreading to distant sites are under development. They are targeting growth factors, their receptors, or intracellular proteins involved in important signalling cascades (fig 5). Some of these targeted therapies have already proved to be efficacious in phase II and III trials. The monoclonal antibody against vascular endothelial growth factor (VEGF), bevacizumab, and the monoclonal antibody against epidermal growth factor receptor (EGFR), cetuximab, have been approved by the FDA and European authorities for the treatment of metastatic colorectal cancer. Other compounds, namely tyrosine kinase inhibitors that block downstream signalling through inhibiting phosphorylation of signal proteins, have been extensively tested in clinical trials and may enter clinical practice soon. The major substances relevant for the treatment of colorectal cancer will be discussed in this section.
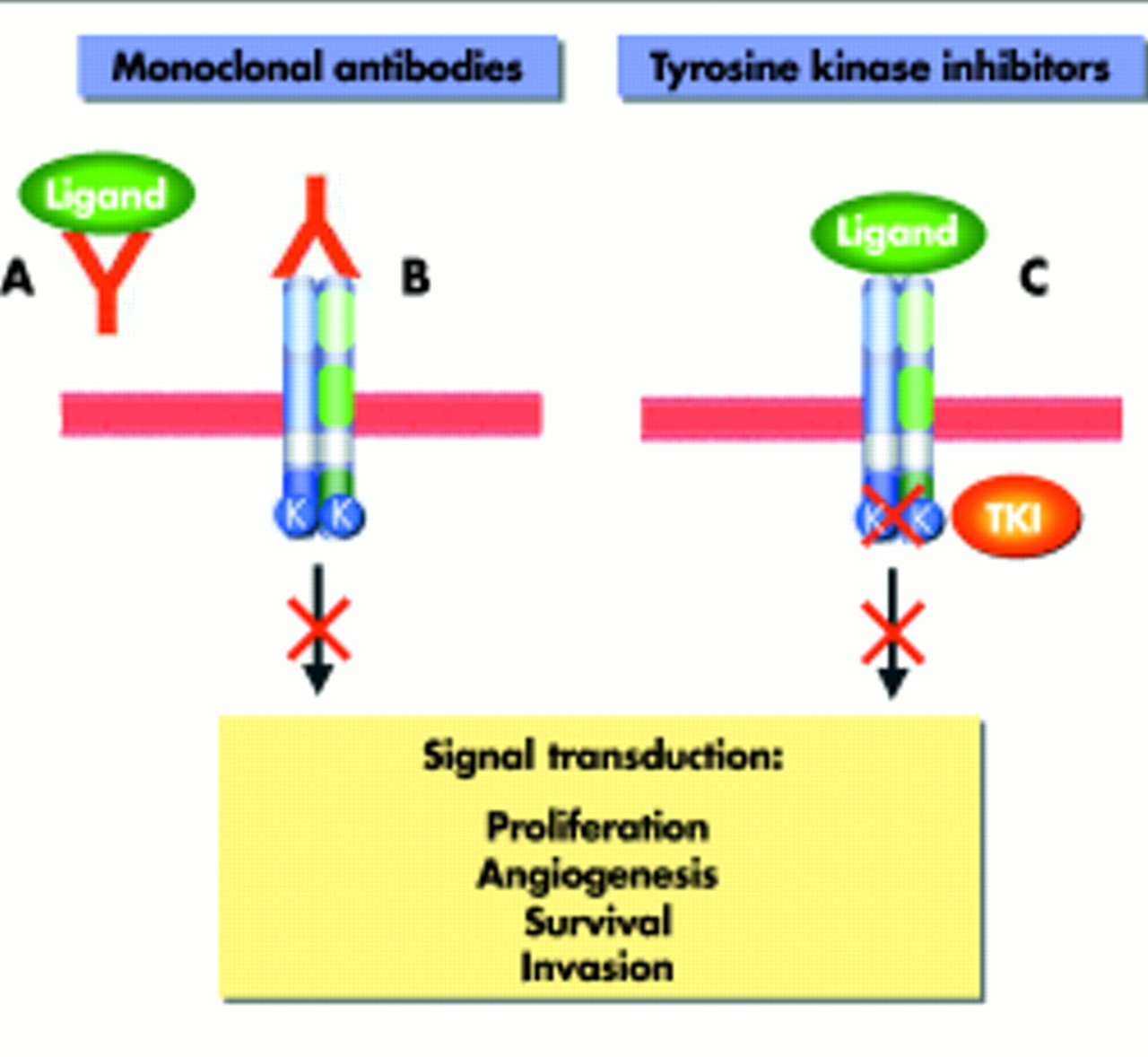
Schematic overview of target structures for monoclonal antibodies (mAbs) and tyrosine kinase inhibitors (TKI). (A) MAbs bind to soluble ligand and thereby inhibit receptor activation (for example, bevacizumab). (B) MAbs block the ligand binding site at the receptor (for example, cetuximab). (C) TKI bind to the catalytic area of the intracellular kinase domain (for example, erlotinib, gefitinib).
Targeting the EGF receptor: cetuximab
EGFR is a tyrosine kinase receptor from the ErbB/HER family. The receptor is a membrane protein of epithelial cells and is overexpressed in a variety of tumours. Its activation initiates signal transduction cascades that promote cell division, migration, angiogenesis, and inhibition of programmed cell death.64 EGFR signalling is therefore a promising target for interfering with cellular pathways crucial for tumour growth and migration. Several strategies have been developed to target EGFR. Most advanced in clinical development are monoclonal antibodies blocking ligand binding or receptor homeo/heterodimerisation and low molecular weight tyrosine kinase inhibitors, so called small molecules, that inhibit intracellular catalytic domains of the EGFR. Cetuximab, originally described as monoclonal antibody C-225, is a humanised monoclonal antibody directed against the extracellular binding domain of EGFR and is the first inhibitor in its class that has been approved in the United States and Europe for the treatment of advanced colorectal cancer.
In preclinical studies, cetuximab showed activity against tumour growth if used as a single substance but interestingly a synergistic effect was observed when it was combined with irinotecan, even in tumour cells already resistant to irinotecan. These findings suggested that the antibody may overcome cellular resistance to irinotecan.65 In a phase II study, 121 patients with advanced colorectal cancer previously unresponsive to irinotecan received a combination of cetuximab and irinotecan as palliative treatment.66 Sixty patients were treated with cetuximab alone.
The combination group showed objective tumour responses in 19% compared with 10% in the monotherapy group. These results were confirmed by an extended phase II trial, the so-called BOND study (for Bowel Oncology with Cetuximab Antibody). A total of 579 patients with irinotecan refractory advanced colorectal cancer were screened for expression of EGFR in primary tumour specimens. Finally, 329 patients showing positive EGFR expression were randomly assigned to receive either cetuximab alone or in combination with irinotecan.67 Showing a response rate of 23% in the combination group and 11% in the monotherapy group (p = 0.007) the reported results clearly demonstrated the significant superiority of the combination regimen (table 2). Cetuximab has therefore been approved for salvage therapy in the treatment of advanced colorectal cancer. The main side effect of cetuximab is an acne-like skin rash which interestingly correlates with treatment response.68 The degree of receptor expression did not show a significant correlation with response rates in the available studies and should no longer be used to select patients for cetuximab therapy.67,69 Current clinical trials are expanding the possible combination of cetuximab with chemotherapy as well as with bevacizumab.70
Combination of chemotherapy and targeted therapy in clinical trials
Targeting VEGF: bevacizumab
Angiogenesis, the formation of new blood vessels, is a prerequisite for tumour growth beyond a diameter of 1–2 mm3.71 VEGF is the most potent and specific angiogenic growth factor and is overexpressed in many tumours. Bevacizumab is a humanised monoclonal antibody against VEGF that exerts its antiangiogenic effect through neutralisation of circulating VEGF.
The efficacy of bevacizumab in the treatment of colorectal cancer was initially demonstrated in a randomised phase II study that compared bevacizumab at two dose levels (5 and 10 mg/kg every two weeks) in combination with fluorouracil-leucovorin versus fluorouracil-leucovorin alone as firstline therapy.72 The combined treatment showed a significant increase in response rates (40% v 17%; p = 0.029) and median time to progression (9 v 5.2 month). Interestingly, this positive effect was reported for the group with the lower bevacizumab dose (table 2).
These results led to two concurrent randomised phase III trials. The first trial conducted by Hurwitz et al randomised 815 patients with metastatic colorectal cancer for firstline treatment with either irinotecan + bolus fluorouracil-leucovorin (IFL) + bevacizumab or IFL + placebo.73 Patients in the bevacizumab group experienced a significant increase in response rate (44.8% v 34.8%) and median overall survival (20.3 months v 15.6 months; p<0.001). The second smaller trial enrolled patients that were considered unable to tolerate irinotecan for treatment with bevacizumab + fluorouracil- leucovorin versus fluorouracil- leucovorin.74 The results also showed an increased response rate and extended time to tumour progression but did not prolong median survival (table 2). The combination regimens with bevacizumab were well tolerated, and application of bevacizumab was associated with mild proteinuria and reversible hypertension. However, rare cases of non-specific gastric perforation have been reported from ongoing studies that may be related to bevacizumab treatment.
-
Cetuximab and bevacizumab have changed the paradigm of systemic cancer treatment and will experience increasing incorporation into clinical routine.
After being approved by the FDA for every firstline treatment containing fluorouracil-leucovorin, European authorities followed with a more restricted approval (firstline must contain fluorouracil-leucovorin/combination only with irinotecan) early this year. Phase III data demonstrating comparable data for the combination of bevacizumab with FOLFOX in the firstline setting will soon be available. In the secondline therapy results from the combination of bevacizumab with FOLFOX already reported a statistically significant prolongation of median survival was found.75 Study designs for combination with oral fluoropyrimidines + oxaliplatin or irinotecan and bevacizumab will further establish the role of bevacizumab in the palliative setting as well as the adjuvant treatment area.
Tyrosine kinase inhibitors
Several studies are actively investigating the effect of tyrosine kinase inhibitors (TKIs) in patients with advanced colorectal cancer. Most available data come from studies using the EGFR specific TKIs erlotinib (OSI-774, Tarceva) or gefitinib (ZD1839, Iressa). In initial phase I studies, no single agent response was observed for erlotinib or gefitinib but approximately 30% of the enrolled patients experienced stable disease.76,77
In contrast, combination of gefitinib with FOLFOX as firstline chemotherapy in a small phase II study showed an impressive tumour response rate of 73%.78 A recently reported phase I study combining FOLFIRI with erlotinib in the treatment of patients with advanced colorectal cancer was terminated due to excessive toxicity at reduced doses.79 How TKIs will find their way into clinical application will be determined through further results from ongoing clinical trials.
PERSPECTIVES AND CHALLENGES
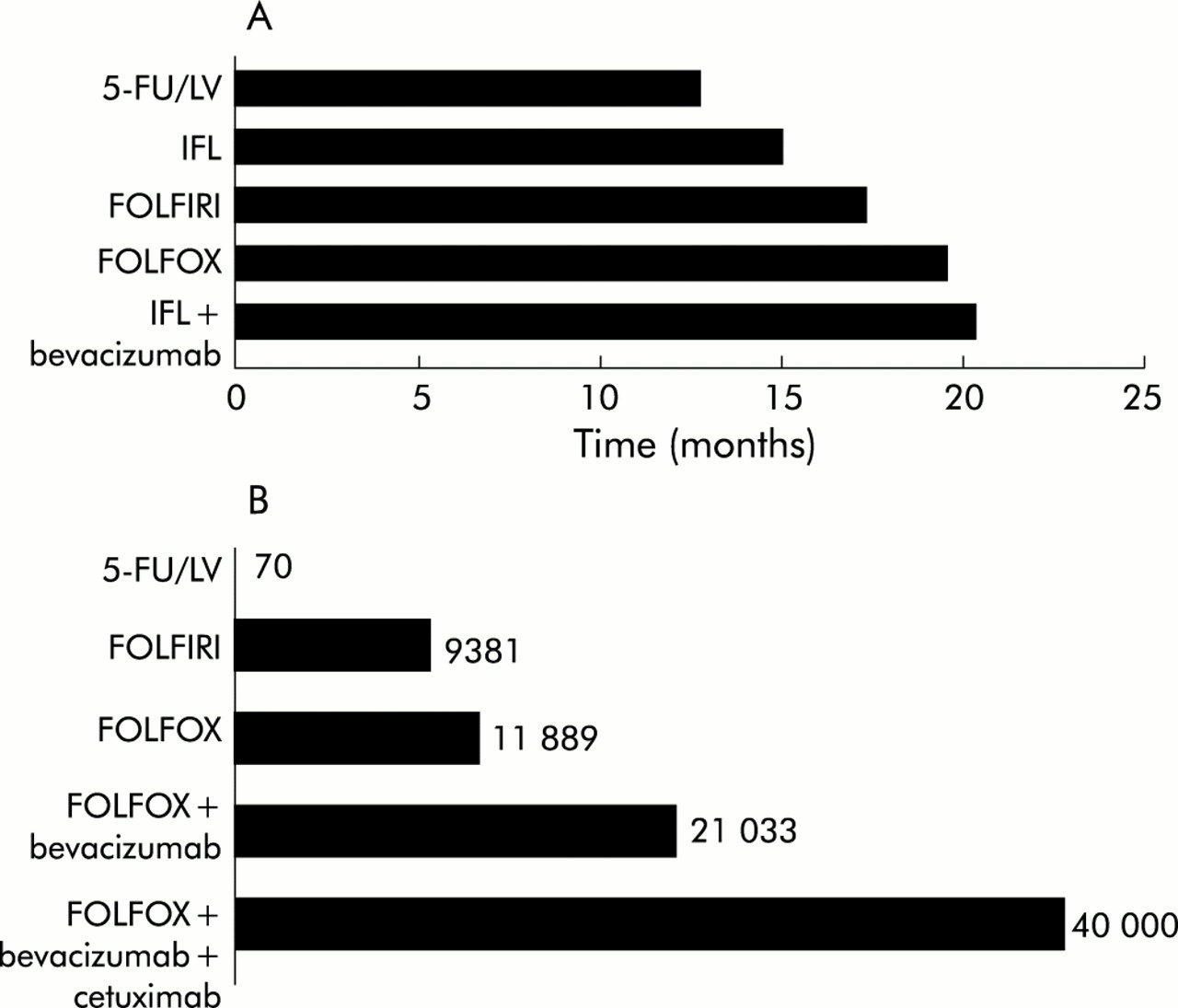
Progress in the systemic treatment of colorectal cancer is evident, not only because of the significant increase in life expectancy in advanced colorectal cancer. It has become possible mainly through the consequent and broad clinical introduction of irinotecan and oxaliplatin, agents which should now be embraced as standard chemotherapy treatment. Oral fluoropyrimidines are on their way towards replacing parenteral fluorouracil application not only in single drug regimens but also in the new and effective combination protocols. Also, the innovative concepts of targeted therapies against VEGF and EGFR have entered clinical treatment. How therapy standards will emerge from the current multiplicity of possible combinations cannot be answered at present. Rapid approval of multiple active substances has made the design and completion of clinical trials to answer this question difficult. It has also led to uncertainty in the choice of which therapy to choose at what time and in which combination. Also, escalating costs caused mainly by the use of targeted therapies will seriously challenge the already restricted resources of public healthcare (fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Overall survival data from randomised phase III firstline trials. (B) Estimated costs for firstline systemic therapy in advanced colorectal cancer. Costs are calculated for a treatment course of eight weeks (patient 75 kg/175 cm) in US dollars. 5-FU, 5- fluorouracil; LV, leucovorin; IFL, irinotecan, fluorouracil, and leucovorin; FOLFIRI, irinotecan, infusional fluorouracil, and leucovorin; FOLFOX, oxaliplatin, infusional fluorouracil, and leucovorin.
Carefully defined individual treatment indications using yet to be developed predictive tools are urgently needed to address this problem. In conclusion, further progress is on the horizon but can only take place through interdisciplinary cooperation and careful design, and completion of randomised clinical trials.
Acknowledgments
We thank Professor Dr Markus Reiser, Ruhr-Universität Bochum, for provision of endoscopic and endosonographic images.
REFERENCES
Supplementary materials
Competing interest: WS received lecture fees from Hoffmann-LaRoche, Sanofi-Aventis, and Astra-Zeneca.