Article Text

Abstract
Prognostication of newly diagnosed colorectal cancer (CRC) predominantly relies on stage as defined by the UICC-TNM and American Joint Committee on Cancer classifications. Tumour extent, lymph node status, tumour grade and the assessment of lymphatic and venous invasion are still the most important morphological prognostic factors. Evidence suggests that tumour budding and tumour border configuration are important, additional histological parameters but are not regarded as essential in prognosis. Although several molecular features, such as LOH18q and TP53 mutation analysis, have shown promising results in terms of their prognostic value, the American Society of Clinical Oncology Tumor Markers Expert Panel does not currently recommend their use in routine practice. cDNA-microarray, PCR and fluorescence in situ hybridisation are now frequently used to identity potential prognostic indicators in CRC, but the applicability of these methods in routine use is likely to have limited impact. Reliable prognostic markers identified by immunohistochemical protein profiling have yet to be established. Randomisation of data sets, assessment of interobserver variability for protein markers and scoring systems, as well as the use of receiver operating characteristic curve analysis in combination with multimarker-phenotype analysis of several different markers may be an effective tactical approach to increase the value of immunohistochemical findings. This article reviews the well established and additional prognostic factors in CRC and explores the contribution of molecular studies to the prognostication of patients with this disease. Additionally, an approach to improve the prognostic value of immunohistochemical protein markers is proposed.
Statistics from Altmetric.com
Colorectal cancer (CRC) is one of the most common malignancies in the western world.1 In the European Union, the incidence and mortality of CRC are 58/100 000 and 30/100 000 per year, respectively.2 Despite improvements in surgical techniques, dosing and scheduling of adjuvant and neo-adjuvant therapy, the 5-year survival rate for patients with CRC ranges from 90% to 10% with tumour progression.3 Prognostication of newly diagnosed CRC predominantly relies on stage or anatomic extent of disease based on the International Union Against Cancer (UICC-TNM)4 and American Joint Committee on Cancer (AJCC)5 staging classifications. However, CRC should be regarded as a heterogeneous, multi-pathway disease, an observation substantiated by the fact that histologically identical tumours may have neither similar prognoses nor similar response to therapy.6 Molecular analysis and protein markers are currently being investigated as a means to improve the identification of patients likely to have a poor clinical outcome and therefore more possibly benefiting from adjuvant treatment.7–9 Immunohistochemistry studies have yielded disappointing results, and several responsible factors have been identified.10–12
The aims of this review are: (1) to summarise the well established and additional prognostic factors in CRC; (2) to explore the contribution of molecular studies in determining prognosis; and (3) to focus on the sources of discrepancy in immunohistochemical prognostic studies, and outline an approach to improve the prognostic value of immunohistochemical protein markers.
WELL ESTABLISHED AND ADDITIONAL PROGNOSTIC FACTORS
TNM category
The UICC/AJCC tumour node metastasis (TNM) stage remains the gold standard of prognostic factors in CRC.4 The 5-year survival rate for patients with CRC is largely dependent on TNM stage. The TNM staging system was initially developed to predict prognosis, but its function has expanded to aid in the choice of treatment and in the selection of patients for clinical trials.13 The latest revision of the TNM staging manual includes the subdivision of stage II disease into IIA (T3 N0 M0) and IIB (T4 N0 M0).5 Patients with IIB have a considerably worse prognosis than patients with IIIA, though the latter are frequently treated with adjuvant therapy. While adjuvant therapy is widely accepted in the treatment of stage III disease, patients with stage II are not yet recommended for this treatment protocol.14
Accurate analysis of regional lymph nodes is one of the most important issues for an optimal pathological staging in CRC. Although special techniques such as immunohistochemistry can facilitate the detection of isolated tumour cells in regional lymph nodes, at present the AJCC, UICC, and the College of American Pathologists (CAP) continue to recommend standard H&E techniques for the pN assessment in CRC. Changes in these recommendations seem to be under consideration, but will be definitively based on the validation of immunohistochemical and molecular analysis by outcome investigation.15
Venous and lymphatic invasion
In addition to TNM stage, several other tumour-related features have been identified as essential or important prognostic factors.16 Venous and lymphatic invasion represent crucial steps in the formation of micro-metastases and eventually macroscopic tumour growth at a secondary site. Several studies have identified both these features as independent adverse prognostic factors in multivariable analysis.17–19 However to date, no widely accepted standards or guidelines for the pathological evaluation of vessel invasion are in place.20
Tumour grade
Tumour grade is an additional prognostic factor in CRC, and its grading system is based on the percentage of gland formation.15 The proposal of different grading systems18 21 22 complicates a meta-analysis and an appropriate determination of the prognostic significance of tumour grade in CRC.
Tumour budding
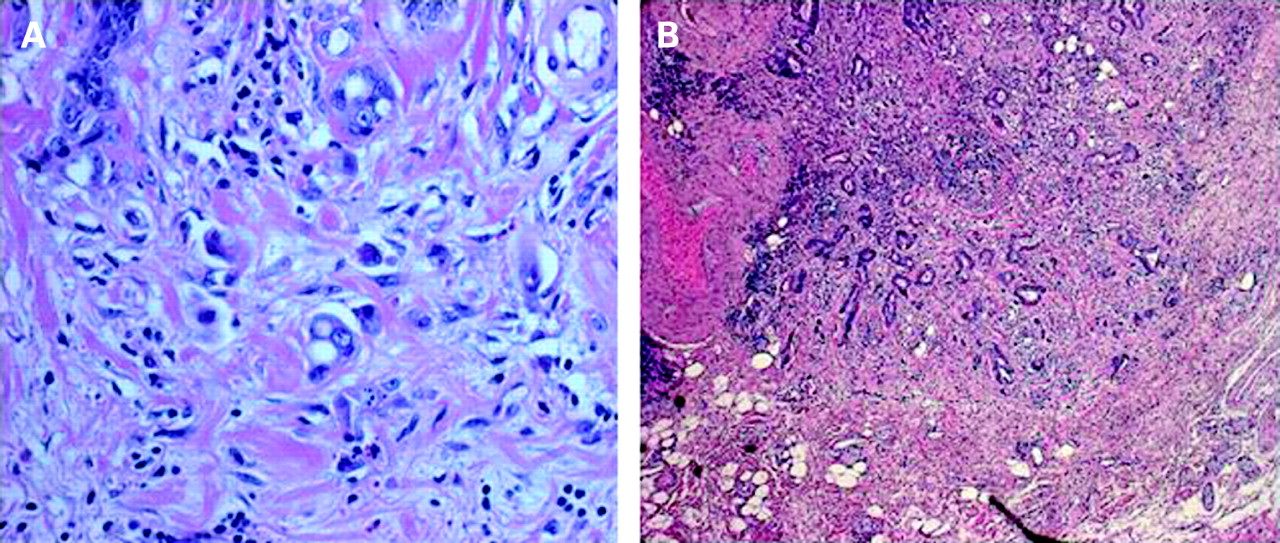
Tumour budding is described as a transition from glandular structures to single cells or clusters of up to four cells at the invasive margin of CRCs.23 Tumour buds have the properties of malignant stem cells, including the potential for re-differentiation both locally and at sites of metastasis.24 Tumour budding is diagnosed at high magnification (fig 1A) and must be clearly discriminated from the tumour border configuration (infiltrative versus pushing) which is diagnosed at low magnification (fig 1B).24 Several studies have shown that tumour budding is an independent risk factor of local spread, lymph node and distant metastasis, recurrence, and worse survival following curative surgery.25–30 Quantified data of tumour budding and podia formation have been related to KRAS mutational status, a feature described in about 30% of CRCs.31 Absence of tumour budding is also correlated with the presence of intratumoural lymphocytes (TILs) and peritumoural lymphocytes (PTLs), suggesting an immune reaction responsible for destruction of buds and therefore improved prognosis.30 Recently cytokeratin immunohistochemical stains were suggested in cases where an inflammatory reaction obscures the presence of tumour buds on H&E staining.15

Tumour border configuration
This morphological feature was originally described by Jass et al and seems to be a stage-independent adverse prognostic factor.32 33 Tumour border configuration is distinct from tumour budding, although it is more often associated with an infiltrative margin.15
MOLECULAR PROGNOSTIC FACTORS
Microsatellite instability
Approximately 75–85% of CRCs arise through the chromosomal instability (microsatellite stable, MSS) pathway characterised by aneuploidy, allelic losses, amplifications, translocations and mutation of APC, KRAS and TP53.34 Although the prognosis of patients with MSS CRC is stage and grade dependent, tumours with identical morphological features display considerable heterogeneity in terms of clinical outcome. The remaining 15–20% of CRCs have high frequency microsatellite instability (MSI-H) characterised by inactivation of mismatch repair (MMR) genes.35 Sporadic MSI-H cases have been shown to arise through promoter hypermethylation and silencing of the hMLH1 gene.36 The autosomal dominant condition hereditary non-polyposis colorectal cancer (HNPCC) is believed to account for 5–15% of CRCs and typically demonstrates MSI-H due to germline mutations in one of the DNA MMR genes.37 Tumours with MSI-H tend to be more proximally located, poorly differentiated, of mucinous histological type, show considerable lymphocytic infiltration, and have been linked with TGFBRII and BRAF mutation.38–46 Recently an MsPath score was proposed to predict MSI-H status in CRC patients with a possible hereditary predisposition using clinicopathological features such as age at diagnosis, anatomical site, histological subtype, tumour grade, Crohn’s-like reaction and TILs.47 A recent meta-analysis by Popat et al, including more than 7000 patients, found that tumours with MSI showed a significant improved overall survival time compared to MSS CRCs.48 This conclusion was however derived primarily from retrospective studies and needs to be confirmed prospectively. Though MSS CRCs appear to derive a survival benefit from adjuvant 5-FU therapy, evidence suggests that MSI tumours may be more resistant to this treatment.49–53
LOH18q and p53
Chromosomal loss at 18q has been reported in up to 70% of CRCs.54 The gene DCC, which maps to 18q21, is recognised as a key player in colorectal carcinogenesis and is the primary candidate for the biological effect of chromosome 18q allelic imbalance. Patients with locally advanced stage II or stage III disease appear to demonstrate a significantly poorer prognosis with loss of 18q.55–58
The TP53 tumour suppressor gene is mutated in approximately 50% of CRCs.59 Despite 20 years of investigation, the impact of TP53 mutation on clinical outcome is far from conclusive. The European Group of Tumour Markers (EGTM), as well as the American Society of Clinical Oncology (ASCO), currently recommend against the use of TP53 mutation analysis for screening, staging, surveillance or monitoring treatment of patients with CRC.60 61
Gene expression profiling
Gene profiling is expected to improve the identification of patients with more aggressive and treatment-resistant tumours. Using a cDNA micorarray containing more than 30 000 distinct gene transcripts, Eschrich et al identified 43 core genes capable of predicting 36-month overall survival with 90% accuracy using 78 patient samples, a result which was validated using an independent set of patients.7 In their analysis, molecular staging was more accurate at determining prognosis than Dukes staging, particularly for stage B and C patients. Microarray gene expression profiling has also successfully been applied to predict complete tumour response in rectal cancer patients undergoing preoperative chemoradiotherapy using test and validation groups and may represent a promising new direction in individualising treatment protocols.8 9 62
Tumour immunity
The prognostic impact of TILs and tumour-related immune responses is becoming increasingly recognised.63 Roponnen et al found an independent effect of TILs with improved overall and recurrence-free survival in addition to an inverse correlation between TILs and tumour stage.64 Baker et al recently demonstrated in more than 1000 CRCs that an increased number of intraepithelial TILs was strongly linked to early stages of tumour progression and to a significantly improved outcome in patients with MSS tumours.65 CD8+ TILs express cytotoxic mediators such as granzyme B and perforin and are thought to be responsible for the more favourable outcome in TIL-positive tumours.66 67 This association with prognosis does not however appear to be generalisable to MMR-deficient tumours, which themselves inherently exhibit an abundance of TILs, a finding which is consistent with the theory of tumour immuno-editing.68 The role of the adaptive immune response in CRCs was additionally explored by Galon et al by both genomic and immunostaining analysis of total lymphocytes (CD3), CD8 T-cell effectors, and memory T-cells (CD45RO) on a large cohort of patients.69 Their results underline once more the important prognostic value of the type, density and location (whether at the invasive margin or tumour centre) of immune cells and their effect on prognosis, independent of UICC-TNM classification.
PROGNOSTIC SIGNIFICANCE OF PROTEIN MARKERS
Immunohistochemistry is frequently employed as a routine diagnostic test and is relatively inexpensive. Nevertheless, immunohistochemical markers have yet to find routine application as prognostic or predictive factors in CRC in which TNM stage and other morphologically defined features continue to provide the clinical gold standard. Prognostic markers are classically defined as markers which can identify patients with differing risks of a specific outcome, such as tumour progression or death but are not used to guide the choice of a particular therapy.70 A predictive marker is one that predicts the differential efficacy or benefit of a particular therapy based on marker status and therefore could be used to guide the choice of therapy.70
Immunohistochemical markers currently being investigated for their prognostic impact include proteins involved in the wide array of signalling pathways mediating colorectal tumour progression and metastasis. The WNT signalling pathway involving β-catenin,71 72 adenomatous polyposis coli (APC),72 E-cadherin,72 73 the transforming growth factor-(TGF)-β pathway including TGFβ,65 a variety of SMAD proteins74 and the TGFβ receptors TGFβRI, TGFβ RII75 76 and the RAS-MAP kinase signalling pathway involving, among the novel potential markers, Raf-1 kinase inhibitor protein (RKIP)77–79 and the receptor for hyaluronic acid mediated motility (RHAMM)80 which are examples of potential targets for immunohistochemical prognostic studies. Markers of cell cycle arrest (p21, p27, p5381–83), apoptosis (Bcl-2,84 Bax,85 apoptosis protease activating factor (APAF)-186), proliferation (Ki6787) and DNA repair (thymidylate synthase, TS87) have also been explored for their prognostic value.
Vascular endothelial growth factor (VEGF) and epidermal growth factor receptor (EGFR) are among the most promising immunohistochemical prognostic indicators in CRC. VEGF is recognised as a potent pro-angiogenic factor whose downstream signalling events include endothelial cell proliferation, migration and vascular permeability.88 Up-regulation of VEGF has also been linked with urokinase plasminogen activator (uPA) and matrix metalloproteinases (MMPs), which function to degrade the basement membrane and extracellular matrix providing a scaffold for migrating endothelial cells resulting in newly formed vasculature composed of leaky, disorganised vessels and increased interstitial pressure. In 1971, Folkman hypothesised that blocking angiogenesis in tumours could be an effective method for treating cancer.89 In fact, the VEGF blockade has been shown to result in “normalisation” of the vasculature, decreased interstitial pressure, improvement of transport of chemotherapeutic agents to the target tumour and additionally potentiating the effect of radiotherapy.90 91 In CRC, VEGF expression detected by immunohistochemistry has been linked with tumour aggressiveness, poor disease-free and overall survival, distant metastatic spread and decreased response to preoperative radiotherapy.92–95 Bevacizumab (Avastin, Genentech/Roche), a humanised monoclonal antibody targeting VEGF, was approved by the United States Food and Drug Administration in February 2004 for the first-line treatment of metastatic CRC in combination with 5-fluorouracil-based chemotherapy.96 Other forms of anti-VEGF therapy are currently in various phases of clinical trial.88 97
EGFR is a tyrosine kinase receptor whose downstream signalling cascade includes the RAS-MAP kinase pathway.98 Over-expression of EGFR has been linked to poor prognosis in the majority of studies.99–102 Several anti-EGFR therapies have been approved for the treatment of metastatic CRC, including the antibodies cetuximab103 and panitumumab,104 and the tyrosine kinase inhibitor gefitinib.105 Cetuximab is a chimeric monoclonal antibody directed against the extracellular binding domain of EGFR, and used in combination with irinotecan for the treatment of EGFR-expressing metastatic colorectal cancer.103
Immunohistochemical scoring methods
Initial studies on promising prognostic markers are often followed up by subsequent reports directly contradicting these preliminary findings. A variety of sources of discrepancy have been recognised in prognostic studies including methodological differences, poor study design, lack of reproducibility, small sample sizes, and differences in the evaluation of immunoreactivity.10 The assessment of immunostaining is typically based on some measure of the number of positive tumour cells and often combined with a degree of staining intensity.99 100 106–111 The inter-observer variability of different scoring systems is rarely documented, and the selection of predetermined cut-off scores for a specific marker varies significantly from study to study. Table 1 provides an example of how discrepancies in the prognostic significance of a well established tumour marker, EGFR, can be affected by the choice of scoring method and the selection of predetermined cut-off values for “positive” expression.
Semi-quantitative scoring method: an alternative possibility
A possible alternative to these categorical scoring methods is the determination of immunoreactivity by semi-quantitative assessment of the proportion of positive tumour cells over the total number of tumour cells, ranging from 0% to 100%. The reproducibility of this scoring method has recently been demonstrated for a variety of different tumour markers including EGFR,102 VEGF,112 p53,112 β-catenin,113 Her2-neu,113 Bcl-2112 and APAF-1,86 112 in both tissue biopsies and tissue microarrays comprised of hundreds of tumour samples. The advantages of a semi-quantitative scoring method over standard methods of evaluation are numerous.
First, the assessment of staining intensity can be avoided. The degree of staining intensity has been shown to vary by tumour type, is partially influenced by the choice of fixatives and is inversely correlated with storage time of the unstained tissue sections.114 Moreover, the inter-observer agreement of staining intensity assessed by multiple observers is in many instances only moderate to poor.113 In addition, it has recently been demonstrated using a tissue microarray of more than 1000 CRCs that the evaluation of immunoreactivity using a semi-quantitative scoring method for several tumour markers appears to be sufficient for establishing associations of these markers with important clinicopathological features including T stage, N stage, tumour grade, vascular invasion and survival time.113
Second, with semi-quantitative scores, a wider array of statistical methods can be applied due to the more continuous nature of the data. Classification and regression tree (CART) methods are becoming increasingly more common because of the ease of interpretation of the results which are summarised in a simple-to-read decision tree.115 CART analysis has recently been used to identify prognostic sub-groups in CRC116 and, in conjunction with immunohistochemistry, to identify predictive markers of tumour response to preoperative radiotherapy.117
Most importantly, by quantifying protein expression, more relevant cut-off scores for tumour marker positivity can be established for the protein and clinical endpoint under evaluation. Recently an approach to the selection of cut-off scores for immunohistochemical biomarkers in CRC, namely by receiver operating characteristic (ROC) curve analysis, has been proposed and validated.11
ROC curve analysis: how positive is “positive”?
ROC curve analysis is a method commonly used in different areas of medicine to determine the sensitivity, specificity and accuracy of quantitative diagnostic tests.118 119 In CRC research, ROC curves have recently played a role in validating the MS-Path score for the identification of patients with Lynch syndrome,47 as well as in comparing novel serum markers for their ability to detect CRC or advanced adenomas.120 The goal of ROC curve analysis is at least twofold. In a first step, this method can be used to select cut-points above which a quantitative test result should be considered “positive”.121 In addition, by evaluating the area under the ROC curve (AUC), the discriminatory power of different quantitative tests can be compared in order to identify those with the greatest discriminatory ability for an outcome.121 These principles can both be applied to immunohistochemistry when used in conjunction with a semi-quantitative scoring system.
The ROC curve is a plot of the sensitivity and (1-specificity) for a binary outcome (yes/no) at each value of the immunohistochemical protein expression score (fig 2). For each percentage of positivity, a hypothetical threshold value is set and tumours are categorised as positive or negative around this cut-off point. The sensitivity and specificity for the outcome at these cut-off values are then evaluated and plotted, thereby generating a ROC curve. In order to determine the “best” cut-off scores for tumour marker “positivity”, the (0,1)-criterion can be used.121 With this method, the point on the ROC curve with the greatest sensitivity and specificity for the outcome is selected. This point can be identified as having the shortest distance from the curve to the coordinate (0,1), which theoretically has the optimal sensitivity and specificity for the outcome.
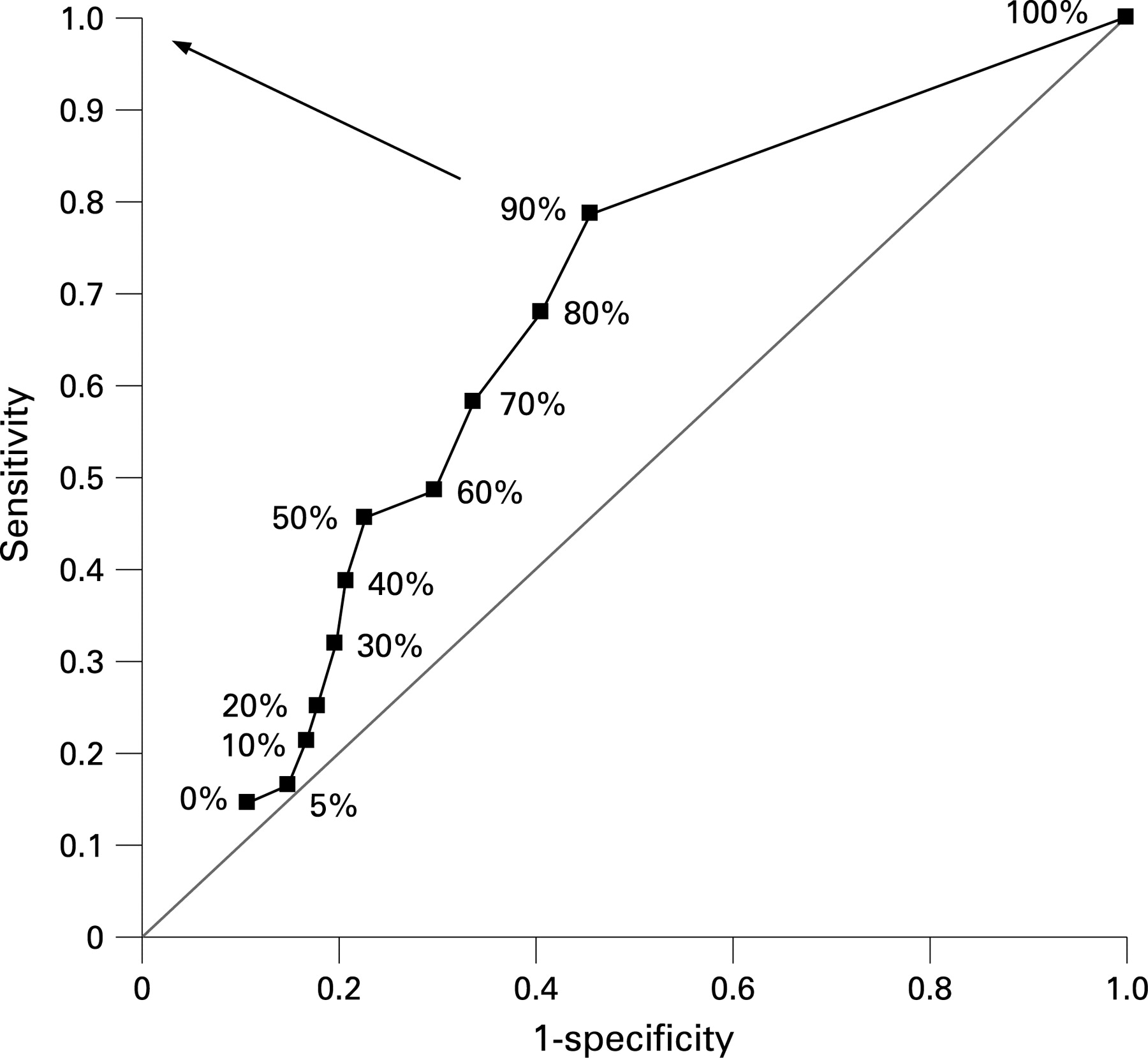
ROC curve analysis has several advantages over the use of predetermined cut-off scores for tumour marker positivity. First, the selection of cut-off scores using this approach should lead to a greater number of tissue samples correctly classified as having or not having a particular outcome, thereby increasing the probability of obtaining statistically significant and clinically meaningful associations. Secondly, a cut-off score can be selected such as to fulfil the specific interests of a particular endpoint. For example, it may be more appropriate to select a cut-off point leading to greater sensitivity over specificity when evaluating the association of a marker with response to treatment in order to capture all potentially responsive patients at an increased cost of over-treating. Third, the AUC can be very informative. The greater the AUC, the greater the discriminatory power of the marker for the outcome. By comparing the AUCs of numerous different tumour markers, it is possible to identify those most capable of discriminating between patients with and without some endpoint. ROC curve analysis may be helpful for identifying, from a larger panel of tumour markers, those with the greatest discriminatory power. Finally, it is a visual representation of the performance of one or many markers, and therefore simple to interpret. ROC curve analysis has been used to determine the cut-off scores for several novel and well-established tumour markers and their associations with a wide variety of clinical endpoints including survival,102 122 tumour budding30 and the presence of distant metastasis.79
ROC curve analysis in daily pathology
The implementation of semi-quantitative scoring into daily pathology would be a practical method to improve the value of immunohistochemistry findings, to further promote research on protein profiling and to reassess the reliability of potential prognostic immunohistochemical markers which have been more or less successful to date. The optimal cut-off scores for positivity for the same tumour marker may vary by clinical endpoint. The reporting of protein expression by the percentage of positive tumour cells would allow these scores to be used in future studies in conjunction with ROC curve analysis in order to develop standardised scoring methods for specific markers and clinical endpoints.
Tissue microarray analysis
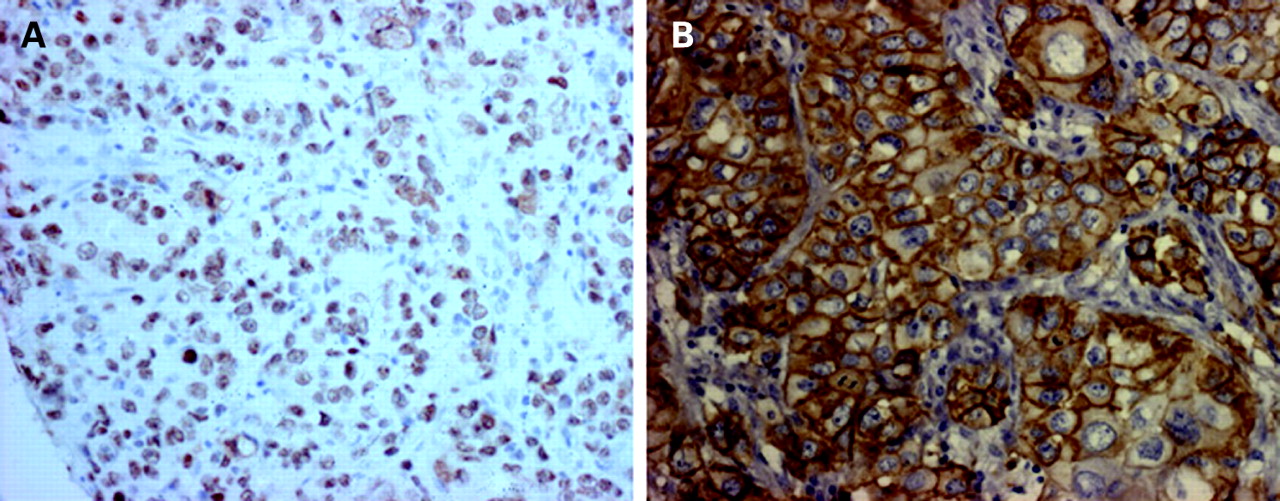
A possible, additional tool to standard histological assessment of tissues is the use of tissue microarray technology (fig 3). The tissue microarray is an unparalleled, cost-effective resource for studying the protein expression of tumour markers123 124 and allows the investigation of protein expression in hundreds of CRCs from patients at different stages of disease and with various lengths of follow-up. The use of tissue microarrays has several advantages over traditional methods of molecular pathology. First, immunostaining can be carried out under identical conditions for hundreds, if not thousands of tumour samples located on only a few histological slides. Second, due to the large number of tissue samples which can be analysed, it is possible to randomise tumour punches into sub-groups which can be used as test and validation sets for establishing the reliability of prognostic or predictive models. This was recently performed on a tissue microarray of more than 1000 MMR-proficient CRCs randomised into two groups on which were analysed tumour markers APAF-1 and E-cadherin and their ability to predict tumour budding.30 Third, evaluating a single tumour punch may lead to more reliable inter-observer agreement for both percent positivity and staining intensity, as precisely the same area of tumour is scored by each observer.113 Most importantly, tissue microarrays facilitate the evaluation of multiple tumour markers, and in conjunction with appropriate statistical techniques, can be a powerful resource for the development of multi-marker prognostic models in CRC.79 122
{kind=link}
{kind=link}
{kind=link}
Multi-marker phenotypes
Most, if not all proteins are subject to modulation by intricate molecular interactions and work within pathways to induce cellular effects. Rather than targeting investigations on a single marker, multi-marker phenotypes, which are defined here as various combinations of clinicopathological and/or tumour markers, can be more helpful in identifying sub-groups of patients with poor prognosis.125 This approach was recently used in conjunction with tissue microarrays and ROC curve analysis to identify independent prognostic markers in patients with node-negative CRC. From a panel of 13 potential markers, multi-marker phenotype combinations of TILs, p27 and uPA expression identified a high-risk group of node-negative T3 tumours.122 In a different study aimed at identifying patients at high-risk of distant metastasis, 10 clinicopathological features and 22 tumour markers were evaluated. Only N stage, the presence of vascular invasion and RKIP expression were valuable for discriminating between patients with and without metastasis independent of other known prognostic factors. Multi-marker phenotypes of these three features identified a sub-group of N0 tumours with similar clinical outcome to node-positive patients.79
These examples highlight the usefulness of investigating simultaneous multiple tumour markers as well as clinicopathological features. Moreover, it underlines the importance of performing multivariable analysis with well established prognostic factors to determine the independent effect of potential prognostic markers above and beyond the information which is routinely collected. With treatments in the preoperative setting, multivariable analyses may include the tumour marker as well as other pretreatment factors which may affect survival, such as clinical T and N stage. Several study groups have implemented a multi-marker phenotype approach to identifying prognostic and also predictive markers in CRC (table 2).
CONCLUSION
Despite promising findings with molecular and immunohistochemical analysis, tumour stage is still regarded as the most important prognostic factor in CRC.15 Tumour budding and tumour border configuration are additional morphological features which need be investigated more closely.126 Analysis of MSI has shown promise, not only as a prognostic, but also adverse predictive factor to adjuvant chemotherapy. Though there are currently no reliable immunohistochemical prognostic markers in CRC, the approach outlined in this review may increase the clinical value of immunohistochemistry findings. Steps include the scoring of immunoreactivity using a semi-quantitative evaluation method performed by multiple observers, followed by the selection of clinically relevant cut-off scores, appropriate statistical methods and assessment of multi-marker phenotype combinations.
Take-home messages
Tumour stage based on the UICC-TNM and American Joint Committee on Cancer (AJCC) classifications is still the most important prognostic factor in newly diagnosed colorectal cancer.
Tumour budding, defined as small clusters or single infiltrating carcinoma cells at the tumour border, is a promising additional morphological prognostic factor and may predict high-risk colorectal cancer cases.
According to the 2006 updated American Society of Clinical Oncology (ASCO) guidelines, none of the assessed prognostic/predictive factors are recommended for clinical use.
The combined approach of data-set randomisation, ROC curve analysis and multi-marker phenotypes could improve the quality of immunohistochemical protein marker investigations.
Acknowledgments
The authors would like to thank Professor Dr Luigi M Terracciano for helpful comments and editing of this manuscript, Dr Kristi Baker, McGill University, and Dr Parham Minoo, University of California for continued collaboration, and Professor Dr Jeremy R Jass for unwavering support.
REFERENCES
Footnotes
Competing interests: None.