Article Text

Abstract
New approaches to the prognostic assessment of breast cancer have come from molecular profiling studies. A major feature of this work has been to emphasise the importance of cancer cell proliferation as a key discriminative indicator of recurrence risk for oestrogen receptor positive breast cancer in particular. Mitotic count scoring, as a component of histopathological grade, has long formed part of a routine evaluation of breast cancer biology. However, there is an increasingly compelling case to include a specific proliferation score in breast cancer pathology reports based on expression of the cell cycle regulated protein Ki67. Immunohistochemical staining for Ki67 is a widely available and economical test with good tolerance of pre-analytical variations and staining conditions. However, there is currently no evidence based protocol established to derive a reliable and informative Ki67 score for routine clinical use. In this circumstance, pathologists must establish a standardised framework for scoring Ki67 and communicating results to a multidisciplinary team.
- Breast Cancer
- Breast Pathology
- KI 67
Statistics from Altmetric.com
Introduction
Histopathological grading of breast cancer has long formed the basis for pathologists to systematically evaluate and report differences in tumour biology. The impact of cancer cell proliferation on this assessment is captured by inclusion of a mitotic count score as one of the three components of grade.1 In recent years, a more detailed assessment of breast cancer biology has been encouraged by molecular profiling studies that have defined breast cancer subtypes as well as individual molecular features and pathways that correlate with survival and/or treatment response. Interestingly, cancer cell proliferation has again emerged as a key discriminative feature of malignant phenotype from this work.2 On a practical level, this has led to an increasing expectation that pathologists will include a specific assessment of proliferation in routine breast cancer pathology reports. A labelling index based on immunohistochemical (IHC) staining of the cell cycle antigen Ki67 is an accessible approach for doing this, and an abundant and increasing body of published evidence supports the use of Ki67 as a clinical indicator for breast cancer.3 However, now under pressure from a compelling case to routinely report Ki67, pathologists face many unanswered questions on the optimal approach to assessment and interpretation of Ki67 in a clinical context.
Breast cancer biology and prognostication in current practice
The key issue for early breast cancer prognostication is to distinguish cases with a sufficiently high risk of relapse to warrant adjuvant cytotoxic chemotherapy. Traditionally, clinicians have used an integrated assessment of the clinicopathological features of breast cancer to estimate this risk. For example, the Nottingham Prognostic Index, which was derived from a retrospective, multivariate regression analysis, separates patients into good, moderate and poor prognostic groups based on tumour size, grade and lymph node involvement.4 Similarly, the web-based programme Adjuvant! Online further includes oestrogen receptor (ER) status, age and co-morbidities to predict recurrence rates at 10 years and potential benefit from adjuvant chemotherapy.5
In current practice, there are a number of influences that impact on interpretation of traditional clinicopathological prognostic indicators. For example, the widespread use of screening mammography has caused a shift towards diagnosis of early stage disease that may reduce the discriminative value of time dependent prognostic features such as lymph node involvement.6 The other major influence is current emphasis on determining sensitivity to targeted therapeutic options by documenting individual biomarkers, specifically the progesterone receptors (ER, PR) and amplification or overexpression of the HER2 oncogene.7 The overall effect of these changes is an increased role for tumour biology in clinical evaluation, and a formal evaluation of cellular proliferation can contribute to this.
Proliferation is a key discriminative feature of ER+ breast cancer
In practice, the question of whether adjuvant cytotoxic chemotherapy is warranted relates principally to ER/PR positive breast cancer and the risk of recurrence following optimal adjuvant endocrine therapy.8 In this regard, the definition of ‘intrinsic’ breast cancer subtypes based on gene expression profiling studies has been useful. In particular, these studies defined two predominantly ER positive ‘luminal’ breast cancer types: designated luminal A and luminal B.9 ,10 Luminal A breast cancers have been characterised as low grade, highly ER expressing tumour types that are typified by tubular and low grade ductal breast cancers.11 Luminal A breast cancer has an excellent survival profile and it has been argued that the addition of cytotoxic chemotherapy to adjuvant endocrine therapy for these tumours may not be warranted.12 ,13 In contrast, luminal B breast cancers have a higher risk of recurrence and adjuvant cytotoxic chemotherapy may be indicated.12
There are a number of molecular features that tend to be different between luminal A and luminal B breast cancers but the most obvious distinguishing feature is a higher proliferation rate in the latter.14 This distinction is consistent with another ‘molecular’ approach to prognostication which is to focus on ER+ breast cancer with a continuous gene expression based score that can define categories of increased recurrence risk. This approach is exemplified by the commercially available 21-gene recurrence score that is weighted to reflect increasing risk associated with increasing proliferation, and incorporates an assessment of Ki67 gene expression.15
Molecular prognostic indicators for breast cancer are increasingly applied clinically and there are commercial gene expression based assays available to assess both intrinsic breast cancer subtype, and gene prognostic scores.15 ,16 However, it has also been demonstrated that similar information can be derived from more routine pathological assessment, especially if a Ki67 score is included. For example, a study by Cheang et al17 that specifically compared a gene expression based intrinsic subtype classification of breast cancers with pathological features, reported that a Ki67 score ≥14% distinguished luminal B from luminal A, ER-positive HER2-negative tumours. This approach was subsequently supported by the St Gallen 2011 Expert Panel as an alternative to molecular subtyping.12 Similarly Cuzick et al18 demonstrated that an algorithm based on semi-quantitative scores for ER and PR expression, HER2 status and Ki67 score derived from immunohistochemical staining (‘IHC-4’ score) showed similar prognostic performance to the 21-gene recurrence score for ER+ breast cancer.
Together such studies illustrate a key role for Ki67 score in current approaches to prognostic assessment of ER+ breast cancer. Moreover, the value of Ki67 as an individual biomarker for breast cancer prognostication has been reported in a large number of studies and in several meta-analyses.19–22 However, methods used to evaluate Ki67 are highly variable across published studies, making results difficult to compare.3 Furthermore, there is no clear evidence available to guide implementation or interpretation of Ki67 scores in routine practice.
Measuring Ki67: gene expression versus IHC
‘Ki67’ is the common term for a protein that was originally identified as the nuclear antigen of a mouse monoclonal antibody designated Ki67. The gene encoding the Ki67 protein (MKI67), on chromosome 10q26, comprises 15 exons with a large exon 13 including 16 homologous sequences that contain a highly conserved 22 amino acid element called the ‘Ki67 motif’.23 Nine of the Ki67 motif regions include a highly immunogenic five amino acid sequence that forms the epitope for a number of Ki67 monoclonal antibodies including the commonly used monoclonal antibodies MIB1 and SP6.24 ,25 The precise function of Ki67 is uncertain, however the combination of its tight cell-cycle phase regulation and a short half-life have established the protein as a robust marker of proliferating cells.3 Ki67 protein is absent in quiescent cells (G0) and universally expressed in proliferating cells. There is varied expression of Ki67 throughout the cell cycle with low expression during G1 and early S phase and progressive increase in expression with maximal expression during mitosis (M phase).3
The two approaches for measuring Ki67 expression in clinical breast cancer samples are: (i) a semi-quantitative analysis of the Ki67 (MKI67) mRNA content in RNA extracted from frozen or formalin-fixed paraffin embedded (FFPE) tissue; and (ii) a score based on the percentage of breast cancer cells that stain positively for Ki67 by IHC. Limited data are available that directly compare RNA and IHC based Ki67 measurement in the same breast cancers. One of the challenges in doing this is the marked area-to-area heterogeneity in cellular proliferation and hence Ki67 expression that can led to substantial differences in proliferation scores between individual samples of the same tumour specimen. However, acknowledging this limitation Yamamoto et al26 recently reported a weak but statistically significant correlation in 203 breast cancer samples between Ki67 relative gene expression values derived from real-time quantitative reverse-transcription PCR (RT-qPCR) analysis of both frozen and FFPE samples, and an IHC labelling index. Tan et al27 also reported an association between Ki67 gene expression levels derived from microarray analysis of 21 frozen breast cancer samples, and IHC in cases with a high Ki67 score (>10%). More indirect support for an informative Ki67 result derived from either an IHC or an RNA based method comes from a study by Sahebjam et al28 that reported a strong linear correlation in 53 breast cancers between a Ki67 IHC labelling index and the RNA based 21-gene recurrence score.
IHC staining for Ki67 has a number of obvious advantages compared with RNA based methods. These include the important fact that pathologists can directly ensure that only cancer cells contribute to the Ki67 score by IHC and exclude contaminant inflammatory and stromal cells (figure 1). In addition, the method is relatively inexpensive, accessible in a routine diagnostic laboratory and the Ki67 result can be included as part of the diagnostic pathology report. Commonly used antibodies for Ki67 staining are the mouse monoclonal antibody MIB1 and rabbit monoclonal antibody SP6. In a direct comparison reported by Zabaglo et al,25 performance of these two antibodies was similar, although there was less background and non-specific staining for SP6.
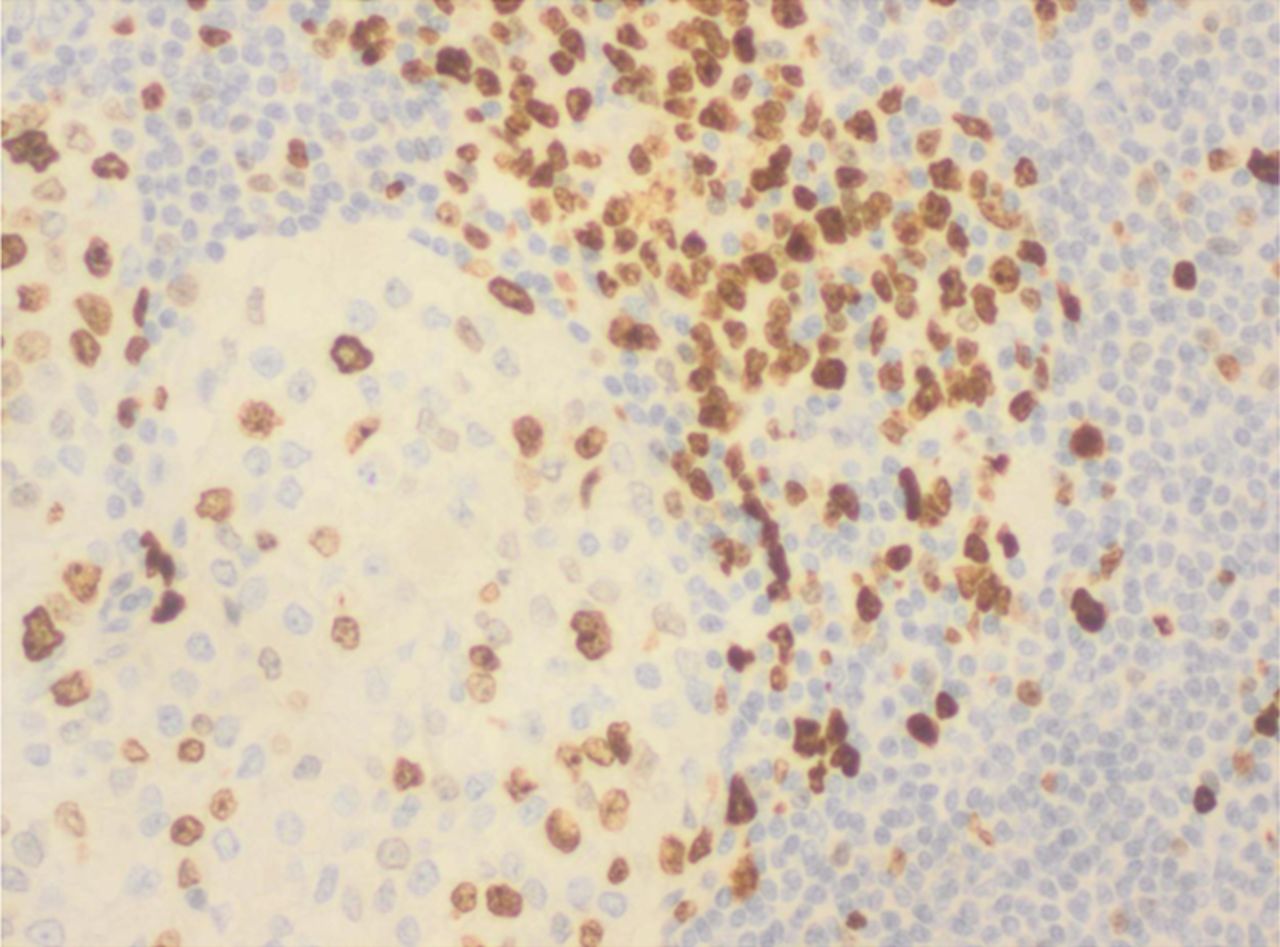
Staining of contaminant lymphoid cells (×200, clone SP6 1 : 200), upper right side of figure, tumour cells on lower left; these cells should be excluded during counting.
Determination of a Ki67 IHC labelling index
IHC staining of fixed tissue sections is a technique which is subject to a large number of variables, and similar to HER2 and ER/PR, Ki67 staining requires optimisation and standardisation of conditions. An advantage of Ki67 IHC is that it is much more tolerant of preanalytical variables that commonly affect HER2 and ER/PR testing. In particular fixation, which is frequently a problem in other breast cancer assays and may even affect mitotic count,29 is less problematic for Ki67,with the mean number of positive nuclei largely unaffected by variable fixation, although staining appearance and intensity may vary.30 ,31 Guidelines for Ki67 IHC proposed by Dowsett et al31 suggest that fixation conditions currently recommended for receptor testing are adequate and unless there is an extreme (overnight) delay in fixation, freezing of the sample or fixatives other than neutral buffered formalin, staining with Ki67 is quite robust.
The IHC Ki67 score or labelling index generally refers to the percentage of cancer cells that stain positively. In assessing staining of individual cells, it is important to acknowledge that variation in Ki67 expression occurs throughout the cell cycle, ranging from weakly staining foci within the nuclei and perinucleolar granules in G1 phase, to nucleolar and perinucleolar staining in G2 and intense staining when the nuclear membrane disrupts during mitosis, and rapid fading of this intensity in anaphase and telophase.20 Consequently, breast cancer cells counted positive for Ki67 should include all types of nuclear staining, whether granular or diffuse, and regardless of staining intensity. Mitotic figures serve as a good positive internal control for Ki67 IHC (figure 2). High Ki67 expression may be seen in tumours with a marked lymphoid infiltrate and in this circumstance caution is needed to distinguish tumour and lymphoid cells when scoring Ki67. Dual IHC staining for keratin and Ki67 may be helpful to positively identify cancer cells if there is an obscuring lymphoid infiltrate.
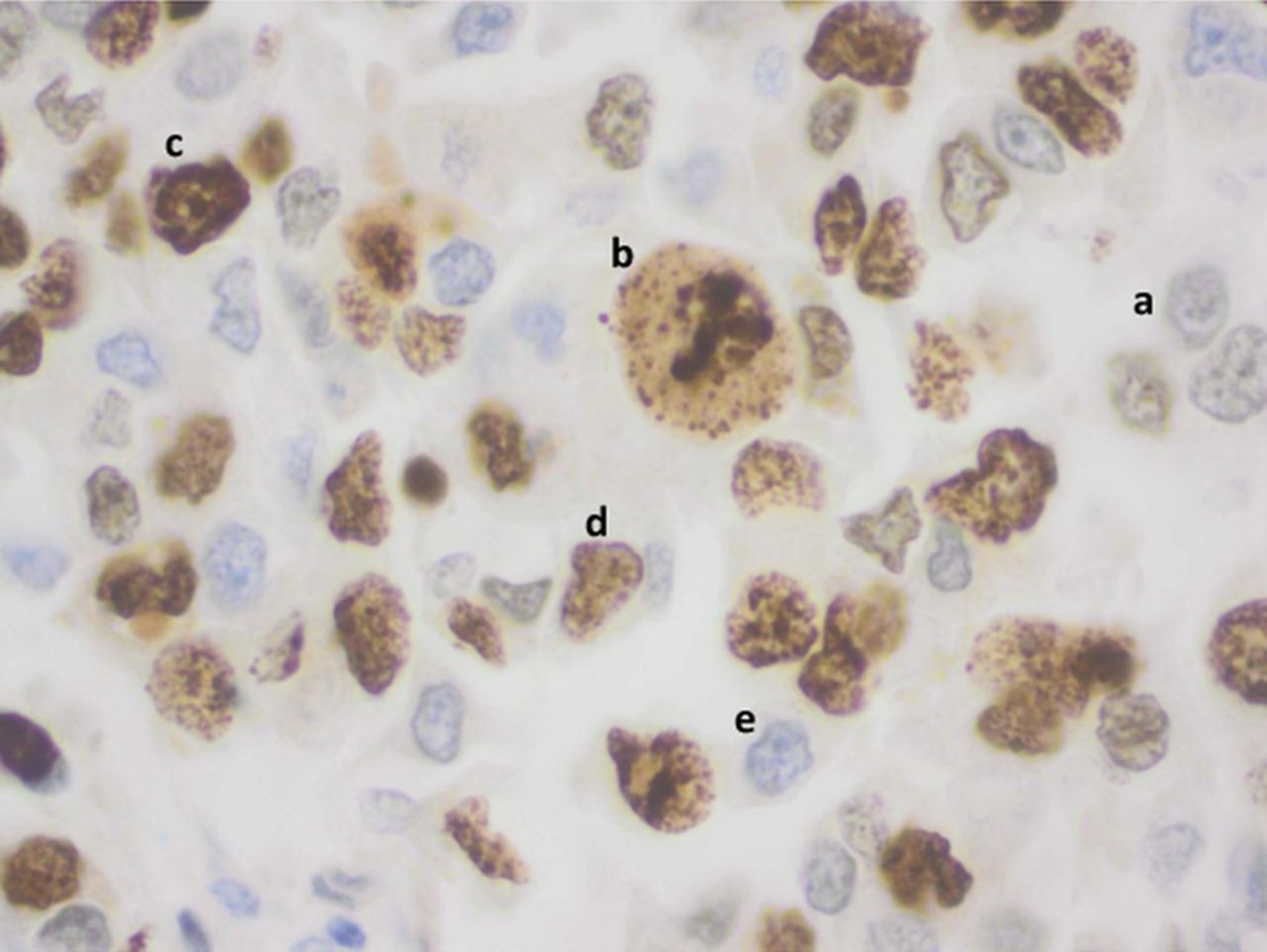
Variations in nuclear staining (×400, clone SP6 1 : 200); (a) weak positive granular nuclear staining, (b) positive staining in a tripolar mitosis serves as a positive internal control, (c) strong diffuse positive nuclear staining, (d) moderate positive granular nuclear staining, (e) no nuclear staining.
A number of approaches for quantifying the proportion of Ki67 positive cells in tissue sections have been reported. These include image analysis methods which have the advantage of speed and objectivity, but may underestimate unstained cell numbers and may also be more affected by background staining as well as heavy lymphoid or stromal infiltration.25 ,32 Visual scoring methods may simply comprise an estimate of the proportion of cells stained. A more robust approach is to perform a formal cell count of stained and unstained cancer cells and Dowsett et al31 have advocated that ideally 1000 cells, and a minimum of 500 should be counted. Cell counting may be aided by an eyepiece graticule, or a method that we have used is to examine a digital image of the stained section and count using software with a manual tag function.33–35
Arguably the greatest challenge to reliable Ki67 scoring is the selection of fields for counting because of the variation caused by intra-tumoural heterogeneity (figure 3). One approach is to select fields in staining ‘hot-spots’ which is analogous to the approach taken in Scarff–Bloom–Richardson grading where the tumour periphery is scanned for the most mitotically active area to assess the mitotic score.1 This approach is conceptually appealing since it maximises the impact of highly proliferative areas of a cancer on prognostic evaluation. An alternative approach aims to derive a representative score by selecting fields with a range of staining patterns across the section.31 In the absence of definitive advice on this issue, a standardised approach should be applied for reporting within an individual laboratory to ensure consistency in case-to-case comparisons.

{kind=link}
{kind=link}
{kind=link}
Heterogeneous staining within an invasive ductal carcinoma(×100, clone SP6 1 : 200), more positive cells on top right of figure and predominantly negative cells in bottom left of figure.
Ki67 cut-off determination
Clearly the range of a Ki67 score is from 0% to 100%, and while this full range can be integrated into a prognostic algorithm as demonstrated by the IHC4 score,18 more commonly a cut-point is used to specify categories of risk. An example is in the breast cancer subtyping study described by Cheang et al17 that used a 14% cut-off to distinguish luminal A and luminal B tumours. This approach has been recommended for clinical use,12 however it is important to note that the Cheang et al study involved examination of tissue microarray rather than whole tissue sections and the method for Ki67 counting was not clearly described. It is therefore unclear whether the very specific 14% cut-off that was reported in the Cheang et al17 study would apply in routine practice.
A large number of different cut-points have been described to specify low and high Ki67 scores in published studies with a range from 3.5% to 34% reported in a recent review.22 A cut-point of 10% has been quite commonly used and in a recent study using whole section, ‘hot-spot’ Ki67 scoring, Aleskandarany et al36 reported that a 10% cut-off for Ki67 could stratify grade 1 and grade 2 breast cancers into statistically significant prognostic groups. In addition the study found Ki67 index was the strongest predictor of overall and metastasis free survival in both univariate and multivariate analysis in grade 2 tumours.36 In order to account for the biologic heterogeneity of breast cancer, the prognostic significance of Ki67 was assessed within breast cancer subtypes in the same cohort. This demonstrated that Ki67 labelling index cut-points set at 10% and 50% could identify subgroups of ER positive (luminal) breast cancer with distinct outcome. However, the majority of HER2 positive and triple negative tumours showed high proliferative activity which limited the ability of the Ki67 labelling index to stratify these tumour types into distinct prognostic groups.37
Summary and future directions
The potential value of Ki67 as a prognostic biomarker for breast cancer emerges strongly from published studies, notwithstanding variations in study design and methodology. Of particular interest is its use in combination with other routinely measured biomarkers to classify breast cancers into subgroups analogous to those identified in gene-expression profiling, that have potential implications for therapy. There is also accruing evidence to support a role for Ki67 as a predictive marker in both the adjuvant and neoadjuvant settings.38 ,39
Thus the advantages of Ki67 assessment in breast cancer are numerous and increasingly widely accepted. Less certain is the methodology that should be employed to report a reproducible and clinically informative Ki67 result. In terms of scoring, it seems clear that individual cell counting is preferable to visual estimates, and guidelines suggest that ideally 1000 tumour cells should be counted, with an absolute minimum of 500 cells. Analogous to mitotic index assessment, the advancing edge of the tumour, probably in the areas of highest Ki67 expression is likely to be representative of tumour clones that will drive the biologic potential of the tumour.
In view of the varied methodologies employed in Ki67 assessment and the lack of consensus regarding quantitation, it may be prudent to establish an institutional Ki67 reporting protocol and then review local data to understand the range of scores seen across grades and under the specific conditions. Discussion and circulation of this information to other members of the breast cancer multidisciplinary team will assist in communication and provide greater understanding of the significance of a result in the context of individual institutions and the patient profiles.
Ki67 is emerging as a valuable addition to the histopathological assessment of breast cancers that provides important prognostic information that is likely to assist with prognostic evaluation and refinement in treatment and follow-up protocols. Strong arguments can be made for addition of this marker to the routine assessment of breast cancer. The challenge with this assay lies in standardising methodology to ensure that Ki67 results are reproducible and clinically relevant. Continuing research aimed at establishing an evidence based approach for routine reporting of Ki67 is a priority in this area.
Take-home messages
-
The proliferation marker Ki67 is emerging as an influential prognostic biomarker for breast cancer.
-
There are currently no evidenced based protocols to guide clinical reporting of Ki67 in routine practice. In this circumstance, individual centres should establish a standardised approach that will provide internally consistent results.
-
Further studies are needed to optimise reporting of Ki67 in breast cancer research and practice.
References
Footnotes
-
Funding RLB received funding support from the Cancer Institute New South Wales via the Sydney West Translational Cancer Research Centre.
-
Contributors Conception and design, or analysis and interpretation of data (NP, RLB); drafting the article or revising it critically for important intellectual content (NP, RLB); and final approval of the version to be published (NP, RLB).
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.