Article Text

Abstract
Background: Akt is a serine/threonine kinase that plays an important role in tumorigenesis and influences prognosis in several cancers. However, its importance in oral squamous cell carcinomas (OSCC) has not been elucidated.
Aim: To investigate the association between the expression of activated Akt, clinicopathological factors, and E-cadherin, PCNA (proliferating cell nuclear antigen), and VEGF (vascular endothelial growth factor) expression to verify the validity of Akt as a prognostic factor in OSCC.
Methods: Phosphorylated Akt (p-Akt), E-cadherin, PCNA, and VEGF expression were assessed immunohistochemically in 84 OSCCs. The results were analysed in relation to clinicopathological factors.
Results: p-Akt was expressed in 29 cases. It was significantly correlated with lymph node metastasis, TNM stage, and E-cadherin expression. Univariate analysis showed that p-Akt expression, E-cadherin expression, PCNA expression, differentiation, tumour size, lymph node metastasis, TNM stage, and recurrence correlated with prognosis. Multivariate analysis showed that p-Akt expression is an independent prognostic factor in patients with OSCC.
Conclusions: This study revealed that Akt activation is a significant prognostic indicator for OSCC and is correlated with E-cadherin expression. The inhibition of Akt is a possible molecular approach to the treatment of OSCC.
- LI, labelling index
- OSCC, oral squamous cell carcinoma
- PBS, phosphate buffered saline
- p-Akt, phosphorylated Akt
- PCNA, proliferating cell nuclear antigen
- VEGF, vascular endothelial growth factor
- oral squamous cell carcinoma
- Akt
- E-cadherin
- prognostic factor
Statistics from Altmetric.com
- LI, labelling index
- OSCC, oral squamous cell carcinoma
- PBS, phosphate buffered saline
- p-Akt, phosphorylated Akt
- PCNA, proliferating cell nuclear antigen
- VEGF, vascular endothelial growth factor
Oral cancer is the sixth most common cancer worldwide. The most common type of oral cancer is squamous cell carcinoma, which accounts for almost nine out of 10 oral malignancies.1 The prognostic evaluation and decisions on treatment strategy are mainly based on the TNM stage.2 Despite progress in treatment modalities over the past few decades, oral cancer still has a poor survival rate, with a high incidence of metastasis.3,4 Oncogenes, tumour suppressor genes,5–7 cell proliferation markers,8 angiogenesis,9 and cell adhesion molecules10,11 have been studied as potential tools to predict the prognosis of an individual with oral squamous cell carcinoma (OSCC).
“Despite progress in treatment modalities over the past few decades, oral cancer still has a poor survival rate, with a high incidence of metastasis”
The oncogenic serine/threonine kinase Akt1 (also known as PKB) is a downstream effector of phosphatidylinositol 3-kinase and is frequently activated in human cancer.12 The gene for the closely related Akt2 is amplified and overexpressed in ovarian, pancreatic, breast, and follicular thyroid carcinomas.13–17 In addition, total Akt kinase activity is increased in non-small cell lung cancer, squamous cell carcinomas of the oral cavity, breast carcinoma, and prostate carcinoma.18–20 Akt activation contributes to tumorigenesis.
The main biological consequences of Akt activation that are relevant to cancer cell growth can be classified loosely into three categories: survival, proliferation (increased cell number), and growth (increased cell size).21
Akt activation is also associated with enhanced tumour cell invasion. Akt enhances invasiveness of pancreatic carcinoma cells via upregulation of insulin-like growth factor I,22 and it increases the secretion of matrix metalloproteinases 2 and 9 in immortalised mammary epithelial cells and ovarian carcinomas.23,24 Activation of the Akt pathway in cancer cells leads to epithelial–mesenchymal transition and invasion in vivo. Akt induced epithelial–mesenchymal transition involves downregulation of E-cadherin, which appears to result from upregulation of the transcription repressor SNAIL.25
Akt has additional effects on tumour induced angiogenesis that are mediated, in part, through hypoxia inducible factor 1α and vascular endothelial growth factor (VEGF).21
There are few reports that have examined the relation between activated Akt expression, clinicopathological factors, and Akt related gene expression in OSCC.
The purpose of our study was to clarify the relation between activated Akt expression, clinicopathological factors, and the expression of E-cadherin, proliferating cell nuclear antigen (PCNA), and VEGF. Accordingly, the potential value of Akt as a prognostic indicator of survival was assessed.
MATERIALS AND METHODS
Patients and tumour samples
Eighty four patients (62 men and 22 women) with OSCC were examined by immunohistochemistry. All tumours were surgically removed at the department of oral and maxillofacial surgery, Seoul National University Dental Hospital, South Korea, between 1992 and 2001. The age of the patients ranged from 27 to 93 years, with a mean of 59.0 years. Clinical data obtained from patient charts included age, sex, smoking habits, alcohol consumption, TNM stage, and recurrence. Tumours were staged according to the current TNM classification as recommended by the AJCC.26 Tumours were re-reviewed by two pathologists to determine the histological grade (well differentiated, moderately differentiated, or poorly differentiated). Survival was calculated from the date of diagnosis until the date of death or last follow up (table 1).
Summary of the clinicopathological features and p-Akt, E-cadherin, VEGF, and PCNA expression
Immunohistochemistry
Immunohistochemical staining was performed using the streptavidin–biotin–peroxidase complex method. Sections (4 μm thick) were cut from each paraffin wax block, dewaxed, and incubated for 15 minutes in a methanol solution containing 3% H2O2 to block endogenous peroxidase activity. For phosphorylated Akt (p-Akt), E-cadherin, and VEGF staining, the slides were placed in 0.01M citrate buffer (pH 6.0) and heated in a 500 W microwave oven for two five minute periods. After washing with phosphate buffered saline (PBS), sections were incubated in 10% normal rabbit serum for 30 minutes to reduce non-specific antibody binding. The primary antibodies used were: monoclonal rabbit antihuman p-Akt (Ser 473; Cell Signaling Technology, Beverley, Massachusetts, USA) at a dilution of 1/50; monoclonal mouse antihuman VEGF (clone G153-694; Pharmingen, San Diego, California, USA) at a dilution of 1/400; monoclonal mouse antihuman E-cadherin (G-10; Santa Cruz Biotechnology, Santa Cruz, California, USA) at a dilution of 1/200; and monoclonal mouse antihuman PCNA (P-10; Dako, Glostrup, Denmark) at a dilution of 1/100. All sections were incubated for one hour at room temperature, except for the Akt sections, which were incubated overnight at 4°C. After being washed with PBS, sections were incubated with biotinylated goat antirabbit IgG for 30 minutes. They were then washed three times with PBS, treated with streptavidin–peroxidase reagent for 30 minutes, and re-washed with PBS three times. The reactions were visualised with diaminobenzidine (Dako) as chromogen and sections were counterstained with Mayer’s haematoxylin. Normal mouse and rabbit IgG were substituted for each primary antibody as negative controls.
Evaluation of immunohistochemical results
The cutoff points were based on the distribution of staining results or the results of other studies in the literature, because clear biological criteria are not available. For p-Akt the cutoff point was 0–20% v > 20%.27 For E-cadherin, expression was defined as positive when at least 50% of the cells showed membrane staining.28 For VEGF, the cutoff point was 20%.29 For PCNA, nuclei from over 1000 tumour cells were counted in the five to eight random fields chosen for each sample and the count was expressed as the percentage of PCNA positive cells (PCNA labelling index; LI).
The slides were assessed by consensus between two investigators who had no prior knowledge of the corresponding clinicopathological data.
Statistical analysis
Relations between p-Akt, E-cadherin, and VEGF and the various clinicopathological factors were examined using the χ2 test. The mean value and SD of PCNA LIs were calculated and compared with clinicopathological factors using the Student’s t test.
Survival curves were calculated using the Kaplan–Meier method and analysed using the log rank test. The expression of PCNA was classified as high at ⩾ 60% and low at < 60% for the Kaplan–Meier method. Deaths caused by OSCC were considered as outcomes and all deaths from other causes were censored. The roles of each identified prognostic factor (by univariate analysis) and combined effects (by multivariate analysis) were explored using the Cox proportional hazards survival analysis model. In the univariate analysis, the hazards ratio and its 95% confidence interval were calculated for each variable. Forward and backward stepwise procedures were used to identify the combination of factors that was important in the prediction of prognosis. All statistical analyses were considered significant when the p value was less than 0.05. Statistical analyses were performed using SPSS version 11.5.
RESULTS
Correlation between p-Akt, E-cadherin, PCNA, and VEGF expression and clinicopathological factors
Table 2 shows the association of several clinicopathological factors with p-Akt, E-cadherin, PCNA, and VEGF expression. P-Akt expression was positive in 29 cases (fig 1A). p-Akt staining significantly correlated with lymph node metastasis and clinical stage (p < 0.05). Patients with a smoking habit, poor differentiation, large tumour size, and recurrence tended to show higher p-Akt expression, but the result was not significant.
Correlation between p-Akt, E-cadherin, PCNA, and VEGF expression and clinicopathological features

Immunohistochemical staining in oral squamous cell carcinoma. (A) Positive expression of phosphorylated Akt (original magnification, ×200); (B) positive expression of E-cadherin (original magnification, ×200); (C) high expression of PCNA (original magnification, ×100); (D) positive expression of VEGF (original magnification, ×200).
E-cadherin was expressed in 40 cases and correlated with lymph node metastasis (p < 0.05). The mean PCNA LI was 57.0 and VEGF was expressed in 57 cases. There was no significant correlation between PCNA and VEGF expression and clinicopathological factors.
Correlation between p-Akt expression and the expression of E-cadherin, VEGF, and PCNA
Table 3 shows that p-AKT expression was significantly higher in cases with high expression of E-cadherin than in those with low expression (p = 0.001). Cases with high VEGF or PCNA expression had higher p-Akt expression, but this was not significant (p = 0.143 and p = 0.091, respectively).
Correlation between expression of p-Akt and E-cadherin, PCNA, and VEGF expression
Survival analysis
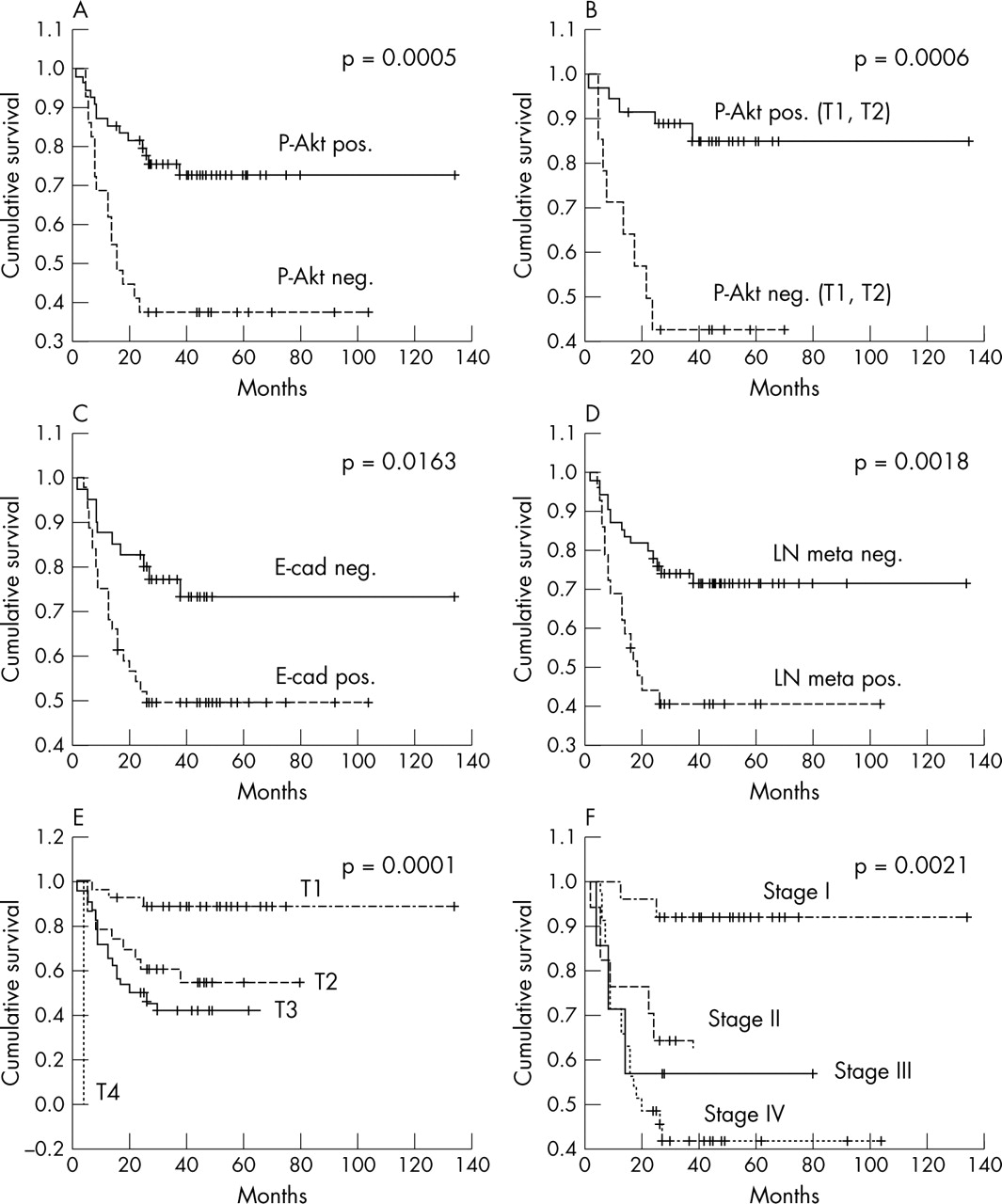
Univariate Cox proportional hazards survival analysis of 84 OSCCs showed that the following factors indicated a worse prognosis (table 4): poor differentiation (p = 0.039), large tumour size (p = 0.003), high clinical stage (p = 0.0002), positive lymph node metastasis (p = 0.003), recurrent disease (p = 0.007), high p-Akt expression (p = 0.001), low E-cadherin expression (p = 0.021), and high PCNA LI (p = 0.049). Figure 2A–F shows the survival curves calculated by the Kaplan–Meier method and analysed using the log rank test. They show that the survival of patients with high p-Akt expression was significantly worse than that of those with low p-Akt expression (p = 0.0005). Survival was also associated significantly with p-Akt expression in T1 and T2 tumours (p = 0.0006). Multivariate Cox proportional hazards survival analysis revealed that pAkt expression and clinical stage were independent prognostic factors (table 5).
Univariate analysis of survival in 84 patients with OSCC according to the Cox proportional hazards model
Multivariate analysis of survival of 84 patients with OSCC according to the Cox proportional hazards model

{kind=link}
{kind=link}
Survival curves of patients with oral squamous cell carcinoma according to (A) phosphorylated Akt (p-Akt) expression, (B) p-Akt expression in T1 and T2 tumours, (C) E-cadherin expression, (D) lymph node (LN) metastasis, (E) tumour size, and (F) clinical stage (Kaplan–Meier method).
DISCUSSION
To establish appropriate therapeutic modalities for OSCC, an accurate assessment of the factors affecting tumour progression and patient prognosis is crucial. Although the conventional TNM staging system is useful for OSCC classification, the outcome is poor for patients even in the low stage (I and II) groups. Therefore, several molecular markers used for OSCC classification have been investigated, but none showed great value in predicting patient prognosis.
Akt is a central player in the signal transduction pathways activated in response to growth factors or insulin, and is thought to contribute to several cellular functions including cell growth, proliferation, apoptosis, invasion, and angiogenesis. Recently, several important publications have described novel mechanisms of regulating Akt. Alteration of Akt expression and activity is associated with several human cancers including glioblastoma, and ovarian, breast, pancreatic, and lung cancers.21
“Phosphorylated Akt expression correlated with lymph node metastasis, the clinical stage of which remains a significant prognostic variable in oral squamous cell carcinoma”
In our study, we used immunohistochemistry to analyse p-Akt and Akt related biological factors known to be involved in tumour progression, such as E-cadherin (associated with cancer invasion), VEGF (tumour angiogenesis), and PCNA (marker of tumour proliferative activity).
The reported incidence of p-Akt expression varied from 26% in prostate cancer27 to 66% in both melanomas30 and head and neck squamous cell carcinomas.31 We found p-Akt expression in 34.5% of OSCCs. However, our threshold for positive expression was 20%, higher than the 10% used in Gupta’s study.31 If Gupta et al had used our 20% threshold, they would have found p-Akt expression in 23.7% of their cases, which is similar to our result.
p-Akt expression correlated with lymph node metastasis, the clinical stage of which remains a significant prognostic variable in OSCC. Gupta et al reported that p-Akt staining was not associated with T stage, N stage, or differentiation of disease. However, the number of cases in their study (38) was too small to carry out meaningful multivariate analysis. In pancreatic cancers, Schlieman et al showed that p-Akt expression correlated with higher histological tumour grade.32 Because reports on the relations between p-Akt expression and clinicopathological factors are rare, an additional larger scale study would be needed to elucidate this association.
Take home messages
-
Activated Akt serine/threonine kinase (p-Akt) is a significant prognostic indicator for oral squamous cell carcinoma (OSCC)
-
p-Akt is inversely associated with E-cadherin expression in OSCC
-
The inhibition of Akt is a possible molecular approach to the treatment of OSCC
E-cadherin expression is closely related to lymph node metastasis. Several reports have shown that E-cadherin expression is significantly correlated with lymph node metastasis in OSCC.33,34
There was no significant correlation between VEGF and PCNA expression and the clinicopathological factors.
Our study suggests a significant inverse correlation between p-Akt and E-cadherin expression in OSCC. This is the first study to demonstrate such an association. Akt activation represses E-cadherin gene transcription by upregulation of the transcription repressors SNAIL and SIP1.25
In our study, univariate and multivariate survival analysis showed that p-Akt and clinical stage were independent prognostic factors in OSCC. The multiple activities of Akt, such as enhancement of proliferation, growth, antiapoptosis, invasiveness, and angiogenesis, endow OSCC with microinvasiveness at the resected margin and promote the invasion and recurrence of cancer. Thus, high p-Akt expression in a patient with OSCC would warrant a more radical mode of treatment.
In conclusion, our study revealed that Akt activation is a significant prognostic indicator for OSCC and may provide a new method of treatment of OSCC. The inhibition of Akt is a possible molecular approach to the treatment of OSCC.
Acknowledgments
This study was supported by the international collaboration research grant 01-2003-000-00192-0 from the Korea Science and Engineering Foundation (KOSEF).