


Abstract
Background: Prognosis of patients with metastatic pancreatic cancer is dismal. Recently, two first-line combination chemotherapy regimens have shown a survival benefit over single-agent gemcitabine. Patients and Methods: A 57-year old metastatic pancreatic cancer patient from our department (Eastern Cooperative Oncology Group performance status (ECOG PS): 0, baseline carbohydrate antigen (CA) 19-9 level: 2,900 U/ml) received 12 cycles of first-line chemotherapy with nab-paclitaxel and gemcitabine until disease progression within the pivotal Metastatic Pancreatic Adenocarcinoma Clinical Trial (MPACT). Results: Treatment with nab-paclitaxel and gemcitabine resulted in a partial response by Response Evaluation Criteria in Solid Tumors (RECIST), a rapid biochemical CA 19-9 response, a progression-free survival of 13 months and an overall survival of 20 months. Leukopenia grade 3 prompted dose reduction by two dose levels. Non-hematological toxicities included alopecia, skin rash, nail changes and peripheral neuropathy (all grade 2 or less). Conclusion: First-line combination chemotherapy with nab-paclitaxel and gemcitabine is an effective and manageable treatment option for patients with metastatic pancreatic cancer with the potential for long-term disease control.
Treatment of patients with metastatic pancreatic ductal adenocarcinoma (PDAC) used to be a tedious endeavor with no really effective systemic treatment option available. Since 1996 gemcitabine had become the mainstay of treatment for patients with advanced PDAC. Approval was granted due to a significant improvement in a clinical benefit response with a composite end-point defined as improvement in pain, performance status or stabilization of weight. In the respective registration trial the median overall survival (OS) with gemcitabine was 5.7 months compared to 4.4 months achieved with the standard arm therapy 5-fluorouracil (5-FU). At 12 months, 18% of patients treated with gemcitabine were still alive. The median time to progressive disease with gemcitabine was 9 weeks, compared to 4 weeks with 5-FU. In patients with measurable disease 5.4% of those treated with gemcitabine had a partial radiological tumor response (1).
In the following 15 years no clinically meaningful progress was made. Median survival times ranged around 6 months. Numerous gemcitabine-based doublet regimens did not result in a meaningful improvement of the clinical benefit and in particular not in a survival benefit (2, 3). The addition of erlotinib to gemcitabine achieved a statistically significant, yet clinically moderate increase in median OS from 5.91 months to 6.24 months, one-year survival from 17% to 23% and median progression-free survival (PFS) from 3.55 months to 3.75 months (4).
Recently, the data from two large phase III trials made a difference for the treatment of patients with metastatic PDAC by demonstrating significant improvements in clinical outcomes for two combination therapies over single-agent gemcitabine (5, 6).
The cytotoxic combination regimen of oxaliplatin, 5-FU, leucovorin and irinotecan (FOLFIRINOX) significantly improved median OS to 11.1 months compared to 6.8 months for gemcitabine (hazard ratio (HR)=0.57; 95% confidence interval (CI)=0.45-0.73, p<0.001). Survival rates at 12 months and at 18 months were 48.4% vs. 20.6% and 18.6% vs. 6%, respectively. Median PFS was 6.4 months vs. 3.3 months with gemcitabine (HR=0.47; 95% CI=0.37-0.59, p<0.001), overall response rate (ORR) 31.6% compared to 9.4% with gemcitabine (5). The intensive treatment with FOLFIRINOX resulted in significantly more adverse events of >grade 3 in terms of neutropenia (45.7% for FOLFIRINOX vs. 21.0% for gemcitabine), febrile neutropenia (5.4% vs. 1.2%), thrombocytopenia (9.1% vs. 3.6%), diarrhea (12.7% vs. 1.8%) peripheral neuropathy (9.0% vs. 0%), while the incidence of elevation of alanin aminotransferase was decreased (7.3% vs. 20.8%) (5).
In January 2014 the combination of nab-paclitaxel and gemcitabine was approved in the European Union for the first-line treatment of patients with metastatic pancreatic adenocarcinoma (7). In the pivotal phase III Metastatic Pancreatic Adenocarcinoma Clinical Trial (MPACT), 861 patients with metastatic PDAC received first-line chemotherapy either with nab-paclitaxel at 125 mg/m2 in combination with gemcitabine at 1,000 mg/m2, both administered on days 1, 8, 15, 29, 36 and 43 of a 56-day cycle with subsequent cycles on days 1, 8, 15 of a 28-day cycle or with gemcitabine monotherapy at 1,000 mg/m2 weekly for 7 out of 8 weeks in the first cycle and in subsequent cycles on days 1, 8, 15 of a 28-day cycle. The median OS was significantly increased to 8.7 months as compared to 6.6 months with gemcitabine alone (HR=0.72; 95% CI=0.620-0.825, p<0.0001). Survival rates at 12, 18, 24 and 36 months were 35%, 16%, 10%, 4% for the combination vs. 22%, 9%, 5%, 0% for gemcitabine alone (6, 8). The median PFS was significantly increased to 5.5 months vs. 3.7 months with gemcitabine alone (HR=0.69; 95% CI=0.58-0.82, p<0.001); the ORR was 23% vs. 7% (p<0.001), respectively. The most frequently observed adverse events of ≥grade 3 were neutropenia (38% for nab-paclitaxel plus gemcitabine vs. 27% for gemcitabine alone), leukopenia (31% vs. 16%), fatigue (17% vs. 7%) and neuropathy (17% vs. 1%) (2).
These efficacy data are encouraging and provide new treatment options for patients and physicians for the treatment of metastatic PDAC. The clinical benefit can be even more impressive in individual patients. Combination chemotherapy may result in improved PFS and OS times as demonstrated by the case reported here.
Case Report
In January 2012 a 57-year-old patient consulted his general practitioner because of postprandial flatulence, indigestion and lack of appetite. He had no relevant comorbidity or medical history other than 40 pack-year of smoking. The patient presented in an excellent performance status (Eastern Cooperative Oncology Group (ECOG)=0).
Abdominal ultrasound showed a lesion of 5 cm in diameter in the pancreatic corpus. Computed tomography (CT)-guided biopsy detected a poorly-differentiated adenocarcinoma of the pancreas. Consecutive CT imaging further revealed mesenteric lymph node and liver metastases. In addition, an asymptomatic embolism of a right segmentary pulmonary artery was diagnosed, which prompted therapeutic anti-coagulation with low molecular weight heparin after implantation of a central venous port system.
Two weeks later the patient was randomized into the experimental arm of the registrational MPACT trial. He received first-line combination chemotherapy: nab-paclitaxel was administered at a dose of 125 mg/m2 and gemcitabine at a dose of 1,000 mg/m2, both administered on days 1, 8, 15, 29, 36 and 43 of a 56-day cycle with subsequent cycles on days 1, 8, 15 of a 28-day cycle.
Overall, the patient was given 12 cycles of combination chemotherapy. In cycle 2 he developed grade 3 leukopenia, which prompted a protocol-prespecified dose reduction by one level of nab-paclitaxel to 100 mg/m2 and gemcitabine to 800 mg/m2. In addition, granulocyte colony-stimulating factor (G-CSF) was administered intermittently. Subsequently, grade 3 leukopenia re-occurred and necessitated a second dose reduction by one further level in cycle 6: chemotherapy was thus continued at a dose of 75 mg/m2 for nab-paclitaxel and at a dose of 600 mg/m2 for gemcitabine. Additional hematological toxicities under chemotherapy were grade 2 anemia and grade 1 thrombocytopenia. Non-hematological toxicities were all grade 2 and comprised alopecia, skin rash, nail changes and peripheral neuropathy.
CT imaging showed a long-lasting response: while the size of the primary tumor did not change significantly, the two remaining target lesions (both mesenteric lymph node metastases) showed a complete regression. In addition, the liver metastasis (which was no target lesion per Response Evaluation Criteria in Solid Tumors (RECIST) due to its size of <1 cm in diameter) disappeared. The sum of target lesion at baseline was 102 mm, while after 11 months the sum of target lesions was decreased to 29 mm (resulting in a partial response by RECIST). In parallel, a long-lasting biochemical response as measured by the level of the serum tumor marker carbohydrate antigen (CA) 19-9 was observed (Figure 1). Overall, the PFS under combination therapy with nab-paclitaxel plus gemcitabine, as assessed by RECIST, was 13 months.
By the end of February 2013 the disease progressed as indicated by an increase of the size of the primary tumor in a follow-up CT scan. This prompted the onset of second-line chemotherapy with FOLFIRI in March 2013. However, in mid-May 2013 second-line therapy had to be stopped because of a further imaging-confirmed progression of the primary tumor and the re-occurrence of new liver metastases. Third-line chemotherapy with mFOLFOX-6 was started in July 2013. However, the patient's performance status deteriorated rapidly after only 1 cycle. He developed peritoneal carcinomatosis and consecutive intestinal obstruction. The patient subsequently was referred to our specialized out-patient palliative care team and died at home at the end of September 2013.
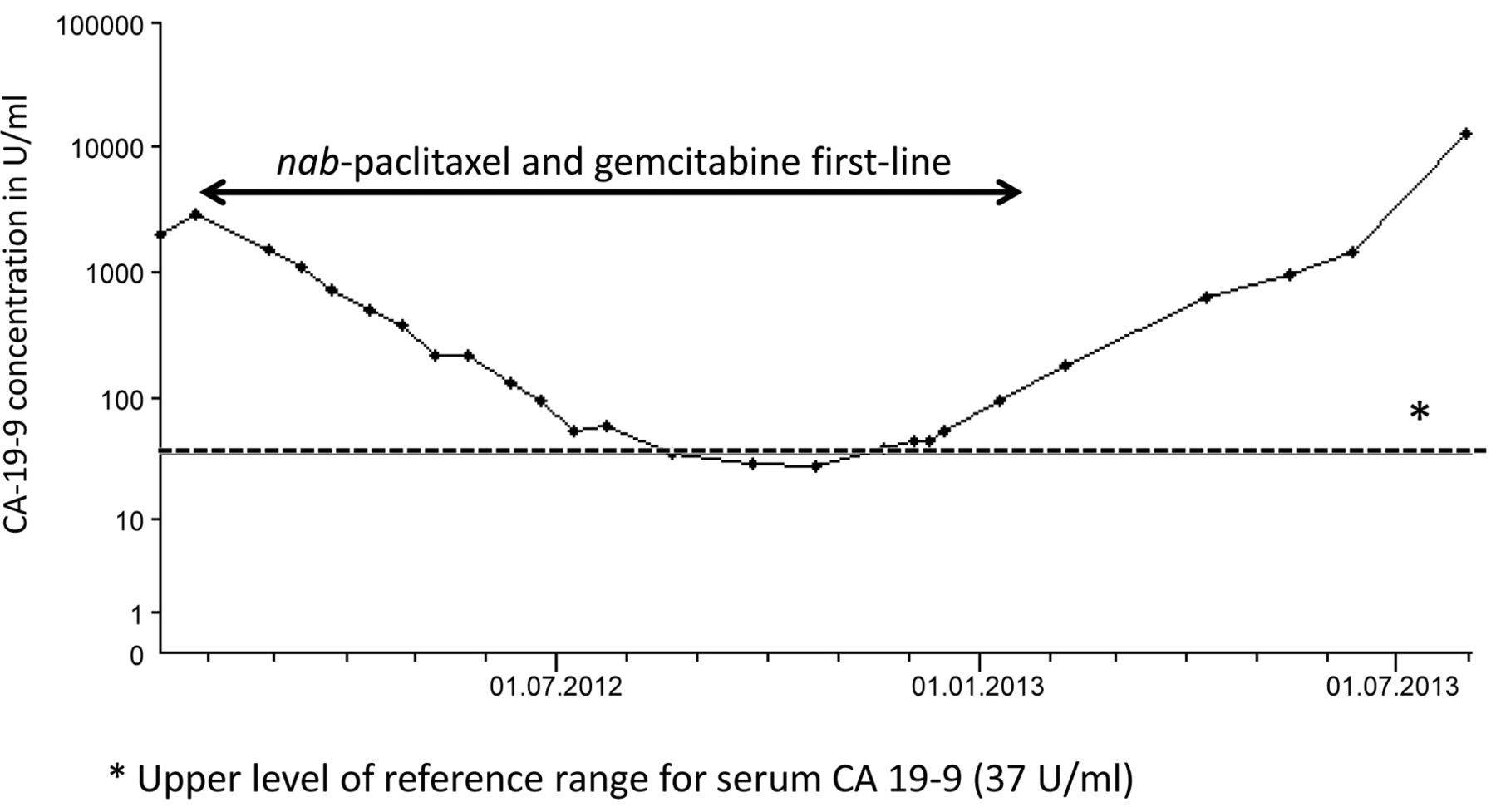
Course of serum CA19-9.
Discussion
Our case illustrates how the situation of patients with metastatic PDAC has actually changed due to the available new treatment options.
The median PFS achieved with single-agent gemcitabine was 9 weeks in the pivotal trial published by Burris and co-workers with the caveat that 70% of patients had a Karnofsky performance status of 50-70% (1). In the standard arms of the trials, that included patients with a more favorable performance status, gemcitabine monotherapy achieved a median PFS of 3.8 months, 3.3 months and 3.7 months (4-6). This compares to a median PFS of 5.5 months with the combination of nab-paclitaxel-plus-gemcitabine in the experimental arm of the MPACT trial. Our patient was progression-free for even 13 months after the start of first-line chemotherapy with nab-paclitaxel and gemcitabine. The median OS achieved with gemcitabine monotherapy was 5.7 months in the pivotal trial (1) and 5.9, 6.8 and 6.6 months in the standard arms of the trials in patients with a more favorable performance status (4-6). This compares to a median OS of 8.7 months with the combination of nab-paclitaxel and gemcitabine in the MPACT trial (6, 8). Two-year survival was actually 10% with this combination (6, 8). Our patient lived for 20 months after the start of first-line chemotherapy with nab-paclitaxel and gemcitabine.
The patient reported here had an elevated serum level of CA 19-9 of 2,900 U/ml at baseline, which dropped by 83% to 500 U/ml after 2 treatment cycles. CA 19-9 is currently regarded as the most widely used serum tumor marker for pancreatic cancer. It is known as a prognostic marker separating PDAC patients with different mortality risks. Those with an elevated level at baseline usually have a poorer prognosis (9, 10). In the MPACT trial baseline CA 19-9 was also significantly associated with median OS in the overall population (8). However, while patients treated with gemcitabine alone had a better OS with a baseline CA 19-9 level below the median level of 2,470 U/ml, treatment with nab-paclitaxel and gemcitabine was equally effective in terms of OS in patients with high and low CA 19-9 levels. In patients with a CA 19-9 level at baseline >59 times higher than the normal range had the greatest reduction in the risk of death with nab-palitaxel and gemcitabine over patients treated with gemcitabine (6).
CA 19-9 has further been identified as a potential predictive marker. Data show a positive correlation between biochemical response (e.g. a decrease in the level of CA 19-9 under chemotherapy) and OS (9). In the nab-paclitaxel registration MPACT trial more patients had a decrease in CA 19-9 when treated with the combination of nab-paclitaxel and gemcitabine as compared to those treated with gemcitabine alone (6). Patients that had a biochemical response in terms of a decrease of CA 19-9 in serum had an improved median PFS and OS compared to those without a fall in CA 19-9. Biomarker results also showed that CA 19-9 was an early surrogate marker of the activity of chemotherapy in PDAC: in patients with a decrease of CA 19-9 of ≥20% the median PFS with nab-paclitaxel and gemcitabine was 7.7 months and the median OS was 13.2 months, while in patients with a CA 19-9 decrease of ≥90% the corresponding survivals were 8.5 months and 13.4 months, respectively (11).
The duration of treatment in our patient was 12 months, while the median duration in the MPACT trial population was 3.9 months. It should be noted that long-term stabilization of the patient's PDAC was achieved, although we had to reduce the dose of nab-paclitaxel and gemcitabine twice and continued therapy at the protocol pre-specified dose level “-2” (see above) from cycle 6 onwards.
In conclusion, first-line combination chemotherapy with nab-paclitaxel and gemcitabine can result in long-term disease control and a substantial prolongation of OS irrespective of a high baseline CA 19-9. An early biochemical response in terms of a CA 19-9 decrease 8 weeks after treatment initiation may be predictive for the activity of the combination of nab-paclitaxel and gemcitabine. It can be regarded as a guidance to continue chemotherapy with this regimen even if treatment has to be continued at a reduced dose due to the management of side effects. Thus, this single case illustrates that modern combination chemotherapy may offer patients with metastatic PDAC a new perspective with the prospect of long-term survival.
Footnotes
-
This article is freely accessible online.
-
Disclosure
The Authors received editorial support in the preparation of this manuscript from Dr. Susanne Hell, funded by Celgene Corporation. The Authors were fully responsible for all content and editorial decisions for this manuscript.
- Received June 20, 2014.
- Revision received July 28, 2014.
- Accepted July 30, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}