


Abstract
Background: In 1972, Beck introduced an inventory (BDI) for rapid screening of depression. The associations between the BDI and the risk of breast cancer (BC) are rarely considered together in prospective studies. Patients and Methods: In an extension of the Kuopio Breast Cancer Study, 115 women with breast cancer symptoms were semi-structurally interviewed in-depth as well as asked to complete standardised questionnaires (Forsen, Spielberger, MADRS), and all study variables were obtained before any diagnostic procedures were carried out. BDI was used to evaluate the depression of the study participants. Results: The clinical examinations and biopsies showed BC in 34 patients, benign breast disease (BBD) in 53 patients, and 28 individuals were shown to be healthy (HSS). There was a trend for the women with HSS to have less sadness (BDI mean score, 0.27) than those of the BC (BDI mean score, 0.56) and BBD groups (BDI mean score, 0.49). The HSS group tended to be less pessimistic (BDI mean score, 0.15) than the patients in the BC group (BDI mean score, 0.44) and in the BBD group (BDI mean score, 0.42). The HSS group also had less self-accusation (BDI mean score, 0.19) than the patients in the BC group (BDI mean score, 0.50) and the patients in the BBD group (BDI mean score, 0.62). The HSS group also reported less work inhibition and weight loss than the patients in the BC group and in the BBD group. The mean sum of the scores of BDI variables was significantly lower in the HSS group (BDI mean score, 7.1) than in the BC (BDI mean score, 8.4) or BBD groups (BDI mean score, 8.8). Conclusion: The results of this study do not support a specific link between BDI and breast cancer risk. However, the patients with BC and BBD tended to have an increased risk for depressive symptoms.
Breast cancer survivors most frequently report genetic factors, family history of cancer, environmental pollutants, food additives, psychosocial stress, hormone replacements and contraceptives as causing their type of cancer (1). Respondents underestimate the importance of life-style factors that are known to be associated with increased risk of breast cancer, while overestimating the importance of stress and environmental pollution factors (2). Because breast cancer is a hormonally responsive neoplasm and one with great psychological impact, it has been the most extensively investigated tumour for possible psychological variables associated with risk and survival. Hormonal factors, such as early age at menarche, later age at menopause, later age at first full-term pregnancy and hormone replacement therapy, are known to be the main risk factors for sporadic breast cancer (BC) (3). In addition, life-style factors, such as obesity, smoking, alcohol consumption and lack of physical activity, appear to contribute to the increased risk for this malignancy, although the results concerning such factors are inconsistent (3-9). Psychological factors, such as stressful and adverse life events, are widely thought to play a role in the aetiology of BC (10-25). In 1972 Aaron Beck introduced an inventory (BDI) for rapid screening of depression even in family practice (26). To the Authors' knowledge, the associations between the BDI and the risk of breast cancer are rarely considered together, and therefore this was a prospective study to examine the role of BDI in women with breast symptoms referred by physicians to the Kuopio University Hospital (Finland).
Patients and Methods
The Kuopio Breast Cancer Study is a multidisciplinary cooperative project conducted by different departments of the University of Kuopio and Kuopio University Hospital. The participants of the project included all women who were referred to Kuopio University Hospital (North-Savo Health Care District) for breast examination between April 1990 and December 1995. The Kuopio Breast Cancer Study follows the protocol of the International Collaborative Study of Breast and Colorectal Cancer coordinated by the European Institute of Oncology in Milan, and was initiated as a SEARCH program of the International Agency for Research on Cancer (IARC). The collaborative study is based on the assumption that breast cancer and colorectal cancer may have common risk factors. Study centres for the study are situated in Canada, Finland, Greece, Ireland, Italy, Russia, Slovakia, Spain and Switzerland (27). The participants of the Kuopio Breast Cancer Study consisted of individuals showing breast cancer symptoms (a lump in the breast or in the axilla, pain in the breast, bleeding from the nipple, nipple discharge and skin dimpling), or an abnormality of the breast and the indications for referral in this study are in line with previous results in a Breast Cancer Diagnostic Unit in Finland (28).
Characteristics of the study participants.
This case-control study is an extension of Kuopio Breast Cancer Study (29, 30). The study was approved by the Joint Committee of the University of Kuopio and Kuopio University Hospital. Participation was based on written consent. Women with breast symptoms or a suspect breast lump had been referred by physicians to the Kuopio University Hospital (Finland) during the study period from January 1991 to June 1992. Women were asked to participate in the study and were interviewed by a psychiatrist (P.O.) before any diagnostic procedures (to determine the level of emotional depression), such that neither the interviewer nor the patient knew the diagnosis at the time of the interview. The interviews were recorded, and the ratings were completed before the final diagnosis. The clinical examination, mammography and biopsy showed BC in 34 (29.6%) patients, benign breast disease (BBD) in 53 (46.1%) patients and 28 (23.4) patients with healthy breasts (HSS) (Table I).
Assessment of life events and stress. The research method was a semi-structured in-depth interview (16). At the beginning of the interview, the patients drew their ‘life lines’ and a line describing being a woman, which supported the interview. In ‘the draw a line of your life’ the patient was asked to draw positive life experiences (‘good times’) with lines pointing upwards and negative life experiences (‘hard times’) with lines pointing downwards. Adverse and stressful life events were evaluated over the whole lifespan, with particular reference to the previous ten years before admission. The adverse or stressful life events and the context surrounding them were marked on the ‘life line paper’ during the interview. After the interviews the life events were rated (by P.O.) according to the degree of threat or stress they were likely to pose, and each adverse or stressful life event was graded on a 5-point scale, grade I (one point) indicating non-threatening event and grade V (five points) a severely threatening event. The defences used were also assessed on a five-point scale: grade I (one point) indicating very defensive, in denial and grade V (five points) non-defensive. The ‘Working through and actively confronting the stressful event’ variable was also rated on a five-point scale: grade I (one point) indicating not resolved and grade V (five points) fully resolved. These measurements were put together in the final statement, one to two points on the scale means little or mild loss or stress, and five means very hard loss or stress.
The rated case record included the loss events from childhood (under three years of age and 4-12 years of age), adolescence (13-23 years of age), adulthood and especially the last ten years prior to the investigation.
Coping and defence strategies. A modified Haan coping and defence inventory (31) was used. This inventory is divided into ten scales, and each scale has subscales from grade 0 to grade III: with 0 meaning no definition, I: coping, II: defending and III: fragmentation.
Beck depression inventory (BDI). The women completed the BDI (26, 32, 33) with 21 variables. The investigator used the modified inventory divided into three grades: grade I (score 0-13), no depression; grade II (score 14-24), moderate depression; grade III (score over 24), severe depression.
Forsen inventory (FI). The women completed the Forsen Inventory (24, 25) with 11 variables. The investigator used the FI inventory divided into three grades: grade 0, no psychiatric symptoms; grade 1, moderate psychiatric symptoms; grade 2, severe psychiatric symptoms.
The BDI scores in healthy study participants (HSS), patients with benign breast disease (BBD) and in patients with breast cancer (BC).
Spielberger trait inventory. All study participants completed the Spielberger trait inventory (34). Trait anxiety was assessed using the subscale from the inventory, and the ten items refer to how a person generally feels, with a higher total score reflecting a higher anxiety trait (20-80 range).
Montgomery Åsberg depression rating scale (MADRS). The MADRS with ten variables (scores from zero to six) was used to evaluate the depression of the study participants (35), and the test was rated as follows: grade I (scores 0-6), no depression; grade II (score 7-19), mild depression; grade III (score 20-34), moderate depression; and grade IV (score 35-60), severe depression.
Statistical analysis. Significance of the results was calculated with the SPSS/PC statistical package (SPSS Inc., Chigaco, IL, USA). Correlations and differences between the study groups were measured with the two-sided Chi-square test and non-parametric Kruskal-Wallis variance analyses. Results were considered statistically significant at a p-value <0.05.
Results
The mean age of the BC patients was 51.5 years. The corresponding figure for the patients with BBD was 47.5 years and for the HSS group 45.7 years. Although the patients in the BC group were older than those in the BBD or HSS groups, the age difference was not statistically significant (p=0.12). The majority of the patients (85/115, 74%) were married or living in a steady relationship. Almost half of the patients (41.7%) had graduated from primary school, and 25% had a college education. By profession, the patients represented industrial and service employees (25.2%), office employees (10.4%), health care employees (8.7%), and farmers (8.7%), and almost 23.5% were retired. The combined mean gross income of both spouses in the patients with BC was 36,100 € per year. The corresponding figures for the patients with BBD were 27,714 € per year. The patients with BC were significantly (p=0.03) wealthier than the patients with BBD and HSS, as estimated by the combined gross income of the both spouses. The groups differed only slightly from each other as to the factors of the reproductive life of the women (Table I).
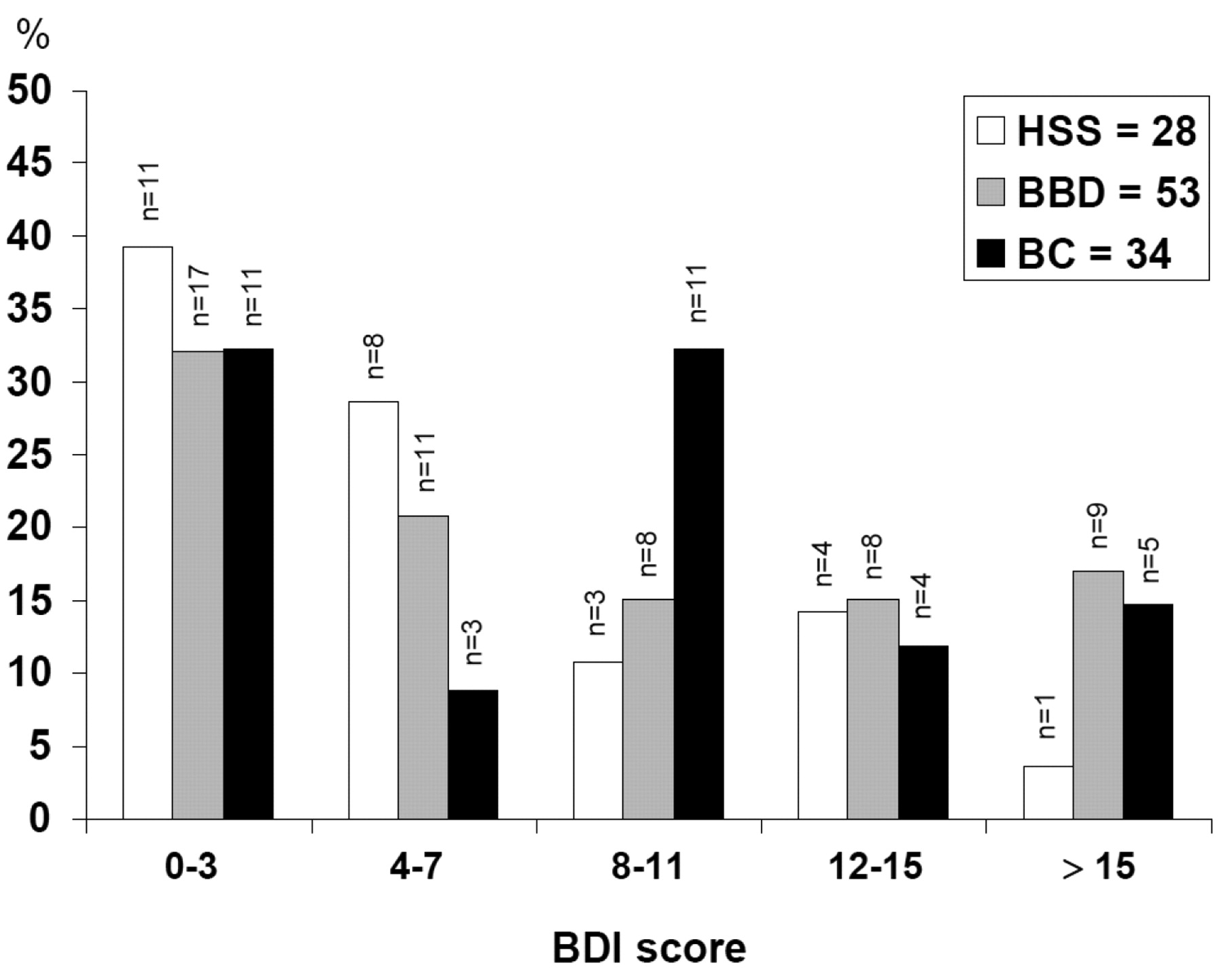
The psychiatric symptoms in Beck Depression Inventory. The psychiatric symptoms in BDI in HSS, in patients with BBD and in patients with BC are shown in Table II. There was a trend for the women with HSS to have less sadness (BDI mean score, 0.27) than these of the BC (BDI mean score, 0.56) and BBD groups (BDI mean score, 0.49). The HSS group tended to be less pessimimistic (BDI mean score, 0.15) than the patients in the BC group (BDI mean score, 0.44) and in the BBD group (BDI mean score, 0.42). The HSS group also had less self-accusation (BDI mean score, 0.19) than the patients in the BC group (BDI mean score, 0.50) and the patients in the BBD group (BDI mean score, 0.62). There was a trend for the women with HSS to have less work inhibition (BDI mean score, 0.22) than these of the BC (BDI mean score, 0.41) and BBD groups (BDI mean score, 0.40). The HSS group also reported less weight loss (BDI mean score, 0.07) than the patients in the BC group (BDI mean score, 0.29) and the patients in the BBD group (BDI mean score, 0.19). The mean sum of the scores of BDI variables were significantly lower in the HSS group (BDI mean score, 7.1) than in the BC (BDI mean score, 8.4) or BBD groups (BDI mean score, 8.8). However, the distribution of the mean sum of the BDI scores for HSS, BBD and BC groups differed only slightly when the variables were shown in five separate categories (Figure 1).

The distribution of the mean sum of the BDI scores for HSS, BBD and BC groups are shown in five separate categories.
Discussion
In 1972 Aaron Beck introduced an inventory (BDI) for rapid screening of depression even in family practice (26). The BDI was used in this study to evaluate the subjects history of psychiatric symptoms. The patients in the BC, BBD and HSS groups differed only slightly from each other, when the BDI variables were considered separately. However, there was a trend for the women with HSS to have less sadness, pessimism and self-accusation than these of the BC and BBD groups. The HSS group also reported less weight loss and work inhibition than the patients in the BC group and the patients in the BBD group. The mean sum of the scores of BDI variables was significantly higher in the BC or BBD groups than in the HSS group. However, this study does not provide a support for the hypothesis of a relationship between the BDI and BC risk.
It may be commented that the study subjects in the BBD group have an increased risk for breast cancer. The BBD category in this study was a heterogeneous group of breast diseases with different histological entities (benign fibrocystic disease, n=37; fibroadenoma, n=5; adenoma, n=3; papillomatosis, n=2; other benign breast disease, n=6). Patients with non-proliferative lesions (benign fibrocystic disease, n=37) have no or only slightly increased risk for breast cancer. Women whose breast biopsies show epithelial hyperplasia have about 2- to 4-fold increased risk of developing breast cancer.
Cancer survivors of all ages substantially underestimate the importance of obesity and physical inactivity. In contrast, survivors were much more likely to believe that fully unproven factors such as environmental pollutants, food additives, and occupation type cause their cancer (1, 2, 36). Many cancer survivors also believe that stress is a significant cause of cancer, even though there is no scientific consensus that stress causes cancer (37). The IARC has estimated that excessive body weight and physical inactivity account for about 20 to 25% of all cancers of the breast and colorectum (38) and that low intakes of fruits and vegetables may account for up to 12% of colorectal cancer (39).
From the popular belief that psychological factors have a significant role in the carcinogenesis of the breast, it follows that study subjects with breast tumour may be more prone than healthy subjects to report prior stress and other psychological problems in an effort to explain their breast disease. This may lead either to a false-positive association between psychological factors and breast cancer risk or to an overestimation of true-positive associations. Therefore, this study was designed to reduce the recall bias; the reports on psychological factors were obtained from the study subjects who had breast cancer symptoms but had not yet been given a definitive diagnosis. After the breast biopsy and the confirmation of diagnosis in histology, the study subjects were divided into those diagnosed with breast cancer (BC group), those with no breast disease (HSS group) or those with breast disease (BBD group). The patients were encountered in an extremely stressful situation before the definitive diagnosis and it can be assumed that on the basis of clinical impressions, some patients had already been given more or less clear hints by their doctors on their expected diagnosis.
One potential bias arises from age being a confounding factor, and some of the earlier studies have been criticised on such methodological grounds as limited controlling for age (40). In the current study, the BC group was 4.0 years and 5.9 years older than the BBD group and the HSS group, respectively. However, no statistically significant age difference between these groups was found in the current study (p=0.12).
The participants of the current study consisted of individuals showing BC symptoms (a lump in the breast or in the axilla, pain in the breast, bleeding from the nipple, nipple discharge and skin dimpling), or an abnormality of the breast detected during outpatient consultations referred to the Surgical Outpatient Department at the Kuopio University Hospital, Finland. There had been no pre-selection and the indications for referral in this study are in line with previously published results from a Breast Cancer Diagnostic Unit in Finland (28). The Authors maintain that this study sample can be considered clinically representative for this type of prospective case–control study design. It should be noted that the control group (healthy individuals) of the current study is not representative of the whole population, since it consists of women who presented primarily with breast symptoms.
In summary, although there was a trend for the women with HSS to have less pessimism, sadness and self-accusations than these of the BC and BBD groups, these findings do not support the hypothesis of a relationship between the BDI and BC risk.
Acknowledgements
We thank Ms A.K. Lyytinen, R.N. for help in data collection. The support from Academy of Finland, Paavo Koistinen Foundation and EVO funds from Kuopio University Hospital are gratefully acknowledged.
- Received November 18, 2010.
- Revision received December 15, 2010.
- Accepted December 16, 2010.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Moderate/severe Depression (MADRS) Can Affect the Quality of Life and Outcome Among Patients Admitted to Breast Cancer Diagnosis Unit
- Beck Depression Inventory as a Predictor of Long-term Outcome Among Patients Admitted to the Breast Cancer Diagnosis Unit: A 25-year Cohort Study in Finland
- Suicidal Ideation Versus Hopelessness/Helplessness in Healthy Individuals and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-control Study in Finland
- Agreement Between Hopelessness/Helplessness and Montgomery-Asberg Depression Rating Scale in Healthy Individuals and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-Control Study in Finland
- Emotional Personality/Proximity Versus Emotional Authenticity in Patient-Physician Communication in Healthy Study Participants, and in Patients with Benign Breast Disease, and Breast Cancer: A Prospective Case-Control Study in Finland
- The Relation of Hopelessness/Helplessness versus Beck Depression Inventory (BDI) in Healthy Individuals and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-control Study in Finland
- The Self-Rating Score (SRS) Versus the Examiner Rating Score (ERS) in Measuring Helplessness in Healthy Individuals and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-Control Study in Finland
- Anger in Health, Benign Breast Disease and Breast Cancer: A Prospective Case-Control Study
- Contribution of Emotional Distance and Reserve in Patient-Physician Communication in Healthy Study Patients, and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-Control Study in Finland
- Measurement of Pessimism: Hopelessness Scale in Healthy Study Subjects, and in Patients with Benign Breast Disease and Breast Cancer: A Prospective Case-Control Study in Finland
- Assessment of 'Cancer-prone Personality' Characteristics in Healthy Study Subjects and in Patients with Breast Disease and Breast Cancer Using the Commitment Questionnaire: A Prospective Case-Control Study in Finland
- Sifneos Alexithymia Questionnaire in Assessment of General Alexithymia in Patients with Breast Disease and Breast Cancer: A Prospective Case-Control Study in Finland
- Assessment of General Anxiety in Patients with Breast Disease and Breast Cancer Using the Spielberger STAI Self Evaluation Test: A Prospective Case-Control Study in Finland