Article Text

Abstract
Objective The clinicopathological significance of four morphological types of intraductal papillary mucinous neoplasms of the pancreas (IPMNs; gastric, intestinal, pancreatobiliary and oncocytic) was assessed.
Design Retrospective multicentre analysis of 283 surgically resected IPMNs.
Results Of the 283 IPMNs, 139 were of the gastric type, 101 were intestinal, 19 were pancreatobiliary and 24 were oncocytic. These types were significantly associated with clinicopathological factors including sex (p=0.0032), age (p=0.00924), ectatic duct size (p=0.0245), detection of mural nodules (p=4.09×10−6), histological grade (p<2.20×10−16), macroscopic types with differential involvement of the pancreatic duct system (p=3.91×10−5), invasive phenotypes (p=3.34×10−12), stage (p<2.20×10−16) and recurrence (p=0.00574). Kaplan–Meier analysis showed significant differences in patient survival by morphological type (p=5.24×10−6). Survival rates at 5 and 10 years, respectively, were 0.937 (95% CI 0.892 to 0.984) for patients with gastric-type IPMNs; 0.886 (95% CI 0.813 to 0.965) and 0.685 (95% CI 0.553 to 0.849) for those with intestinal-type IPMNs; 0.839 (95% CI 0.684 to 1.000) and 0.734 (95% CI 0.526 to 1.000) for those with oncocytic-type IPMNs; and 0.520 (95% CI 0.298 to 0.909) and undetermined for those with pancreatobiliary-type IPMNs. Analysis by the Cox proportional hazards model comparing prognostic risks determined by stage and the morphological and macroscopic types indicated that staging was the most significant predictor of survival (p=3.68×10−8) followed by the morphological type (p=0.0435). Furthermore, the morphological type remained a significant predictor in a subcohort of invasive cases (p=0.0089).
Conclusion In this multicentre retrospective analysis, the morphological type of IPMN appears to be an independent predictor of patient prognosis.
- IPMN
- subtype
- prognosis
- clinicopathologic feature
- pancreatic cancer
- pancreatic pathology
- pancreatic surgery
- pancreatic tumours
Statistics from Altmetric.com
- IPMN
- subtype
- prognosis
- clinicopathologic feature
- pancreatic cancer
- pancreatic pathology
- pancreatic surgery
- pancreatic tumours
Significance of this study
What is already known about this subject?
Intraductal papillary mucinous neoplasms of the pancreas (IPMNs) comprise four distinct morphological variants (the gastric, intestinal, pancreatobiliary and oncocytic types) which have been described recently.
Differences in the clinical manifestations and prognostic parameters between the morphological types have not been documented thoroughly.
What are the new findings?
Morphological variation of IPMNs was associated with sex, age, imaging studies, histological grading, macroscopic variations, invasiveness, stage, recurrence and prognosis of patients with IPMNs.
A Cox proportional hazards model analysis comparing prognostic risks, determined by morphological type, stage and macroscopic variation, indicated that the morphological type was an independent prognostic factor.
How might it impact on clinical practice in the foreseeable future?
Assessing the morphological type of IPMNs may provide useful information for clinical management of patients with IPMNs.
These results may stimulate efforts to evaluate morphological types in cytological or biopsied specimens and to develop biochemical markers for the different IPMN types.
Introduction
Intraductal papillary mucinous neoplasms of the pancreas (IPMNs) are characterised by the presence of dilated and, frequently, cystic pancreatic ducts filled with mucus.1 Neoplastic cells line these dilated ducts and often form well-developed papillae with varying degrees of atypia.2 IPMN lesions are often non-invasive and are hence considered surgically curable. However, some patients with IPMNs develop invasive ductal adenocarcinoma or recurrent IPMNs, even after undergoing complete resection of non-invasive IPMNs; such patients have poor prognoses. Determination of which type(s) of IPMN may predispose patients either to developing invasive ductal adenocarcinomas or to having a higher risk of disease-specific death is important for clinical management of IPMNs.
Morphological variations of IPMNs have recently been recognised and the criteria for distinguishing the four distinct subtypes—gastric, intestinal, pancreatobiliary and oncocytic—have been defined.3 This classification is based on the histomorphological features of papillae and the immunohistochemical features of mucin glycoproteins. Despite the fact that the morphological types of IPMN are well established, the differences between these types in terms of clinical manifestation have not been well documented. Therefore, the purpose of this study was to investigate whether there are any significant associations between clinicopathological features, including prognosis, and the abovementioned four morphological types by analysing the data of a large series of patients with IPMNs.
Materials and methods
Patients
We retrospectively analysed the data obtained from 283 patients with IPMN who underwent surgical resection between 1985 and 2008.
Histological grading, invasive components and staging
Histological grading of neoplasms was performed according to criteria defined by the Japan Pancreas Society (JPS).4 IPMNs were classified as intraductal papillary mucinous adenoma (IPMA) and intraductal papillary mucinous carcinoma (IPMC). An IPMN with moderate dysplasia or a borderline lesion (IPMB) by the WHO classification5 is classified with IPMA, and such lesions are described as IPMA/B in this report. IPMCs were classified as non-invasive, minimally invasive and invasive. Non-invasive IPMC corresponds to IPMN with high-grade dysplasia in the WHO classification. A minimally invasive IPMC is defined as having invaded slightly beyond the ductal wall according to the JPS classification.4 Invasive components in invasive IPMCs were classified as invasive colloid carcinoma, invasive oncocytic carcinoma or invasive tubular adenocarcinoma. When more than two histological types of invasive components were observed in a case, the most dominant type was documented as the invasive component of such a case. Staging was made according to the TNM staging system described in the American Joint Committee on Cancer (AJCC) Staging Handbook6 with the following slight modification. In this study we defined IPMA/B as Tisa and then TisaN0M0 was assessed as stage 0A.
Macroscopic type (differential involvement of the pancreatic duct system)
Macroscopic types of IPMNs, classified into main duct-type, branch duct-type and mixed-type IPMNs based on differential involvement of the pancreatic duct system, were determined by clinical imaging studies and macroscopic investigations of resected specimens according to criteria described previously.7
Morphological type
As mentioned above, tumors were morphologically classified into four distinct types (gastric, intestinal, pancreatobiliary and oncocytic) based on their microscopic morphology and immunohistochemical reactivity against anti-mucin 1 (MUC1), anti-mucin 2 (MUC2) and anti-mucin 5AC (MUC5AC) antibodies according to previously described criteria (figure 1).3 In brief, gastric-type IPMNs have thick finger-like papillae that express MUC5AC but not MUC1 or MUC2; intestinal-type IPMNs have villous papillae that consistently express MUC2 and MUC5AC but not MUC1; pancreatobiliary-type IPMNs have complex thin branching papillae that focally express MUC1 and consistently express MUC5AC but not MUC2; and oncocytic-type IPMNs have complex thick papillae comprised of eosinophilic oncocytic cells that express MUC5AC consistently and MUC1 and/or MUC2 focally. In patients with multiple morphologically distinct IPMNs, each neoplasm was classified depending on papillae type of the highest histological grade or the most dominant component present in the area of the same histological grade.
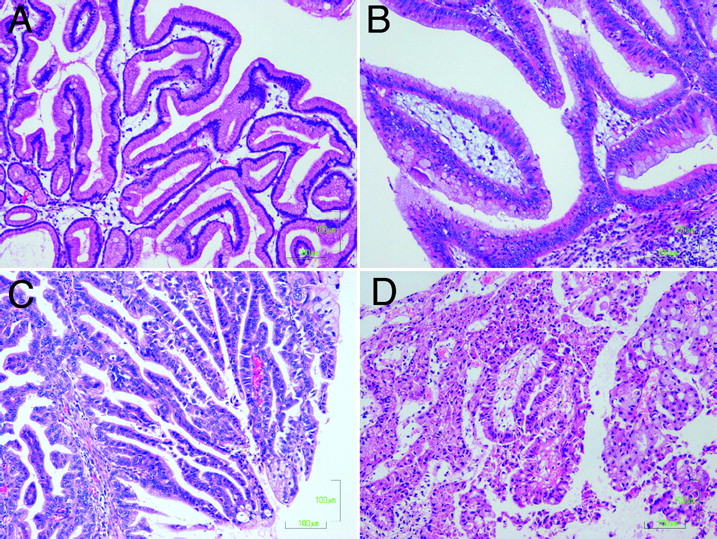
Morphological types of intraductal papillary mucinous neoplasms of the pancreas: (A) gastric type; (B) intestinal type; (C) pancreatobiliary type; (D) oncocytic type.
Statistical analysis
Statistical analysis was performed using R environment Version 2.8.1 (The R Foundation for Statistical Computing, Vienna, Austria) and PASW Statistics Version 18.0 (SPSS Inc). Correction for multiple comparisons was performed by the Bonferroni method and p values <0.05 were considered statistically significant.
Results
IPMN types and their association with clinicopathological disease features
Of the 283 patients with IPMNs studied, 139 had gastric-type, 101 had intestinal-type, 19 had pancreatobiliary-type and 24 had oncocytic-type IPMNs. Upon evaluating the relationship between the morphological type and the clinicopathological features of various IPMNs, we found that morphological type was significantly associated with sex, age, imaging studies, histological grade, macroscopic type, invasive features, stage, recurrence and outcome (table 1). However, the morphological type was not associated with serum carcinoembryonic antigen (CEA) or carbohydrate antigen 19-9 (CA19-9) (table 1).
Morphological types of IPMN and clinicopathologic features
IPMN morphological type was significantly associated with patient sex (p=0.00474, Fisher exact test; table 1). The proportion of women was higher among patients with pancreatobiliary-type IPMN than the proportion among other IPMN types (p=0.00134, Fisher exact test); this p value was lower than the threshold significance level corrected for the multiple comparisons (p<0.0125).
IPMN morphological type was also associated with patient age (p=0.00925, one-way ANOVA; table 1). Patients with oncocytic-type IPMNs were significantly younger than those with other IPMN types (p=0.0081, unpaired t test). Moreover, patients with pancreatobiliary-type IPMN tended to be older than patients with other IPMN types (p=0.037, unpaired t test).
In imaging studies the size of the ectatic duct was associated with the IPMN morphological type (p=0.0245, one-way ANOVA). In general, the size was significantly larger in intestinal type-IPMNs than gastric-type IPMNs (p=0.017, pairwise multiple comparison). Moreover, the detection of mural nodules was also associated with the morphological type (p=4.09×10−6, Fisher exact test; table 1). In particular, pancreatobiliary-type and oncocytic-type IPMNs were strongly associated with mural nodules (93% and 100% respectively).
Morphological type was also significantly associated with histological grade (p<2.2×10−16, χ2 test; table 1). Gastric-type IPMNs had a strong association with low histological grade/IPMA/B (p<2.2×10−16, Fisher exact test; OR 39.6; 95% CI 19.2 to 87.0). Conversely, other IPMN types exhibited negative associations with low histological grade (p=7.46×10−16–1.03×10−5), which raises the possibility that they are associated with higher histological grades/IPMC with or without invasion. Furthermore, intestinal-type IPMNs were particularly associated with non-invasive IPMC (p=6.73×10−6, Fisher exact test; OR 3.47; 95% CI 1.95 to 6.24). Invasive features were associated with the morphological type of IPMNs. Invasive colloid mucinous carcinomas were exclusively associated with intestinal-type IPMNs (p=5.38×10−15, Fisher exact test; OR infinity; 95% CI 717.8 to infinity). Similarly, invasive oncocytic carcinomas were exclusively associated with oncocytic-type IPMNs (p=4.06×10−5, Fisher exact test; OR infinity; 95% CI 7.79 to infinity). Moreover, invasive tubular adenocarcinomas were strongly associated with pancreatobiliary-type IPMNs (p=3.28×10−8, Fisher exact test; OR 20.8; 95% CI 6.60 to 69.0). These positive associations between gastric-type IPMNs and IPMA/Bs, intestinal-type IPMNs and non-invasive IPMCs, intestinal-type IPMNs and invasive colloid carcinomas, oncocytic-type IPMNs and invasive oncocytic carcinomas, and pancreatobiliary-type IPMNs and invasive tubular adenocarcinomas were significant even after applying multiple comparison correction (significance level 0.00200). Despite the fact that the p value did not reach the threshold, minimal invasion was observed more frequently in oncocytic-type IPMNs (p=0.0148, Fisher exact test): in 5/19 minimally invasive IPMNs and 19/264 IPMNs without minimal invasion.
IPMN morphological type was also significantly associated with disease stage (p<2.2×10−16, χ2 test; table 1). Gastric-type IPMNs were strongly associated with stage 0A (non-invasive low/moderate grade neoplasms) (p<2.2×10−16, Fisher exact test; OR 39.7; 95% CI 19.8 to 79.8). Both intestinal-type and oncocytic-type IPMNs were associated with stage 0 (p=1.82×10−6, Fisher exact test; OR 3.72; 95% CI 2.15 to 6.48; and p=0.0046, Fisher exact test; OR 3.58; 95% CI 1.48 to 8.68, respectively). Conversely, gastric-type IPMNs and other types of IPMNs were negatively associated with stage 0 (p=5.67×10−12, Fisher exact test; OR 0.126; 95% CI 0.065 to 0.243) and stage 0A (p=2.76×10−16–6.38×10−6), respectively. Pancreatobiliary-type IPMNs were associated with stage IIB (p=6.58×10−4, Fisher exact test; OR 8.8; 95% CI 2.89 to 27.0).
IPMN morphological type was significantly associated with its macroscopic type (p=8.73×10−7, Fisher exact test; table 1). In our series, 64.7% of gastric-type IPMNs and only 32.6% of IPMNs of other types were classified as the branch duct-type (p=7.22×10−8, Fisher exact test; OR 3.77; 95% CI 2.25 to 6.39). Conversely, gastric-type IPMNs were negatively associated with the main duct-type (p=7.26×10−5, Fisher exact test; OR 0.363; 95% CI 0.210 to 0.618). In contrast, 53.5% of intestinal-type IPMNs and only 26.4% of other morphological types of IPMNs were of the main duct-type; intestinal-type IPMNs were significantly associated with the main duct-type (p=9.27×10−6, Fisher exact test; OR 3.19; 95% CI 1.86 to 5.52). Conversely, intestinal-type IPMNs were negatively associated with the branch duct-type (p=2.71×10−7, Fisher exact test; OR 0.258; 95% CI 0.146 to 0.448). These two positive associations (ie, between gastric-type IPMNs and branch duct-type and between intestinal-type IPMNs and main duct-type) were significant even after adjusting for multiple comparisons (significance level 0.00416). However, pancreatobiliary-type and oncocytic-type IPMNs were not significantly associated with any particular macroscopic types (p>0.0916).
Survival of patients with IPMN
Disease-specific survival rates were estimated using the Kaplan–Meier method. The mean follow-up period was 54 months. Of the 282 patients for whom survival data were available, 40 had recurrences and 32 died of the disease. Among the 40 patients who developed recurrences, 5 presented with IPMN in the remnant pancreas, including 4 who underwent subsequent total pancreatectomy and survived. The other 35 developed ductal adenocarcinoma (15 had local recurrence, 13 had liver metastasis, 15 presented with peritoneal dissemination, 3 developed lung metastases and 1 had bone metastasis). Of the 32 patients who died, 7 had gastric-type, 15 had intestinal-type, 4 had oncocytic-type and 6 had pancreatobiliary-type IPMNs. Furthermore, of these 32 patients, 7 had non-invasive IPMNs and 25 had invasive IPMNs. Of the 7 patients with non-invasive IPMNs, 6 had intestinal-type IPMCs and 1 had gastric-type IPMA. Of note, these 7 patients developed recurrent tumors in the remnant pancreas after the initial surgery. Furthermore, the patient with gastric-type IPMA who died developed cancer in the remnant pancreas 4 years after the initial surgery. It was recorded that, during the initial surgery, this patient underwent medial (segmental) pancreatectomy and low-grade dysplastic lesions were seen on the surgical margin. Although we were curious to know whether the recurrent tumour was associated with the initial gastric-type IPMA, no further information was available for this case.
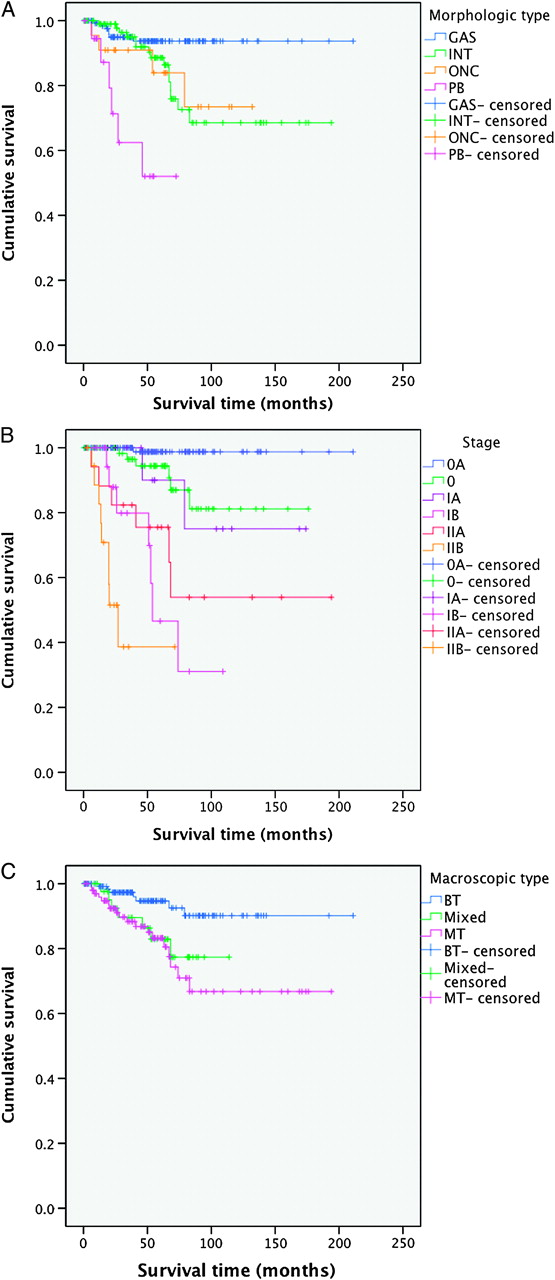
Morphological type was significantly associated with patient prognosis (p=5.24×10−6, log rank test; figure 2A). Patients with gastric-type IPMNs had a fair prognosis (5- and 10-year survival rates of 0.937 (95% CI 0.892 to 0.984)). Patients with intestinal-type and oncocytic-type IPMNs had relatively less favorable prognosis (5- and 10-year survival rates of 0.886 (95% CI 0.813 to 0.965) and 0.685 (95% CI 0.553 to 0.849), respectively, in patients with intestinal-type IPMNs and 0.839 (95% CI 0.684 to 1.000) and 0.734 (95% CI 0.526 to 1.000), respectively, in those with oncocytic-type IPMNs). Patients with pancreatobiliary-type IPMNs had the poorest prognosis with a 5-year survival rate of only 0.520 (95% CI 0.298 to 0.909). The 10-year survival rate for this group was not considered because surviving patients were censored for less than 10 years of follow-up.
{kind=link}
{kind=link}
Kaplan–Meier survival curves to show the cumulative survival of patients with intraductal papillary mucinous neoplasms (IPMNs) according to (A) morphological types of IPMN (p=5.24×10−6, log rank test; GAS, gastric-type; INT, intestinal-type; ONC, oncocytic-type; PB, pancreatobiliary-type); (B) stage of IPMN (stage 0A categorises non-invasive low or moderate grade neoplasms; p<2.2×10−16, log rank test); and (C) macroscopic type of IPMN (p=0.0084, log rank test; BT, branch duct-type; Mixed, mixed-type; MT, main duct-type).
Disease stage was associated with patient prognosis (p<2.2×10−16, log rank test; figure. 2B). Specifically, the 5- and 10-year survival rates were both 0.987 (95% CI 0.963 to 1.000) for patients with stage 0A; 0.944 (95% CI 0.884 to 1.000) and 0.812 (95% CI 0.672 to 0.980) for patients with stage 0; 0.900 (95% CI 0.732 to 1.00) and 0.750 (95% CI 0.496 to 1.00) for patients with stage IA; 0.466 (95% CI 0.237 to 0.915) and undetermined for patients with stage IB; 0.755 (95% CI 0.571 to 0.997) and 0.539 (95% CI 0.313 to 0.930) for patients with stage IIA; and 0.386 (95% CI 0.185 to 0.808) and undetermined for those with stage IIB, respectively. We had no patient with stage III nor included the single patient with stage IV in this survival analysis.
IPMN macroscopic type was also associated with patient prognosis (p=0.0084, log rank test; figure 2C). Patients with branch duct-type IPMNs had fair prognoses (5- and 10-year survival rates 0.947 (95% CI 0.901 to 0.994) and 0.901 (95% CI 0.829 to 0.980), respectively), patients with main duct-type IPMNs had less favourable prognoses (5- and 10-year survival rates 0.832 (95% CI 0.750 to 0.923) and 0.668 (95% CI 0.534 to 0.834), respectively) and patients with mixed-type IPMNs also had less favourable prognoses (5-year survival rate 0.829 (95% CI 0.711 to 0.966); the 10-year survival rate was not available for this group).
We applied the Cox proportional hazards model analysis to our dataset to compare the risks determined by staging and morphological and macroscopic typing. Different classes of the stages, morphological types and macroscopic types were incorporated as covariates in the model and disease-specific death was defined as the outcome (table 2). This analysis indicated that disease staging was the most significant predictor of survival (p=3.68×10−8), followed by the morphological type (p=0.0435). Specifically, stage IIB exhibited the highest risk, followed by stages IB, IIA, IA and 0 compared with stage 0A (table 2). We omitted data for the patient with stage IV because there was only one patient in the cohort. For morphological typing, pancreatobiliary-type IPMNs exhibited the highest risk, followed by the gastric-type, oncocytic-type and intestinal-type (table 2). However, the different macroscopic types did not reveal significantly different risks. When evaluating the prognostic factors in a subcohort of invasive cases, we found that the IPMN morphological type was the most significant predictor of survival (p=0.0089) followed by disease stage (p=0.0170) (table 2). In the cohort, pancreatobiliary-type IPMNs showed the highest risk compared with intestinal-type IPMNs (p=0.0012). These results indicate that the morphological type of an IPMN is an independent predictor of patient prognosis compared with staging or macroscopic type.
Cox proportional hazards model analysis
Discussion
IPMNs are known to exhibit a wide spectrum of histomorphological variations that are thought to be associated with varying clinicopathological features. In their study of 24 patients with IPMNs, Yonezawa et al noted that morphological variations of IPMNs classifiable into three distinct types (villous dark cell type, papillary clear cell type and compact cell type) were associated with different clinical outcomes.8 Lüttges et al also described three distinct variants in 51 patients with IPMNs that were associated with histological grade and invasion.9 Adsay et al introduced 11 cases of intraductal oncocytic papillary neoplasms that had distinctive clinicopathological features.10 Furthermore, this group also reported three distinct variants (the intestinal type, pancreatobiliary type and null type) in 74 IPMNs that were associated with different histological grades and invasion, and also with different clinical outcomes.11 12 Ban et al described 80 cases of IPMNs, comprised of 50 gastric-type and 30 intestinal-type IPMNs, and showed the contrasting features of these two types with respect to involvement of ducts and histological grading.13 Collectively, these studies suggest that distinctive morphological variations of IPMNs are associated with different clinicopathological features and prognoses. However, these conclusions were based on results obtained from a small number of cases and short-term follow-up periods. Also, a clear-cut conclusion has not been reached regarding the significance of the variations in prognosis and clinical management of patients due to confusion in the nomenclature and criteria for subclassifying morphological variations of IPMNs. Recent consensus studies classifying the morphological variants of IPMNs into four distinct types—namely, gastric-type, intestinal-type, pancreatobiliary-type, and oncocytic-type—paved the way for determination of the clinicopathological significance of these variants.3 Based on this consensus classification, our current multi-institutional retrospective study on 283 patients with IPMNs has confirmed some of the previous studies and has also demonstrated clear statistical associations between morphological type and sex, age, imaging, histological grade, macroscopic variations based on the differential involvement of the pancreatic ductal system, invasive features, stage, recurrence and patient prognosis. Analysis by the Cox proportional hazards model comparing prognostic risks determined by stage and morphological and macroscopic types indicated that staging was the most significant predictor of survival, followed by morphological type. Furthermore, the morphological type remained a significant predictor in a subcohort of invasive cases. Although this study was a retrospective multicentre analysis of surgically resected IPMNs with possible understaging of the cases for suboptimal sampling of the surgical specimen, morphological type appears to be an independent predictor of patient prognosis.
Gastric-type IPMNs were associated with a lower histological grade, involvement of branch ducts, absence of invasion, stage 0A and fair survival. These associations of gastric-type IPMNs with low histological grade, branching ducts and non-invasive phenotypes were consistent with previously published reports.12–14 Of note, Nakamura et al studied 50 patients with IPMNs and reported that the prognosis was better in the patients without MUC2 expression or gastric-type IPMNs than in those with MUC2 expression or intestinal-type IPMNs. However, Adsay et al reported that, in their analysis of 74 patients with IPMNs, the prognosis of patients with null-type IPMNs or gastric-type IPMNs was worse than for those with intestinal-type IPMNs.12 In their analysis, 4/23 patients with null or gastric-type IPMNs had invasive tubular adenocarcinoma, which may have been responsible for the poor prognoses. Notably, in our series, of the 139 patients with gastric-type IPMNs, 7 died of the disease; of these 7 patients, 5 presented with invasive tubular adenocarcinomas. One of these patients was noted to have developed cancer in the remnant pancreas 4 years after he underwent an initial surgery for gastric-type IPMA. The results indicate that, although most patients with gastric-type IPMNs have non-invasive phenotypes and fair prognoses, the possibility of developing invasive tubular adenocarcinoma with this type remains, which can lead to a poor outcome.
Intestinal-type IPMNs were associated with non-invasive IPMCs, invasive colloid carcinomas in those cases with invasion, stage 0, involvement of the main duct and less favourable prognosis. Invasive IPMCs with colloid carcinomas were exclusively associated with intestinal-type IPMNs and had a better prognosis than invasive IPMCs with tubular adenocarcinoma, which is consistent with results described elsewhere.12–14 Furthermore, some cases of non-invasive intestinal-type IPMCs had unfavourable prognosis with tumour recurrence in long-term follow-up; this observation was uncommon in other types of IPMCs, which indicates that non-invasive intestinal-type IPMCs have a greater potential for long-term recurrence than non-invasive IPMCs of other types. Because IPMNs without invasive cancer can typically be resected completely, the prognosis should be excellent. However, some of patients with non-invasive IPMNs did have a recurrence in the remnant pancreas. These recurrences may be a result of residual neoplasm including multifocal disease that may not be recognised at the time of surgery, or the metachronous development of IPMN which requires further detailed histological and molecular studies.
Pancreatobiliary-type IPMNs tended to occur with a slight preference in older women and were associated with high histological grades, invasive phenotypes characterised by tubular adenocarcinoma, stage IIB and poor prognosis. The predominance in women was quite distinctive from the sex distribution of other IPMN types in our series. Such female predominance has not been described previously.11 12 However, additional studies are required to determine if this finding is due to a small number of patients with this IPMN type. According to the results of the Cox proportional hazards analysis, pancreatobiliary-type IPMNs had the highest prognostic risk of the four types. This was particularly evident in a subcohort of patients with invasive disease. This result may be due to the high susceptibility of this IPMN type to develop invasive tubular adenocarcinoma, which is inevitably responsible for the worst prognosis in pancreatic neoplasms. The association of pancreatobiliary-type IPMNs with tubular adenocarcinoma is described elsewhere.11 12 It is noteworthy that, in contrast to invasive pancreatobiliary-type IPMNs, non-invasive pancreatobiliary-type IPMNs can have a fair prognosis as evidenced by the fact that none of the patients with this type of non-invasive IPMN in our series died. This result may emphasise the importance of early diagnosis of pancreatobiliary-type IPMNs.
Oncocytic-type IPMNs were more likely to develop in younger people than were other IPMN types. These IPMNs were associated with a high histological grade, minimal invasion, invasive oncocytic carcinoma in the cases with invasion, stage 0 and less favourable prognosis. The long-term prognosis of patients with oncocytic-type IPMNs has not been well documented. In our study, patients with oncocytic-type IPMNs exhibited survival rates of 80.3% at 5 years and 70.2% at 10 years, which is comparable to the survival rates for patients with intestinal-type IPMNs. We also showed that the association between oncocytic-type IPMNs and minimally invasive phenotypes was the characteristic feature for this type. Adsay et al described one patient with minimal invasion in their cohort.10
Previous reports have documented the prognostic significance of staging and the macroscopic type in patients with IPMNs.15 16 In this study we compared the prognostic significance of the IPMN morphological type with that of staging and the macroscopic type using Cox proportional hazards model analysis to determine whether it was an independent prognostic factor. We found that both staging and the morphological type were significantly and independently associated with prognosis. Furthermore, the morphological type remained the significant predictor in a subcohort of invasive cases. Of the morphological types, the pancreatobiliary-type IPMNs had a significantly greater risk than the intestinal-type IPMNs. This result may reflect the aggressive nature of pancreatobiliary-type IPMNs compared with the indolent nature of intestinal-type IPMNs.
We suggest that assessing the morphological type of IPMNs may contribute to better clinical management of patients with IPMNs. The current recommendations for the preoperative management of patients with IPMNs depend on the size of the lesion, the differential involvement of ducts (main or branch) and the presence of mural nodules. An IPMN with involvement of the main duct, a lesion larger than 3 cm and/or mural nodules is likely to have a high-grade or an invasive phenotype and hence surgical resection is recommended for such a neoplasm. However, as the results of this study indicate, IPMNs are heterogeneous diseases comprised of different morphological types that are associated with distinct clinicopathological characteristics. Therefore, if we can identify the morphological IPMN types of patients, it may help to predict the clinical course of the neoplasms. For instance, a gastric-type IPMN is usually a localised low-grade lesion; an intestinal-type IPMN tends to be a diffuse high-grade lesion with considerable probability of recurrence; a pancreatobiliary-type IPMN is likely to have an invasive lesion of tubular adenocarcinoma; and an oncocytic-type IPMN may have a minimally invasive lesion. These predictions may facilitate the design of appropriate surgical procedures, adjuvant therapies and follow-up regimens for patients with IPMNs. For example, variations in surgery may be used to target the different IPMN types; we may need to consider using a limited pancreatectomy for removal of a localised gastric-type IPMN, an extensive and often total pancreatectomy for an intestinal-type IPMN, a radical pancreatectomy for a pancreatobiliary-type IPMN, and a standard pancreatectomy for an oncocytic-type IPMN. Furthermore, the high risk of disease-specific death due to invasive pancreatobiliary-type IPMNs may illustrate the requirement for adjuvant therapy. For follow-up clinical scheduling, both invasive IPMNs and non-invasive intestinal-type IPMNs should probably be carefully examined for recurrence. These issues for potential clinical applications should be further determined by a prospective standardised study. Cytological preparations or biopsied samples of the tips of tumours have been shown to act as a diagnostic tool for determining both the grade and morphological type of neoplasms.17 18 Chemical analyses of cyst fluid may also be interesting because some studies have demonstrated diagnostic values of MUC and CEA in cyst fluid in cystic neoplasms including IPMN.19 20 Whether we can consistently identify the morphological types of IPMNs based on preoperative cytological, histopathological or chemical analyses needs to be clarified in a further study.
The results of the current study may stimulate efforts to evaluate biochemical markers of the morphological types of IPMNs which would be particularly useful for clinical purposes.
References
Footnotes
Funding This work was supported in part by a grant-in-aid from the Ministry of Education, Culture, Sports, Science and Technology and by the Program for Promoting the Establishment of Strategic Research Centers, Special Coordination Funds for Promoting Science and Technology, Ministry of Education, Culture, Sports, Science and Technology (Japan).
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of Tokyo Women's Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.