Article Text

Abstract
Background and Aims Knowledge on the aetiology of exocrine pancreatic cancer (EPC) is scant. The best established risk factor for EPC is tobacco smoking. Among other carcinogens, tobacco contains cadmium, a metal previously associated with an increased risk of EPC. This study evaluated the association between concentrations of trace elements in toenails and EPC risk.
Methods The study included 118 EPC cases and 399 hospital controls from eastern Spain. Levels of 12 trace elements were determined in toenail samples by inductively coupled plasma mass spectrometry. OR and 95% CI, adjusted for potential confounders, were calculated using logistic regression.
Results Significantly increased risks of EPC were observed among subjects whose concentrations of cadmium (OR 3.58, 95% CI 1.86 to 6.88; ptrend=5×10−6), arsenic (OR 2.02, 95% CI 1.08 to 3.78; ptrend=0.009) and lead (OR 6.26, 95% CI 2.71 to 14.47; ptrend=3×10−5) were in the highest quartile. High concentrations of selenium (OR 0.05, 95% CI 0.02 to 0.15; ptrend=8×10−11) and nickel (OR 0.27, 95% CI 0.12 to 0.59; ptrend=2×10−4) were inversely associated with the risk of EPC.
Conclusion Novel associations are reported of lead, nickel and selenium toenail concentrations with pancreas cancer risk. Furthermore, the results confirm previous associations with cadmium and arsenic. These novel findings, if replicated in independent studies, would point to an important role of trace elements in pancreatic carcinogenesis.
- Arsenic
- cadmium
- cancer
- epidemiology
- epithelial differentiation
- genetics
- lead
- molecular carcinogenesis
- molecular epidemiology
- molecular oncology
- mucins
- pancreas
- pancreatic cancer
- pancreatic epidemiology
- pancreatic tumours
- polymorphic variation
- selenium
- statistics
Statistics from Altmetric.com
- Arsenic
- cadmium
- cancer
- epidemiology
- epithelial differentiation
- genetics
- lead
- molecular carcinogenesis
- molecular epidemiology
- molecular oncology
- mucins
- pancreas
- pancreatic cancer
- pancreatic epidemiology
- pancreatic tumours
- polymorphic variation
- selenium
- statistics
Significance of this study
What is already known about the subject?
-
Little is known about the aetiology of pancreatic cancer.
-
Some trace elements, such as arsenic and cadmium, are carcinogenic for humans and may enter the organism through different routes.
-
A few studies have found a link between exposure to arsenic and cadmium and pancreatic cancer risk.
What are the new findings?
-
Individuals with the highest levels of selenium or nickel in toenails present a lower risk of pancreatic cancer.
-
The study confirms the increased risk of pancreatic cancer among subjects with the highest levels of arsenic or cadmium in toenails.
-
Besides arsenic and cadmium, high levels of lead may also be a risk factor for pancreatic cancer.
How might it impact on clinical practice in the foreseeable future?
-
Selenium intake might be tested in clinical trials as a chemopreventive intervention in individuals at high risk of pancreatic cancer. Understanding the role of trace elements in pancreatic cancer pathogenesis could lead to preventive measures or treatments.
In spite of decades of research, the aetiology of exocrine pancreatic cancer (EPC) remains largely unknown.1 The best established risk factor for EPC is tobacco smoking, which may account for up to one third of cases.2 A personal history of diabetes, chronic pancreatitis and high body mass index, as well as a family history of cancer have also been consistently associated with an increased risk of EPC.1 In addition to aromatic amines, one of the main carcinogens involved in pancreatic carcinogenesis,3 tobacco, contains other carcinogens, including trace metals such as cadmium.4 High levels of cadmium have been associated with an increased risk of EPC.5 ,6 Recently, a potential link between pancreatic cancer mortality and childhood exposure to milk powder contaminated with arsenic has also been suggested.7 ,8 The objective of the present study was to assess the risk of EPC associated with concentrations of selected trace elements measured in toenails.
Methods
Study populations
We conducted a case–control study with incident cases of EPC included in the PANKRAS II Study,9 and hospital-based controls from the Spanish Bladder Cancer/EPICURO Study.10 The two studies had overlapping geographical recruitment areas and were performed close together in time. Case enrolment occurred during 1992–5 at five general hospitals from the Mediterranean coast in Spain. An epidemiological questionnaire was administered by trained monitors through a face-to-face interview during the first hospital admission. Sociodemographic information as well as data on tobacco smoking and past history of diabetes was considered in this analysis. Out of 185 patients with EPC included in the study, 118 (63.8%) provided pretreatment toenail samples. Controls, recruited during 1998–2001 in 18 Spanish hospitals, were patients with diagnoses unrelated to the exposures of interest.10 For the present analysis, only controls (n=441) admitted to hospitals from the same regions as those participating in the PANKRAS II Study were considered. Information on known or potential cancer risk factors, as well as toenail samples, were obtained from 399 (90.5%) controls during their inpatient hospital stay, as was done with cases. The final study sample was mainly composed of men, with a high prevalence of tobacco smokers. Cases were slightly older than controls (see supplementary table 1, available online only). Informed consent from all subjects and ethical approval from local institutional review boards were obtained.
Trace element assessment
Toenails were stored at room temperature until the time of the analysis. After careful cleaning and washing to remove external contaminants, trace elements were quantified at the Trace Element Analysis Core (Dartmouth College, Hanover, New Hampshire, USA), using inductively coupled plasma mass spectrometry.11 Toenails were acid digested with Optima nitric acid (Fisher Scientific, St Louis, Missouri, USA) at 105°C followed by the addition of hydrogen peroxide and further heating the dilution with deionised water. All sample preparation steps were recorded gravimetrically. As a quality control, each batch of analyses included six standard reference material (SRM) samples with known trace element content (GBW 07601, powdered human hair) and six analytical blanks, along with the study samples. The within and the between-assay coefficients of variation for SRM replicates were less than 15% for arsenic, manganese, lead, selenium and zinc; 15–25% for aluminium, cadmium, copper and nickel; 25–40% for iron and vanadium; and over 40% for chromium. The amount of SRM used ranged from less than 10–50 mg to mimic the mass of toenails. This small SRM sample mass may be the cause of some of the variability seen in the within and between-batch SRM results. The case–control status of study participants was not disclosed to the testing laboratory.
Statistical analysis
The Mann–Whitney U test was used to assess differences in median toenail concentrations of the trace elements between cases and controls. For association analyses, participants were divided into quartiles based on the distribution of trace element concentrations among controls, and logistic regression was applied to estimate adjusted OR and their 95% CI, with the lowest quartile as the reference category. Basic models for each trace element included age at interview (continuous), gender (dichotomous), region (three categories) and smoking status (ever/never) as covariates. Controls were classified as ever or never smokers according to the definition of smoking status of cases.12 Further adjustment was made for potential confounders such as educational level (high vs low),13 pack-years and total duration of cigarette smoking (continuous), past medical history of diabetes status (dichotomous) and for trace elements (categorical), for which an association was observed in the basic model. Tests for linear trend were computed by including the median of each quartile of the trace element concentration as a continuous variable. As controls from the Balearic Islands were not available, in a first round of analyses, cases from these islands were grouped with those of Barcelona due to their similarities and proximity. In a second round, those cases were excluded. Results were considered statistically significant with a two-sided p<0.05. Statistical analyses were performed using STATA/SE V.10·1.
Results
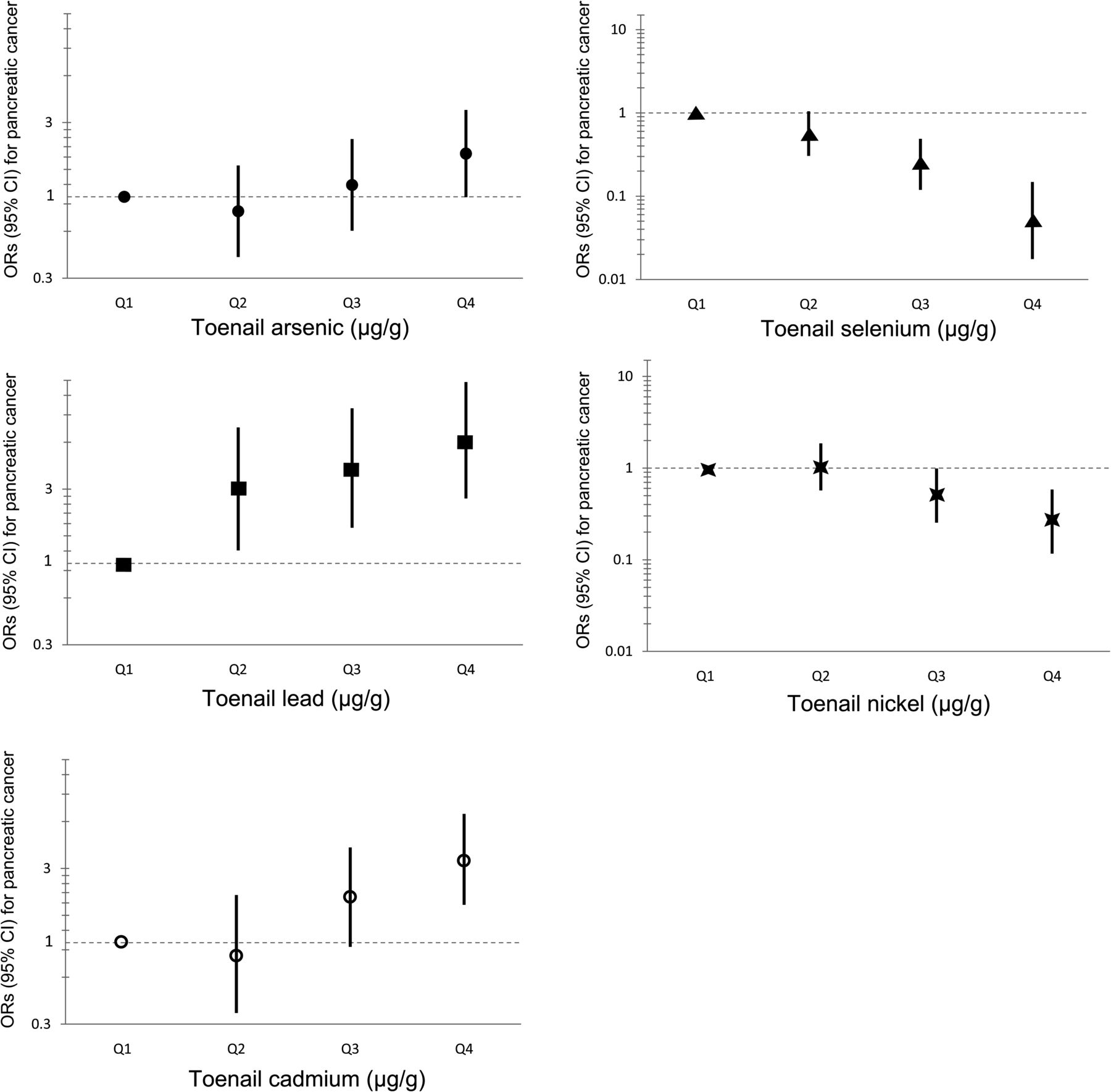
The toenail concentrations of cadmium and lead were significantly higher in cases than in controls (p<0.001). In contrast, the concentrations of nickel and selenium were lower in cases than in controls (see supplementary table 2, available online only). Comparing the highest quartile versus the lowest quartile of concentrations, an increased risk of EPC was associated with lead (adjusted OR 6.26, 95% CI 2.71 to 14.47; ptrend=3×10−5), cadmium (adjusted OR 3.58, 95% CI 1.86 to 6.88; ptrend=5×10−6) and arsenic (adjusted OR 2.02, 95% CI 1.08 to 3.78; ptrend=0.009). By contrast, levels of nickel (adjusted OR 0.27, 95% CI 0.12 to 0.59; ptrend=2×10−4) and selenium (adjusted OR 0.05, 95% CI 0.02 to 0.15; ptrend=8×10−11) were inversely associated with EPC risk (table 1 and figure 1). No statistically significant associations were observed for the other trace elements (see supplementary table 3, available online only).
OR, 95% CI and p for the associations between pancreatic cancer risk and concentrations in toenails of selected trace elements (arsenic, cadmium, lead, nickel and selenium)
{kind=link}
OR and 95% CI for pancreatic cancer risk according to the concentrations in toenails of arsenic, cadmium, lead, nickel and selenium.
Further adjustment for diabetes (see supplementary table 3, available online only) and other potential confounders did not substantially change the results (see supplementary tables 4 and 5, available online only). Additional adjustment for the elements found significant in the basic model (arsenic, cadmium, lead, nickel and selenium) did not markedly change the OR estimates, although the association with arsenic was no longer statistically significant (highest vs lowest quartile: adjusted OR 1.72, 95% CI 0.77 to 3.86; ptrend=0.201) when the lead concentration was included in the model (see supplementary table 6, available online only). The results were similar after excluding the Balearic cases from the analysis (data not shown).
Discussion
The study shows, for the first time, highly significant associations between EPC risk and toenail concentrations of lead, selenium and nickel, and confirms associations with cadmium and arsenic exposure, previously reported by a few studies.5–8 Importantly, a dose–response effect was observed for each of these associations.
Cadmium has previously been associated with an increased risk of lung, prostate and kidney cancers,14 ,15 in addition to pancreatic cancer risk and mortality.5 ,6 Cadmium is a well established carcinogen that acts on different steps of carcinogenesis, inhibiting DNA repair, and causing genomic instability.16–18 Furthermore, it causes transdifferentiation of pancreatic cells, inhibits DNA repair, and induces or regulates the activity of several oncogenes or tumour-suppressor proteins that are expressed in human pancreatic cancer.5 ,19 ,20
Arsenic exposure has been associated with an increased risk of cancer.21 Regarding its association with pancreatic cancer risk, little has been published. However, a potential relation between childhood exposure to milk powder contaminated with arsenic and an almost twofold excess mortality due to pancreatic cancer was recently reported.7 ,8 Some studies on the relationship between arsenic exposure and type 2 diabetes, which is a potential risk factor for pancreatic cancer, obtained conflicting results.22 ,23 In the present study, diabetes did not confound the association between arsenic and EPC. Inorganic arsenic is a highly toxic and carcinogenic metalloid, which can induce oxidative stress leading to the inhibition of DNA repair.15 ,21 ,24 Arsenic-induced oxidative stress also causes DNA strand breaks, alkali-labile sites and eventually DNA adducts.25 Moreover, alterations in the methylation status of oncogenes and tumour-suppressor genes, mediated by arsenic, may also play a role in carcinogenesis.26
To our knowledge, this is the first epidemiological study showing an association between lead and EPC risk. The International Agency for Research on Cancer classifies inorganic lead as ‘probably carcinogenic to humans’, and several studies found it to be linked to cancer.27–29 The possible involvement of lead in pancreatic cancer development cannot be ruled out, given the long residence time of this metal in the bone and the regular exchange between this matrix and blood and soft tissues.30 ,31 Lead induces chromosome aberrations, micronuclei and sister chromatid exchanges.32 ,33 It can activate epidermal growth factor receptor and SFK tyrosine kinases and increase Ras-GTP levels, leading to cell proliferation and differentiation.34 Furthermore, a direct association has recently been observed between bone lead levels and LINE-1 DNA hypomethylation,35 which in turn has been linked to cancer risk.36 ,37
Epidemiological evidence on nickel carcinogenicity to humans is limited and controversial. High occupational exposure to nickel has been associated with an increased risk of lung and prostate cancers,21 ,38–41 but several studies found no association with bladder, colorectal, gastric or lung cancers.42–45 A meta-analysis of occupational exposures and pancreatic cancer reported an increased risk with nickel exposure.46 However, in occupational settings nickel may be associated with high concentrations of polychlorinated biphenyls, and the latter compounds could account for the observed increased risk.9 ,47 Furthermore, no measurement of nickel concentrations in biological samples was performed in previous studies.47 Nickel may increase DNA methylation, inhibit DNA repair, and induce apoptosis through the generation of reactive oxygen species.48–51
Selenium is an essential micronutrient,52 ,53 and high levels of this trace element have been inversely associated with several cancers.54–58 While a small study published in 1989 showed a strong inverse association between serum selenium levels and pancreatic cancer risk,59 no replication studies have been published. Aberrant expression patterns of some selenoproteins show that they are relevant in scavenging reactive oxygen species and diminishing oxidative damage.60 The protection against cancer given by selenium has also been linked to the activities of hydrogen selenide and selenomethionine present in cells leading to higher methylating efficiency of RNA and thiols.61 In addition, selenium may boost p53 activity, leading either to DNA repair or apoptosis.62 Selenium seems also to play a role as an antagonist of arsenic, cadmium and lead, decreasing the oxidative stress caused by exposure to these elements.63 ,64 In the present study, the association between selenium and pancreatic cancer risk was not affected by the concentrations of those three elements.
The limitations of our study include its retrospective design, relatively small sample size, and slight difference in the recruitment period of cases and controls. Nevertheless, the appropriateness of this control group is supported by the replication of the association between smoking and EPC risk (adjusted OR 2.08, 95% CI 1.09 to 3.99; p=0.027). Regarding lead, the banning of leaded gasoline took place in Spain in January 2002, after samples from controls had been collected. Also, we did not observe differences in toenail concentrations of lead by year of recruitment among controls. Furthermore, diet is the main source of lead exposure in adults, with the exception of individuals occupationally exposed.29 ,31 Therefore, a potential decrease in concentrations of lead in the air would not necessarily imply a direct decrease in toenail lead levels in the participants of the present study. Also, lead has a long half-life in bone, from where it goes back to the blood stream and to soft tissues,30 ,31 which means that levels of lead in the organism and those measured in toenails do not reflect recent environmental changes; rather, they mirror past and chronic exposures. The study was not designed to identify the environmental sources of the trace elements found. Among the potential sources of these elements are air and water pollution, although it should be taken into account that both cases and controls share the area of residence and drinking water is publicly supplied. We adjusted for smoking, which is one source for some metals. Adjusting for diet or occupation was not possible, and these factors cannot be ruled out as sources of some of the trace elements relevant in this study. Finally, the possibility that even under similar environmental exposures, different genetic profiles between cases and controls might account for pancreatic cancer risk cannot be excluded.
The study also has important strengths, including the matching on area of residence, the similar age distributions of cases and controls, and the simultaneous quantification of the trace elements in the same laboratory and under the same quality control procedures. Furthermore, toenails are not altered with long-term storage and they are reliable matrices to assess past exposures.65–70
In conclusion, our results support an increased risk of pancreatic cancer associated with higher levels of cadmium, arsenic and lead, as well as an inverse association with higher levels of selenium and nickel. While our findings need to be replicated in independent studies, they suggest a role of trace elements in pancreatic cancer pathogenesis, and justify further research.
Acknowledgments
The authors acknowledge the coordinators, field and administrative workers, technicians and patients of both the PANKRAS II and Spanish Bladder Cancer/EPICURO studies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
-
Funding This work was partly supported by the Association for International Cancer Research (AICR09-0780), Fondo de Investigación Sanitaria, Spain (#PI09-02102), Red Temática de Investigación Cooperativa en Cáncer (RTICC) and CIBER de Epidemiología y Salud Pública (CIBERESP), Instituto de Salud Carlos III, Ministry of Health, Spain, Fundación Científica de la Asociación Española Contra el Cáncer (AECC) and the Intramural Research Program of the Division of Cancer Epidemiology and Genetics, National Cancer Institute, USA. The Dartmouth Trace Element Core is partly supported by NIH grant number P42 ES007373 from the National Institute of Environmental Health Sciences.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was obtained from local institutional review boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editor's quiz: GI snapshot