Article Text

Abstract
The objective of this study was to review and summarise the published evidence for an association between circulating concentrations of C reactive protein (CRP) and cancer through a systematic review. 90 discrete studies were identified. 81 (90%) were prevalent case–control or cross-sectional studies, and only 9 studies had a prospective design. In most prevalent studies, CRP concentrations were found to be higher in patients with cancer than in healthy controls or controls with benign conditions. Of the nine large prospective studies identified in this review, four reported no relationship between circulating CRP levels and breast, prostate or colorectal cancers, and five studies found that CRP was associated with colorectal or lung cancers. Most of the studies evaluating CRP as a diagnostic marker of cancer did not present relevant statistical analyses. Furthermore, any association reported in the prevalent studies might reflect reverse causation, survival bias or confounding. The prospective studies provided no strong evidence for a causal role of CRP in cancer. Instead of further prevalent studies, more large prospective studies and CRP gene–cancer association studies would be valuable in investigating the role of CRP in cancer.
- CRP, C reactive protein
- IL, interleukin
Statistics from Altmetric.com
C reactive protein (CRP) is a marker of acute-phase inflammatory response. It is produced mainly by hepatocytes, and its production is regulated by interleukin 6 (IL6). Both genetic and environmental factors influence an individual’s basal CRP concentration,1,2 and thus circulating CRP levels in apparently healthy people can vary from 0.1 to 10 mg/l.1 Increased CRP concentrations have been reported in many diseases, including cardiovascular diseases, type 2 diabetes, arthritis and many types of cancers.1,3–7
Several possible mechanisms have been proposed for the relationship between CRP and cancer. First, tumour growth can cause tissue inflammation and hence increase CRP levels.8,9 Second, CRP could be an indicator of an immune response to tumour antigens.10–12 Third, there is evidence that cancer cells can increase the production of inflammatory proteins, which could explain the high CRP concentrations in patients with cancer. Some cancerous cells have been shown to express CRP2,6,13 and cancer cell lines have been shown to secrete IL6 and IL8, which in turn induce the production of CRP.14,15 These mechanisms imply that increased CRP is a response to the neoplastic process and that CRP concentrations could thus provide a marker for identifying people with cancer at an early stage when treatment might be more effective. Finally, chronic inflammation, of which CRP is an important marker, might have an aetiological role in cancer. It has been suggested that inflammation creates a tissue microenvironment where the reactive oxygen and nitrogen species released by inflammatory cells could cause potentially malignant DNA alterations,16 and that some inflammatory cytokines and proteins in chronic inflammation promote tumour growth.17,18
The prognostic use of CRP and other inflammatory markers has been demonstrated in many forms of cancer,7 but the epidemiological evidence for a diagnostic or an aetiological role of circulating CRP in cancer has been inconsistent to date. Given the large and increasing body of research in this area, with different claims about the role of CRP in malignancy, we undertook a systematic review of the literature in order to summarise the currently available evidence for the role of circulating CRP in the diagnosis and aetiology of cancer, to assess the quality of studies and to discuss where further research resources in this area would be best placed.
MATERIALS AND METHODS
Electronic databases Medline, Embase and the Cochrane Library were searched systematically on 1 July 2006. The Web of Science database was searched for publications citing the articles identified from previous searches, and publications cited in the reviewed articles were included where relevant. Table 1 details the search terms used. Studies of any type of cancer in humans, written in any language and comparing patients with cancer with apparently healthy people or with people with benign conditions were included. Where more than one paper had been published using data from the same study, all publications were reviewed, but where duplication of the CRP data was apparent, the latest or the most conclusively reported study was included in the summary of studies. Any study including results of the relationship between CRP and any type of cancer was included in the review, irrespective of the primary focus of the study. As our aim in this review was to assess the role of circulating CRP in the diagnosis or aetiology of cancer, we did not specifically search for studies investigating CRP as a prognostic marker of cancer. However, as we extensively searched for studies comparing CRP concentrations in patients with cancer and in people free of malignant diseases, we found studies evaluating CRP as a prognostic marker that also included a control group free of malignant diseases. These studies were included in the review if they presented relevant results.
Search terms used in this study
If the title or abstract of the article seemed relevant, the abstract and, where necessary, the full text were reviewed to decide whether it should be included. Two reviewers (KH and DAL) independently extracted data from 50% of the publications using a standard data extraction sheet, and as the reviewers agreed on the extracted information over 95% of the time, KH extracted the data from the remaining papers and any uncertain issues were addressed by further joint inspection of the papers and discussion (with DAL). As the hypotheses, cancer types and designs of the identified studies were markedly different, it was deemed inappropriate to pool the results using meta-analysis.
RESULTS
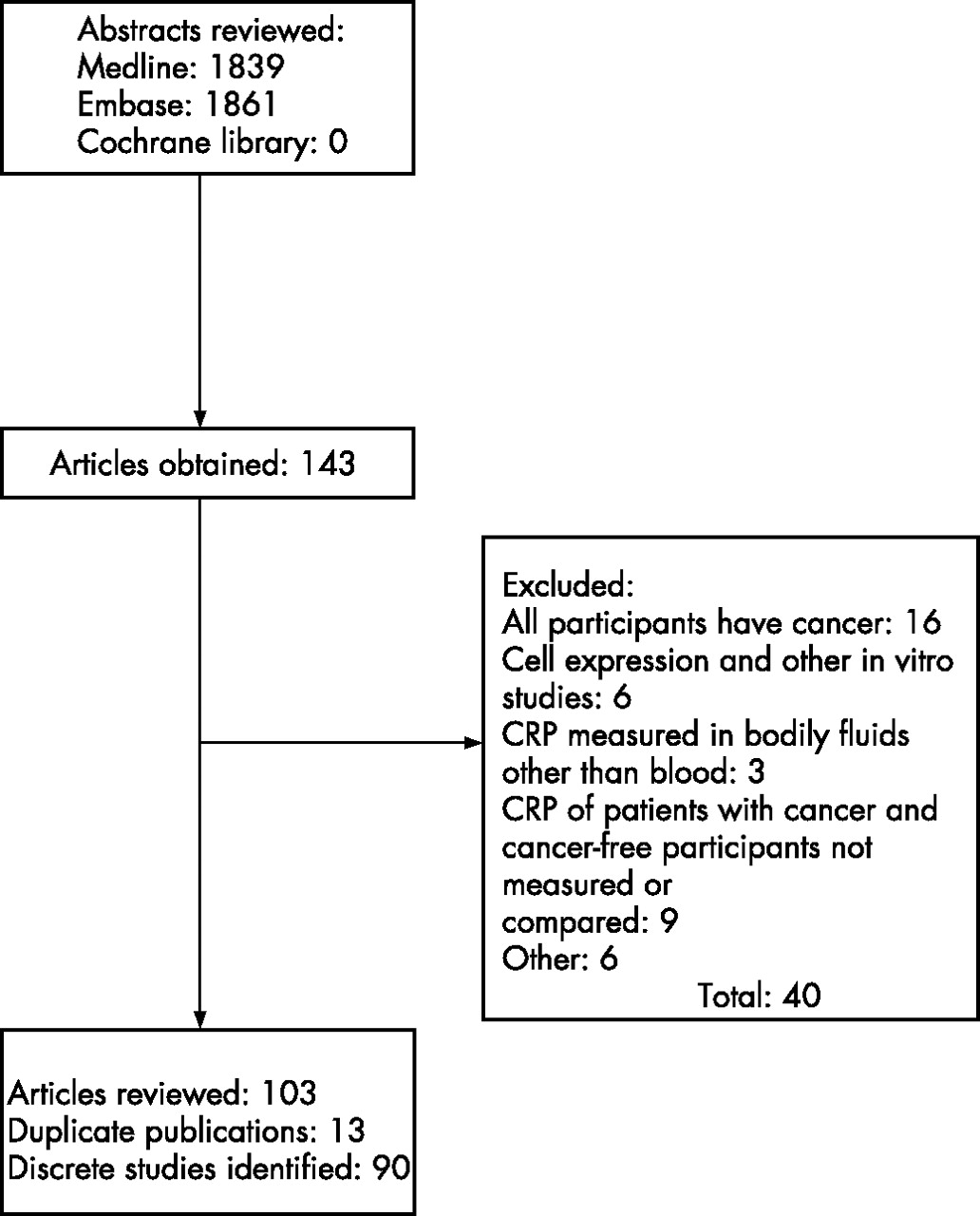
The Medline search produced 1839 hits and the Embase search produced 1861 hits. No relevant publications were identified in the Cochrane Library. A total of 103 publications that fulfilled our inclusion criteria were identified; 40 publications did not contain relevant data and were excluded (fig 1). There were 13 duplicate publications among studies investigating CRP and other biochemical markers in patients with multiple myeloma, colorectal and lung cancer: of the 9 publications by the same group of investigators, CRP data from the same cancer cases seem to have been included in 7 publications19–25 and the controls seem to have been the same in 5 of these.19–21,23,25 Three publications on advanced lung cancer26–28 and two publications on newly diagnosed lung cancer,29,30 two on colorectal cancer,31,32 two on multiple myeloma33,34 and two on prostate cancer35,36 also included the same participants. One publication drew together two sets of results previously published by the same authors37 and was not treated as a discrete study. After excluding the duplicate publications, we were left with 90 discrete studies. Despite our efforts, we were unable to obtain a full-text copy of a study of bronchial carcinoma38 and were unable to translate a Polish article on various cancers in children,39 but we included the data that we were able to extract from the abstracts and tables only. Summaries of all the published papers are presented in two supplementary web tables (supplementary tables 1 and 2 are available at http://jech.bmj.com/supplemental). Examining the association between CRP and cancer was the primary aim in 54 discrete studies.8,9,28,38–89 We also identified 36 studies in which CRP was not the main focus, but which contained relevant data.10,12,23,29,32,34,36,90–117
Number of discrete studies by type of cancer

{kind=link}
C reactive protein (CRP) systematic search results.
Table 2 lists the reviewed studies that examined various forms of cancer. The most commonly studied cancers in relation to circulating CRP were colorectal cancer, various types of lung cancer, multiple myeloma and gastrointestinal cancer. There were 81 studies of prevalent cancer cases and 9 prospective studies with incident cancer cases.42,45,59,64,66,76,79,80,89 The studies comprised 78 case–control studies, 5 of which were nested in prospective cohorts and 2 in randomised controlled trials; 2 cohort studies, 1 of which was nested within a randomised controlled trial; 5 cross-sectional studies; and 5 interventional before-and-after studies (supplementary tables 1 and 2).
Limitations of studies
Design and selection of controls
As table 3 shows, most studies had a prevalent design and their results could not determine the temporal sequence of any observed association between CRP and cancer, and could be subject to survival bias, as cases of rapidly fatal cancer would be excluded. Only nine prospective studies investigated the possible aetiological role of circulating CRP in cancer.42,45,59,64,66,76,79,80,89 Most studies had important limitations in the selection of participants. In all, 41 studies did not contain an adequate description of how the participants had been selected.22,24,32,40,44,47,48,50,51,53,54,62,65,67–69,71,74,75,77,82,85–87,93,95–97,100,102–104,106,108–110,114–118 As only abstracts were available for two studies, we could not ascertain any details of the recruitment of controls for these.38,39 Of the 78 case–control studies included in our review, 12 had selected controls from hospital staff, soldiers, or blood or organ donors, who might have been healthier than the general population from which the cancer cases were obtained.8,23,27,28,40,46,52,60,78,88,90,113 In all, 22 case-control studies,9,12,29,43,51,57,58,63,70,78,81,83,88,91,92,94,98,99,101,105,107,112 2 before-and-after studies49,73 and 4 cross-sectional studies55,56,72,84 had recruited controls and participants free from cancer from hospital inpatients or outpatients who were likely to be less healthy than the general population. Only 10 case–control studies had used community controls,36,42,45,59,61,66,76,79,80,107 and 2 cohort studies64,89 and 1 cross-sectional study34 had recruited community-living participants.
Summary of results by study design
Adjustment for confounders
Few studies included adjustment for known potential confounders of the relationship between CRP and cancer, such as smoking,119,120 body mass index121 or socioeconomic position.119 It would be unreasonable to expect the researchers to adjust for confounders in studies in which the relationship between CRP and cancer is not the main focus, but in the studies in which CRP is the primary aim, lack of adjustment is a major limitation. Of the 54 studies in which CRP was the main focus, 38 had adjusted for no confounders at all,8,28,33,43,44,46–58,60–63,65,67–70,72–74,78,81–84,86–88 1 had adjusted for age only 9 and 2 for age and sex only.75,77 Only 11 studies included adjustment for age and sex as well as indicators of body mass, study site, race or other possible confounders.40,42,45,59,64,66,71,76,79,80,89 Adjustment for any potential confounders was not clear from the abstracts of the two studies that we were unable to review in full.38,39
Circulating CRP in the diagnosis and aetiology of cancer
Most of the reviewed studies had compared CRP concentrations in patients with cancer and apparently healthy controls, and 49 prevalent studies8,10,23,28,29,32,38–40,44,46,49–51,53,65,68,71,73–75,77,78,81,82,85,88,90,94–97,99,100,103,104,106–118 reported higher CRP concentrations in patients with cancer (table 3).
Forty-three prevalent studies compared CRP concentrations between patients with cancer and controls with other benign diseases (table 3). This is a useful design for determining whether increased CRP concentrations are specific to cancer, for specificity would provide evidence for their possible diagnostic or aetiological role.
Of the 34 studies comparing patients with cancer with controls with benign diseases of the same organs or organ groups,8,9,12,34,43,47,48,51,52,55–58,60–62,67,69,70,72,81,83,84,86,88,90,92,93,96,98,101,104,105,112 14 (42%) reported higher CRP concentrations in patients with cancers of the lung,56,90 pancreas,8,98 breast,12,81 ovary,83,88 oesophagus,62 liver,60 the biliary tract,48 stomach43 and multiple myeloma.34,61 However, the results of one of the breast cancer studies might have been influenced by the inclusion of healthy participants as well as those with benign diseases in the control group,12 and the analysis in the study on ovarian cancer was based on data from a small subgroup for which serum samples were available.83 In addition, three studies found higher CRP concentrations only in patients with advanced, but not with newly diagnosed, breast, gastrointestinal tract and prostate cancers when compared with controls with benign diseases.9,69,105 Several studies reported contrasting findings: six studies of multiple myeloma and cervical, prostate or lung cancers reported no difference in CRP concentrations between patients with cancer and controls with benign diseases of these organs,51,52,72,92,93,104 and a further four studies reported higher CRP concentrations in patients with benign prostate, lung, ovarian and myelogenous conditions than in patients with cancer.55,57,58,88 In one study, no sufficient data was presented for the comparison between pancreatic cancer and benign pancreatic disease.112
Of the nine studies including a control group of people with non-cancerous conditions of different organs,10,54,78,87,101,102,106,113,118 five studies only compared patients with malignant and benign diseases with healthy controls and reported no formal statistical comparison of CRP concentrations in patients with cancer and in people with other diseases. One study found higher CRP concentrations in patients with cancer-related thrombocytosis than in those with essential thrombocytosis10 and one study found increased CRP in advanced gastrointestinal cancer in comparison with controls with hernia,43 whereas two studies reported higher CRP concentrations in people with neurological conditions than in those with malignant brain tumours101 and peritoneal sepsis.87 In all, 19 studies (44% of all the studies including a control group with any benign disease) found that patients with cancer had higher CRP concentrations than participants with other non-malignant diseases (table 3).
Twenty-seven studies defined their aim as examining the value of serum CRP in the diagnosis of cancer, but only five of them presented analyses of the sensitivity and specificity of increased CRP concentrations in discriminating cancer cases from controls. In a study of hepatocellular carcinoma comparing cancer cases with patients with other liver conditions, sensitivity, specificity and diagnostic accuracy of CRP using a threshold of 5 mg/l were 78.9%, 56.0% and 34.9%, respectively.60 Another study comparing patients with hepatocellular carcinoma with healthy controls with a cut-off value of 12 μg/ml reported 82.4% sensitivity and 82.0% specificity.70 Results from two other studies suggested that CRP is useful in distinguishing patients with pancreatic cancer from healthy controls112 and people with malignant pleural effusions from those with non-malignant effusions,56 but not in differentiating between malignant and non-malignant ascites.91 A study of testicular cancer reported CRP to be highly sensitive and specific in differentiating epididymitis (in which the CRP concentrations were higher than in the malignant disease) from cancer.57 Thus, the results from the studies that presented appropriate tests of diagnostic accuracy did not provide strong evidence to support the usefulness of increased CRP in early diagnosis of cancer. However, most studies claiming to examine the role of CRP in the diagnosis of cancer did not undertake appropriate analyses (sensitivity, specificity, receiver operator characteristics or other tests of calibration or discrimination) to determine the usefulness of CRP as a diagnostic tool in cancer.
As the only observational study design that assures the temporal relationship between exposure and outcome, prospective studies provide the best level of evidence for any potential role of circulating CRP in the diagnosis or aetiology of cancer. Table 4 summarises the nine prospective studies identified in this review. The findings in these studies were conflicting and provided no strong evidence of circulating CRP being causally related to cancer in general, but there was some evidence that it could be related specifically to certain types of cancer.
Summary of prospective studies of the association between circulating CRP and cancer
Two studies found increased circulating CRP concentrations to be associated with an increased risk of any incident cancer, even after excluding the first year of follow-up to avoid possible reverse causality,45 although this association seemed stronger with deaths from cancer than non-fatal cancer events.64 However, a prospective case–control study found no association between CRP and incident cancer in general or any specific form of incident cancer.80 No association was reported in prospective studies between circulating CRP at baseline and the subsequent risk of prostate64,79 or breast64 cancers.
Evidence of an association between increased CRP and colorectal cancer is contradictory. In four prospective studies (nested in the Campaign Against Cancer and Heart Disease (CLUE II) cohort, α-Tocopherol, β-Carotene (ATBC) Trial, Health Aging and Body Composition Study and Japan Public Health Center-based Prospective study), the investigators found increased CRP concentrations to be associated with incident colorectal cancer, although the analysis in one of these was based on only 41 cancer events.42,59,64,76 Results from two of these studies showed a more prominent association in colon cancer than in rectal cancer.59,76 However, one prospective study, with 169 cancer cases, found a borderline statistically significant association between higher CRP concentrations and a reduced risk of colorectal cancer in age-adjusted multivariate models,89 and in another study with 141 cases,66 the researchers reported no association. Thus, overall, there is some evidence for a positive association between CRP and colorectal cancer.
A prospective cohort study and a prospective nested case–control study reported positive associations with incident cancer in general and incident lung cancer in particular.45,64 However, the findings for lung cancer in both these studies were based on small numbers of cancer events, 42 cancer events in the cohort study and 72 events in the case–control study. In the cohort study, the positive association remained with adjustment for pack-years of cigarette smoking in multivariate analyses, but in the case–control study, stratified analysis showed little evidence for an association with any cancer among the participants who had never smoked.
DISCUSSION
In general, patients with cancer have been shown to have higher CRP concentrations than healthy controls and participants with some benign diseases. However, too few studies provided appropriate analyses to assess the diagnostic value of circulating CRP in cancer. Moreover, most studies to date measured CRP in prevalent cancer cases, and it is therefore possible that any association between CRP and cancer reported in these studies reflects reverse causation, survival bias or confounding. Of the nine large prospective studies identified in this review, four studies reported no association between circulating CRP and breast, prostate and colorectal cancers, but five studies provided some evidence that CRP could be related to colorectal and lung cancers.
Although the results of prospective studies are less likely to be influenced by reverse causation or bias, these associations can be explained by confounding. Associations between CRP concentrations and cancer are likely to be confounded by socioeconomic and lifestyle factors, particularly smoking and body mass index.119,121 Although the prospective studies identified in this review did adjust for important confounding factors, residual confounding due to measurement error in these factors and poor modelling of their relationship with the outcome is possible.122 In particular, the strong relationship between tobacco smoking and lung cancer will make adequate adjustment for its confounding effect difficult.
One way to overcome the problem of adequate adjustment would be to examine the association of functional CRP gene variants with cancer. This approach uses the principles of Mendelian randomisation to exploit the random allocation of genes at birth.123,124 Therefore, the CRP gene variants will not be associated with socioeconomic or lifestyle factors, such as tobacco smoking, and examining the association of CRP gene polymorphisms with cancer would avoid any confounding from these factors. Although this approach has been used to determine the causal relationship of CRP with cardiovascular risk factors,125,126 we are unaware of its use with cancer outcomes. This could be partly due to the large numbers of cancer cases required for such studies in order to reach reasonable precision with binary outcomes.127
What this paper adds
-
Most prevalent studies have reported higher C reactive protein (CRP) concentrations in patients with cancer than in healthy controls and participants with some benign conditions, but this can be due to reverse causality, survival bias or confounding.
-
The small number of prospective studies in this area provided no strong evidence for a causal role of CRP in cancer.
Policy implications
-
Few studies published so far provided relevant analyses to assess the diagnostic value of circulating C reactive protein (CRP) in cancer, and the results from the small number of prospective studies are conflicting.
-
Thus, currently, there is little evidence to support the use of CRP in the early diagnosis or aetiology of cancer.
In conclusion, most of the studies attempting to evaluate the use of circulating CRP in the diagnosis of various cancers did not present relevant statistical analyses and most of the vast literature published on the association of circulating CRP with cancer has been based on studies of prevalent cancer cases, which cannot provide evidence for causality. The small number of prospective studies identified in this review did not provide strong evidence for a causal role of CRP in malignancy, although there was some evidence that CRP could be related to colorectal cancer in particular. Further prevalent studies in this area will not add to what is already known; more large prospective studies and studies examining the association of CRP functional genetic variants with cancer outcomes would be useful to determine the role of CRP in the aetiology of cancer.
Acknowledgments
KH is funded by the Medical Research Council (MRC) PhD award.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Competing interests: None declared.
Linked Articles
- In this issue