Article Text

Abstract
Background: This study examines whether insufficient ultraviolet B (UVB) irradiance, a marker of vitamin D inadequacy, might contribute to lung cancer incidence.
Methods: The association of latitude and UVB irradiance with age-adjusted incidence rates of lung cancer in 111 countries was investigated. Independent associations with UVB irradiance, cloud cover, anthropogenic aerosols, and cigarette smoking, were assessed using multiple regression.
Results: Latitude was positively related to incidence rates in men (R2 = 0.55, p<0.01) and women (R2 = 0.36, p<0.01). In men, cigarette consumption (p<0.001) was positively related to risk, whereas UVB irradiance was inversely associated (p = 0.003). There were positive associations with UVB absorbers, in particular cloud cover (p = 0.05) and aerosol optical depth (p = 0.005). The R2 for the model was 0.78 (p<0.001). UVB irradiance was also inversely associated with incidence rates in women (p = 0.0002), whereas cigarette consumption (p<0.001), total cloud cover (p = 0.02) and aerosol optical depth (p = 0.005) were positively associated. The R2 for the model was 0.77 (p<0.001).
Conclusions: Lower levels of UVB irradiance were independently associated with higher incidence rates of lung cancer in 111 countries.
Statistics from Altmetric.com
There are approximately 1 350 000 cases and 1 180 000 deaths from lung cancer worldwide per annum,1 making morbidity and mortality from this disease a serious global public health problem. Cigarette smoking is the overwhelming cause of lung cancer,2 3 although other factors may also be involved to a far more limited extent.
An ecological study in the United States by Grant4 was the first to identify an inverse association between ultraviolet B (UVB) irradiance, vitamin D status, and lung cancer mortality rates. The inverse association persisted after adjustment for multiple covariates, including ethnicity.5 Another study found a positive correlation between UVB and lung cancer survival rates in black men.6 Several studies have found substantial inverse associations between UVB or its markers and mortality from several different types of cancer,7–9 suggesting that vitamin D photosynthesis caused by UVB may be associated with a lower risk of some types of cancer. An analysis by Giovannucci and colleagues10 of the Harvard Health Professionals Follow-Up Study identified a 20% lower incidence of lung cancer per 25 nmol increase in the estimated serum 25(OH)D level, although this result did not reach statistical significance. Serum concentrations of the main vitamin D metabolite, 25(OH)D, are strongly related to UVB irradiance.11 This study investigated the associations of cigarette smoking, UVB and UVB-absorbing atmospheric factors with global incidence rates of lung cancer.
MATERIALS AND METHODS
Data sources
Age-adjusted incidence rates of lung cancer were obtained for 175 countries using the International Agency for Research on Cancer GLOBOCAN database (for annual adjusted incidence rates of cancer by country and sex for 2002 see appendix available online only ).1 GLOBOCAN uses national cancer registries and vital events registers to estimate annual age-adjusted incidence rates per 100 000 population in 175 countries; of these, cigarette consumption data for 1980–1982 were available from the World Health Organisation for 111.12 The period 1980–1982 was selected to allow for the induction period of lung cancer.13 The most recent incidence year for which complete data were available, 2002, was used for this study. The incidence rates were age-adjusted to the world standard population,1 and were analysed separately for men and women using five-year age groups. As a result of inevitable delays in reporting by countries, incidence rates in the 2002 database were for the most recent data available, which was generally 1997–2000.
A file was created that contained information for each country on solar UVB irradiance at the top of the atmosphere at the vernal equinox, anthropogenic atmospheric sulphate aerosol optical depth, total cloud cover as a proportion of sky covered, and annual per capita cigarette consumption. Data from NASA satellite instrument packages were used to obtain aerosol optical depth and total cloud cover.14 15 Anthropogenic aerosol optical depth is an index of the attenuation of radiation as it passes through the atmosphere, caused by the presence of suspended particles resulting from human activities. Non-industrial countries were categorised as not having anthropogenic sulphate aerosols. Total cloud cover was measured as the mean proportion of the sky covered by clouds at the winter solstice.15 Latitude for each country was determined by using the latitude of the population centroid. The population centroid of each country was calculated for this study by the Columbia University Center for Earth Sciences International Network. Data on per capita cigarette consumption for 1980–1982 were defined as the average annual number of cigarettes smoked by persons over the age of 15 years.12 Data on per capita cigarette consumption in 1990 were included in a sensitivity analysis.12
Data on dietary intake including total energy from plant sources, animal sources, fats, fish and alcohol intake were obtained from the United Nations Food and Agriculture Organisation.16 These variables, however, had weak or inconsistent associations with incidence rates of lung cancer, and were not included in regression models after preliminary analyses for this reason.
Data on cigarette consumption by country were not sex-specific, and therefore cigarette consumption was apportioned by sex to estimate sex-specific cigarette consumption. For men, this was done by dividing the male incidence rate of lung cancer by the sum of the male and female incidence rates for a given country, then multiplying this proportion by the per capita cigarette consumption. For women, the lung cancer incidence rate for women was divided by the sum of the male and female incidence rates with the resulting proportion multiplied by the per capita cigarette consumption. The estimated sex-specific cigarette consumption rates were used in the regressions.
Total solar irradiance at the top of the atmosphere was calculated using a standard algorithm provided by Columbia University.17 The algorithm is based on the cosine law of solar irradiance. This algorithm provided the estimated total solar irradiance at the top of the atmosphere during the 30-day period surrounding the vernal equinox (21 March in the northern hemisphere and 21 September in the southern) for the population centroid of each country.
The cosine law equation is: A′ = A * cos x. In this formula, x is the latitude of the population centroid of each country, A′ is the solar radiation for the country’s latitude at the vernal equinox, in W/m2, and A is the total solar radiation at the top of the atmosphere at the equator on the equinox.17 This product is multiplied by 0.0042 to obtain estimated UVB irradiance, which is 0.42% of total solar irradiance. To illustrate the calculations, assume a country is located at the latitude of Boston, Massachusetts, specifically 42.32°N. From many measurements, the standard value of the solar constant, A, is 1368 W/m2.18 The solar constant cannot be exceeded anywhere on earth, and all points away from the equator on the dates of the equinoxes have lower solar irradiance.
The example for the vernal equinox in Boston would be calculated as follows: A′ = 1368 W/m2* cos (42.32°) = 1368 W/m2*0.7394 = 1011 W/m2. This value is multiplied by 0.0042 to obtain the estimated UVB irradiance at the top of the atmosphere, 4.2 W/m2. A standard calculator for the solar zenith angle and its cosine is available at http://www.srrb.noaa.gov/highlights/sunrise/azel.html. As a sensitivity analysis, all calculations were repeated assuming winter and summer solstice inclinations of the earth from its plane of rotation around the sun, with essentially identical results.
Statistical analysis
The relationship between latitude and incidence rates for all 175 countries was examined, and found to be parabolic, with a vertex (low point) near the equator. An iterative procedure using all 175 data points and the cosine law relationship yielded a curve with y = (cos(x)* − 236.89) + 4.16, where y is the age-standardised incidence rate of lung cancer and x is the latitude in degrees.
Multiple regression was used to assess the relationship of total solar irradiance at the top of the atmosphere in W/m2, sulphate aerosol optical depth, and per capita cigarette consumption with lung cancer incidence rates in 111 countries. As a sensitivity analysis, the analyses were repeated after adding a variable on alcohol consumption and a variable for the change in cigarette consumption between 1970 and 1980–1982. The analyses were performed using JMP 5.1.2 (SAS Institute, Cary, North Carolina, USA).
RESULTS
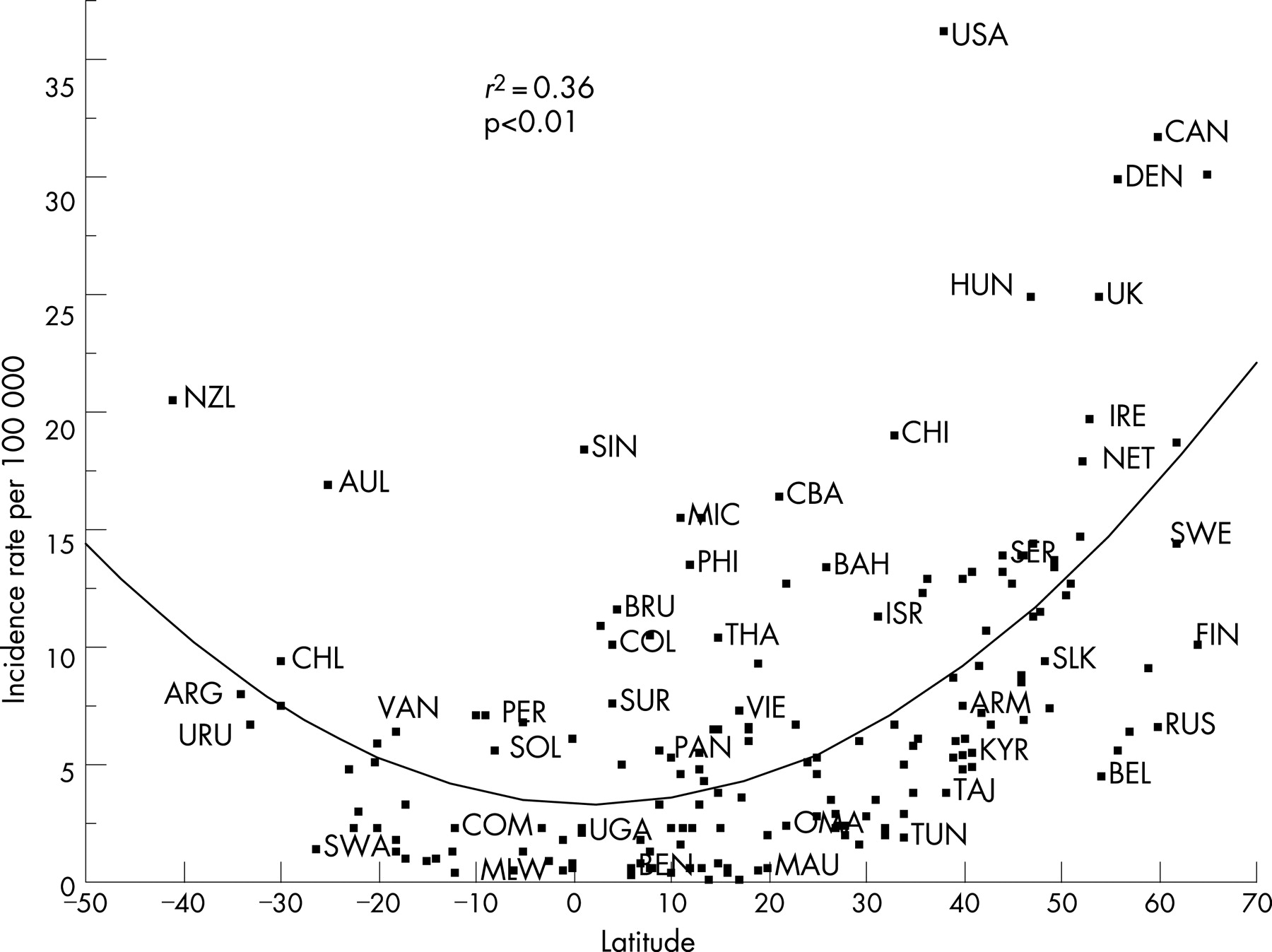
According to univariate analyses, lung cancer incidence rates increased with increasing latitude in men (coefficient of determination, R2 = 0.55, p<0.01; fig 1) and women (R2 = 0.36, p<0.01; fig 2). Univariate analyses also revealed that UVB irradiance was inversely associated with lung cancer incidence rates in men (p<0.001; table 1) and women (p<0.001; table 2).


{kind=link}
{kind=link}
According to multivariate analysis, UVB irradiance (p = 0.003) was inversely associated with lung cancer incidence rates in men, whereas total cloud cover (p = 0.05), sulphate aerosol optical depth (p = 0.005), and cigarette consumption (p<0.001) were positively associated (overall R2 = 0.78, p<0.001; table 3).
In women, UVB irradiance (p = 0.0002) was inversely associated with lung cancer incidence rates, whereas total cloud cover (p = 0.02), sulphate aerosol optical depth (p = 0.005), and cigarette consumption (p<0.0001) were positively associated (overall R2 = 0.77, p<0.0001; table 4).
In a sensitivity analysis that included a covariate for the change in cigarette consumption between 1970 and 1980–1982, UVB irradiance remained inversely associated with lung cancer incidence rates in men (p = 0.003), whereas sulphate aerosol optical depth (p = 0.002) and cigarette consumption (p<0.0001) were positively associated (overall R2 = 0.79, p<0.001; not shown). The change in the number of cigarettes consumed between 1970 and 1980–1982 was not associated with the incidence rate of lung cancer.
In a similar sensitivity analysis of women, UVB irradiance was inversely associated with lung cancer incidence rates (p = 0.0002), whereas total cloud cover (p = 0.02) and sulphate aerosol optical depth (p = 0.003) were positively associated with incidence rates (overall R2 = 0.78, p<0.001; not shown). Cigarette consumption (p<0.0001) and the change in cigarette consumption between 1970 and 1980–1982 (p = 0.01) were both positively associated with incidence rates in women.
The regression models were also computed using total, instead of sex-specific, cigarette consumption. The findings persisted in the same direction and remained statistically significant (not shown). As some previous studies19 20 reported a positive association of alcohol intake with the risk of lung cancer, models were also computed that included the intake of alcohol in 1980 as a covariate. There was a positive, although non-significant, independent association of alcohol intake with incidence rates of lung cancer in men, but not in women. The inverse association of UVB (p = 0.02 in men, p = 0.002 in women) and the positive association of atmospheric aerosol (p = 0.01 in men) and cigarette consumption (p⩽0.001 in both sexes) persisted in the model that included alcohol intake. The association with cloud cover remained positive (p = 0.03) in women, but was borderline (p = 0.09) in men. Alcohol intake was not included in the final model because its association with lung cancer was not statistically significant.
DISCUSSION
Smoking is by far the most important cause of lung cancer,2 3 and the population-attributable risk of lung cancer from smoking is in the range of 75–85%.21 Lung cancer occasionally occurs in non-smokers, possibly as a result of exposure to secondhand smoke, radon, occupational carcinogens, and air pollution.22 This analysis investigated the role that vitamin D status may play in the remaining 15–25% of lung cancer incidence not accounted for by cigarette smoking.
Previous studies have found an association between UVB and lung cancer incidence in the United States.4 5 A survival study found that patients who had surgery for lung cancer during the summer and had the highest oral vitamin D intake, had substantially better survival than patients who had surgery during the winter and who had the lowest oral vitamin D intake.23 Another study independently observed better survival in lung cancer cases diagnosed during the summer months.24
The principal source of vitamin D is from solar UVB irradiance, which increases with increasing proximity to the equator.25 Lung cancer incidence rates in men (R2 = 0.55, p<0.01; fig 1) and women (R2 = 0.36, p<0.01; fig 2) were highest in countries at the latitudes most distant from the equator, a finding borne out by multiple regression analyses of the association of UVB irradiance with the incidence of lung cancer that controlled for cigarette consumption and other factors.
The approximately parabolic latitudinal distribution of incidence rates of lung cancer (fig 1 and fig 2) conforms to the theoretical distribution of any disease that is inversely related to solar irradiance.26 The curve represents the cosine law,26 which states that daily solar irradiance is directly proportional to the cosine of the solar zenith angle, in particular the vertical angle between the zenith and the sun at solar noon. The latitude and solar zenith angle at solar noon are identical on the equinoxes (21 March and 21 September).
This study had several strengths. The regression model was able to explain 78% of the variation in lung cancer incidence rates in men and 77% in women. The coefficient of determination for lung cancer was higher than was previously observed for colon (R2 = 0.61, p<0.0001),27 breast (R2 = 0.55, p<0.0001),27 and ovarian (R2 = 0.60, p<0.0001)28 cancers that were previously analysed using similar regression methods.
Multiple regression allowed an assessment of the independent contributions of regional UVB irradiance, cloud cover, anthropogenic aerosol optical depth, and per capita cigarette consumption to the incidence rates of lung cancer. Per capita cigarette consumption had the strongest positive correlation with incidence rates, whereas UVB irradiance was inversely correlated with incidence rates. Consistent with this finding, total cloud cover and anthropogenic aerosol optical depth, both atmospheric factors that attenuate UVB irradiance, were positively correlated with incidence rates. Stratospheric ozone also substantially reduces UVB irradiance,29 but it is more uniformly distributed over inhabited land areas than clouds15 and aerosols.14
The possibility that the incidence rates of lung cancer might not have had a chance to reflect the expanding epidemic of cigarette smoking30–32 was addressed in a sensitivity analysis that included an additional covariate for the change in cigarette consumption between 1970 and 1980–1982. The inverse association of UVB incidence with the incidence rates of lung cancer persisted after taking the change in cigarette intake into account.
Several mechanisms are involved in vitamin D anticarcinogenesis, a multistep sequence that includes translocation of intercellular adhesion proteins to the cell membrane, increased differentiation, reduced mobility and opportunities for natural selection, inhibition of tumour angiogenesis, increased apoptosis, and heterologous contact inhibition of tumour growth by adjacent normal epithelial cells.33 Vitamin D metabolites induce the differentiation of cancer cells, including lung cancer cells,34 in tissue culture, and arrest their growth by mitotic arrest in the interphase (G0/G1) phase of the mitotic cycle. 1,25(OH)2D enhances the apoptosis of epithelial cells in tissue culture by decreasing phospho-Erk and phospho-Akt, kinases that regulate apoptosis, pathways upregulating MEKK-1, a pro-apoptotic signaling molecule.35
What this paper adds:
Previous research suggested that low levels of UVB exposure are associated with a higher than expected risk of lung cancer. This study examined incidence rates of lung cancer in 111 countries according to the UVB level, while controlling for cigarette smoking and other factors. Lower levels of UVB were associated with higher incidence rates of lung cancer. This inverse association persisted after adjustment for cigarette smoking and other variables. The likely mechanism involves higher levels of serum vitamin D metabolites in individuals as a result of exposure to solar UVB. Although cigarette smoking is the main cause of lung cancer, greater UVB exposure may reduce the incidence of the disease.
Recent studies of the human tumour suppressor oncogene, p53,36 and its murine analogue, p63,37 have shown that their gene products induce the synthesis of vitamin D receptor, a molecule that may mediate the actions of vitamin D on intercellular adhesion. Consistent with this, the concentration of CYP24, an enzyme that deactivates 1,25(OH)2D, is higher in lung cancer cells than in normal lung epithelium.38
This was a study of aggregates rather than individual subjects. It is well known that findings that apply to aggregates may not apply to individuals. For example, all individuals living in areas of high UVB irradiance may not have high exposure to UVB. This can result from urbanisation and industrialisation. On the other hand, regional solar UVB irradiance is often likely to affect a broad range of individuals, and the finding was present despite the possible misclassification of exposure. Non-differential misclassification of exposure generally obscures associations, rather than creating them.39
Ecological studies should be considered as hypothesis generating, rather than definitive. Such studies are potentially the source of variables to be investigated using other methods. On the other hand, the diverse geographical distribution of populations in areas with different levels of UVB irradiance provides a natural experiment on a large scale. Natural experiments are sometimes of value in identifying relevant factors for a disease. For example, ecological comparisons of areas with high fluoride concentrations in drinking water with areas with low fluoride concentrations showed that fluoridation could markedly reduce the incidence of dental caries.40
Ecological studies cannot account for all possible confounders. For example, this study did not control for differences in physical activity or diet among the populations of different countries. There is, however, no evidence supporting an independent association of low physical activity, or particular foods, with lung cancer, and the effects of these or other factors are not mutually exclusive of favourable associations of UVB and vitamin D status with the incidence of lung cancer. Lung cancer incidence varies mainly with cigarette consumption, rather than socioeconomic status, so it was not necessary to adjust for socioeconomic status because cigarette consumption was included in the regression models. In addition, the data available for this research did not include possible confounders such as occupational exposures, low lung function, or the prevalence of lung diseases.
Many of these limitations could be addressed by observational studies of individuals, because such studies can more definitively examine hypotheses generated from natural experiments. Whereas cigarette use had the strongest association with lung cancer incidence rates (p<0.0001), UVB irradiance was also modestly inversely associated with incidence rates (p<0.001), although other unmeasured confounders might play some role. Further epidemiological studies of the effect of serum 25(OH)D levels and the oral intake of vitamin D on lung cancer risk are needed, holding cigarette consumption constant.
Acknowledgments
The authors express warm thanks to Drs Jacques Ferlay, Paola Pisani, Donald M. Parkin and Mr Freddie Bray of the International Agency on Research on Cancer, Lyon, France, for providing cancer incidence data from the GLOBOCAN database.
REFERENCES
Footnotes
Competing interests: None declared.
Funding: This research was supported by a congressional allocation to the Penn State Cancer Institute of the Milton S. Hershey Cancer Center, Hershey, Pennsylvania, USA, through the Department of the Navy, Bureau of Medicine and Surgery, under work unit no. 60126.
The views expressed in this report are those of the authors and do not represent an official position of the Department of the Navy, Department of Defense, or the US Government.
Linked Articles
- In this issue