Article Text

Abstract
Background: Although there is evidence that vitamin D inadequacy may be linked to adverse cognitive outcomes, results from studies on this topic have been inconsistent. The aim of this trial was to examine the association between 25-hydroxyvitamin D (25(OH)D) levels and cognitive performance in middle-aged and older European men.
Methods: This population-based cross-sectional study included 3,369 men aged 40–79 years from eight centres enrolled in the European Male Ageing Study. Cognitive function was assessed using the Rey–Osterrieth Complex Figure (ROCF) test, the Camden Topographical Recognition Memory (CTRM) test and the Digit Symbol Substitution Test (DSST). Serum 25(OH)D levels were measured by radioimmunoassay. Additional assessments included measurement of physical activity, functional performance and mood/depression. Associations between cognitive function and 25(OH)D levels were explored using locally weighted and linear regression models.
Results: In total, 3,133 men (mean (±SD) age 60±11 years) were included in the analysis. The mean (±SD) 25(OH)D concentration was 63±31 nmol/l. In age-adjusted linear regressions, high levels of 25(OH)D were associated with high scores on the copy component of the ROCF test (β per 10 nmol/l = 0.096; 95% CI 0.049 to 0.144), the CTRM test (β per 10 nmol/l = 0.075; 95% CI 0.026 to 0.124) and the DSST (β per 10 nmol/l = 0.318; 95% CI 0.235 to 0.401). After adjusting for additional confounders, 25(OH)D levels were associated with only score on the DSST (β per 10 nmol/l = 0.152; 95% CI 0.051 to 0.253). Locally weighted and spline regressions suggested the relationship between 25(OH)D concentration and cognitive function was most pronounced at 25(OH)D concentrations below 35 nmol/l.
Conclusion: In this study, lower 25(OH)D levels were associated with poorer performance on the DSST. Further research is warranted to determine whether vitamin D sufficiency might have a role in preserving cognitive function in older adults.
Statistics from Altmetric.com
The essential role of vitamin D in maintaining bone health and regulating calcium metabolism has long been recognized.1 A growing body of research has revealed, however, that the vitamin D endocrine system is associated with a broad range of physiological outcomes besides systemic calcium homeostasis.2 Although there are some data to suggest that vitamin D deficiency may have adverse effects on cognition or behaviour,3 4 there is currently insufficient evidence to draw definitive conclusions. Disagreement remains as to what actual threshold levels of 25-hydroxyvitamin D (25(OH)D) best describe either deficient or suboptimum status. According to currently recommended levels, vitamin D ‘inadequacy’ has been reported to be highly prevalent.5
Vitamin D is a fat-soluble secosteroid that is primarily synthesised in the skin from 7-dehydrocholesterol following solar UV-B exposure and derived to a lesser extent from dietary sources. Vitamin D is hydroxylated to 25(OH)D in the liver and subsequently to the main active molecule, 1,25-dihydroxyvitamin D (1,25(OH)2D), principally in the kidneys.6 Serum 25(OH)D levels are typically measured to establish the vitamin D status of an individual. 1,25(OH)2D exerts its biological effects both via the nuclear vitamin D receptor, thereby modulating the expression of numerous target genes, and through binding to cell membrane receptors, initiating rapid non-genomic intracellular signalling.3 The nuclear vitamin D receptor has been found in key areas of the brain known to regulate behaviour—for example, the cortex, cerebellum and limbic system—and is often co-localised in cells with 1α-hydroxylase, the final enzyme in the vitamin D activation pathway.7 In vitro experiments have demonstrated that vitamin D has both neurotrophic and neuroprotective properties,8 9 whereas long-term 1,25(OH)2D supplementation has been shown to retard hippocampal ageing in rats.10 Together, such findings suggest that the active form of vitamin D may function as a neurosteroid.
Although the positive influence of vitamin D on brain function is biologically plausible, there have been few studies exploring the association between vitamin D status and adult cognitive function. Two recent clinic-based observational studies reported that low serum 25(OH)D levels were associated with poor cognitive test performance among patients with mild Alzheimer disease,11 12 whereas a retrospective study of older adults attending a memory assessment clinic found a positive correlation between 25(OH)D levels and scores on the Mini Mental State Examination.13 Conversely, a cross-sectional analysis of a sub-sample of participants with secondary hyperparathyroidism in the Tromsø study14 reported no association between 25(OH)D levels and performance in a battery of 14 neuropsychological tests. Overall, the findings of these studies cannot be generalised to community-dwelling individuals, and the studies were limited by small sample sizes and failure to adjust for multiple confounders. To the best of our knowledge, there has been only one large community-based study that has examined the association between vitamin D and cognitive function. McGrath et al.15 analysed survey data from the Third National Health and Nutrition Examination Survey (NHANES III) and found no evidence of an association between low 25(OH)D levels and impaired neurocognitive performance. This study used different cognitive tests for different age groups, however, and failed to adjust for potential confounders, such as education and depression.
We used baseline data from the European Male Ageing Study (EMAS), an ongoing large population-based study of ageing in middle-aged and older men, to evaluate the association between vitamin D levels and cognition. In addition to standardised measurements of cognitive function, EMAS includes comprehensive lifestyle and functional assessments. The availability of this data meant we could adjust our analyses for a wide range of possible confounders of the association between vitamin D and cognition.
METHODS
Patients
The major aims of EMAS are to examine the nature, prevalence and incidence of symptoms associated with physiological ageing, exploring their relationships with endocrine functions and other risk variables. There are two phases: a cross-sectional survey of a random population sample of middle-aged and older men, which was completed in 2005, and a follow-up assessment, which is scheduled for completion in 2009. Details regarding recruitment, response rates and assessments in EMAS have been described previously.16 Briefly, noninstitutionalised men aged 40–79 years were recruited from municipal or population registers in eight centres based in the following cities: Florence, Italy; Leuven, Belgium; Lodz, Poland; Malmö, Sweden; Manchester, UK; Santiago de Compostela, Spain; Szeged, Hungary; Tartu, Estonia. For the baseline survey, stratified random sampling was used with the aim of recruiting equal numbers of men into each of four age bands (40–49 years, 50–59 years, 60–69 years and 70–79 years). Participants were invited by letter to complete a short postal questionnaire and to attend for screening at a local clinic. The study was funded by the European Union and ethical approval for the study was obtained in accordance with local institutional requirements in each centre.
Assessments
The short postal questionnaire included items concerning demographic, health and lifestyle information. Participants were asked about tobacco use (response set: current smoker, past smoker or nonsmoker), typical alcohol consumption during the preceding month (response set: every day, 5–6 days per week, 3–4 days per week, 1–2 days per week, less than once per week or not at all), and the age they left full-time education. Those who agreed to take part subsequently attended a research clinic to complete an interviewer-assisted questionnaire and assessment of cognitive function (see below). The interviewer-assisted questionnaire included the Physical Activity Scale for the Elderly (PASE)17 and the 21-item Beck Depression Inventory (BDI) to assess the presence and severity of depressive symptoms.18 In addition, physical function was assessed during the clinic visit using Reuben’s Physical Performance Test (PPT).19 Height and weight were measured using standardised instruments.
Measurement of serum 25-hydroxyvitamin D
Morning phlebotomy was performed before 10 am to obtain a fasting blood sample from all participants. Processed serum was stored at −80°C prior to analysis and shipped on dry-ice to a single laboratory (University of Leuven) for measurement of 25(OH)D levels. Serum 25(OH)D levels were determined using a radioimmunoassay kit (RIA kit; DiaSorin, Stillwater, MN, USA). Intra-assay and inter-assay coefficients of variation for 25(OH)D levels were 11% and 9%, respectively. The detection limit of the RIA kit was 3.7 nmol/l 25(OH)D.
Tests of cognitive function
To assess cognitive function, participants were asked to complete a battery of three neuropsychological tests: the Rey–Osterrieth Complex Figure (ROCF) test, the Camden Topographical Recognition Memory (CTRM) test and the Digit-Symbol Substitution Test (DSST). These tests assess the domains of visuo-constructional ability, memory, recognition, and speed of information processing, and were selected on the basis that they could be standardised across centres independent of culture and language.
Copying and delayed reproduction of the ROCF were used as measures of visual perceptual abilities and visual memory.19 The scoring criteria used were based upon Osterrieth’s original test procedure, which defines 18 units of the drawing and assigns point values of 0 to 2 to each unit dependent upon the degree to which the units are correctly drawn and placed. Each element of the ROCF test had a maximum score of 36. The CTRM test, developed to measure the recognition component of visual memory retrieval, taps into the cortical component of visual memory.21 The CTRM test involves the presentation of 30 coloured photographs of outdoor topographical scenes, each shown for 3 seconds, followed by a three-way forced recognition component. The CTRM test had a maximum score of 30. The DSST is a subtest adopted from the Wechsler Adult Intelligence Scales and provides a reliable measure of psychomotor speed and visual scanning.22 Participants were asked to make as many correct symbol-for-digit substitutions as possible within a 1 minute period.
Analysis
Analyses were undertaken using the statistical package Intercooled Stata version 9.2 (StataCorp, College Station, TX, USA). Participants with missing cognitive and/or 25(OH)D data were excluded from the analysis. Age (years), age leaving education (years) and body mass index (BMI; kg/m2) were analysed as continuous variables. The BDI score was treated as both a continuous variable and a categorical variable, with the latter based upon Beck’s original cut-off scores.18 PASE and PPT scores were treated as continuous variables and also categorised into tertiles. 25(OH)D level was examined as a continuous variable and classified into suboptimum (50–75 nmol/l), insufficient (25–49 nmol/l) and deficient (<25 nmol/l) groups broadly based on previously recommended cut-off points.23 24
The relationship between 25(OH)D level and cognitive function was initially evaluated graphically (while simultaneously adjusting for age) using the LOcally WEighted Scatterplot Smoothing (LOWESS) technique.25 This approach, where linear regression is applied repeatedly to sequential small sections of the covariate–outcome relationship, is primarily exploratory. By reducing the influence of outliers, this technique provides a smooth fit to the data so that relationships and thresholds can be more readily identified. The associations between cognitive test scores and factors that could potentially confound the relationship between cognitive function and 25(OH)D concentration were explored using linear regression, with adjustments made for age. Multiple linear regression models were then used to examine the association between 25(OH)D levels and cognitive function, with the cognitive test scores as dependent variables. Adjustments were made for factors that showed a significant association (P<0.05) with 25(OH)D status and cognitive function in age-adjusted models. Regression models were additionally adjusted for centre and season of the year (winter (Jan–March), spring (April–June), summer (July–Sept), autumn (Oct–Dec)) to account for the effects of the seasons on 25(OH)D levels. Effect modification by age was also assessed by inclusion of interaction terms between 25(OH)D concentration and age (by decade) in the regression models.
To further explore the relationship between cognitive function and 25(OH)D levels, we used a spline or piecewise regression approach whereby the model fits linear segments to different ranges of the data. Breakpoints, the level of 25(OH)D where the slope of the linear function changes, were estimated from the LOWESS plots. The mkspline function within Stata allows the regression function to be continuous at all points, including the breakpoint. All regression results are expressed as β coefficients and 95% confidence intervals (CI).
RESULTS
A total of 138 participants with missing vitamin D data (16 missing blood samples and 122 assay failures) and 98 participants with incomplete cognitive data were excluded from this analysis. The baseline characteristics of the remaining 3,133 men are shown in table 1.
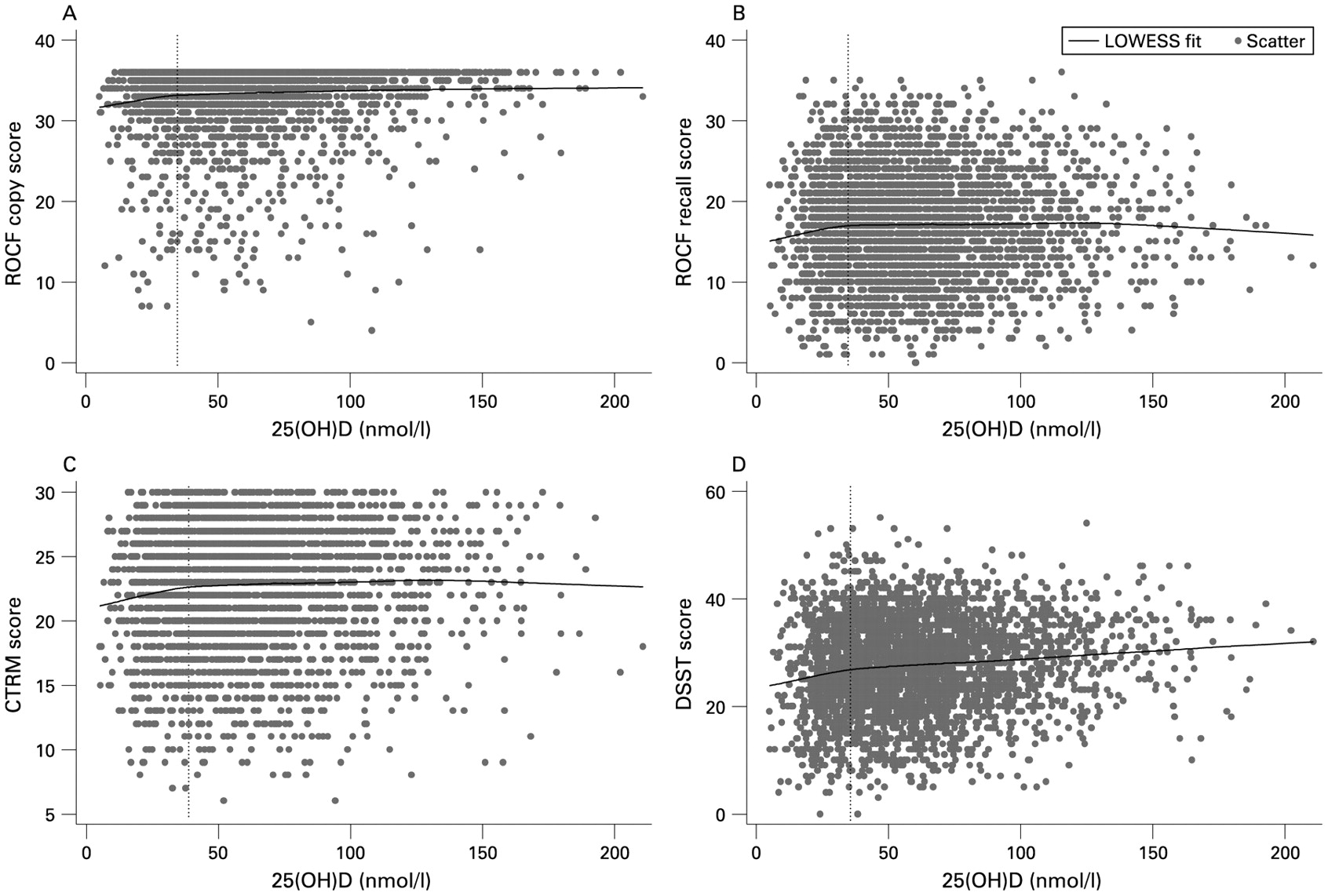
The results from the LOWESS analyses exploring the association between 25(OH)D levels and cognitive performance (while adjusting for age) are shown in Figure 1. Only the LOWESS plot of 25(OH)D level versus the DSST score was suggestive of an overall positive association (Figure 1D). At 25(OH)D levels of approximately 35 nmol/l and under, however, a more pronounced positive relationship between 25(OH)D and all four cognitive test scores was apparent.
{kind=link}
Relationship between 25(OH)D concentration and cognitive function: LOWESS plots adjusted for age. The vertical dotted line represents the estimated 25(OH)D level at which the slope of the vitamin D–cognition relationship changes. (A) Rey–Osterrieth Complex Figure (ROCF) copy score. (B) ROCF recall score. (C) Camden Topographical Recognition Memory (CTMM) test. (D) Digit Symbol Substitution Test (DSST). 25(OH)D, 25-hydroxyvitamin D; LOWESS, LOcally WEighted Scatterplot Smoothing.
Table 2 summarises the influence of factors that could potentially confound the relationship between 25(OH)D levels and cognitive function. There were significant cross-sectional age-related decreases in scores across all four cognitive test scores, but there was no association between 25(OH)D and age (β −0.0135; 95% CI −0.114 to 0.087). Depression (BDI), BMI, physical activity (PASE), physical performance (PPT) and smoking were all consistently associated with both cognitive test scores and 25(OH)D concentrations. CTRM test and DSST scores, together with 25(OH)D levels, were additionally associated with drinking one or more alcoholic drink per week. As expected, 25(OH)D levels varied markedly by season of measurement, peaking in the summer (mean 85.0 nmol/l) with a nadir in the winter (mean 49.7 nmol/l). Mean serum 25(OH)D levels also varied significantly by geographical region (one-way ANOVA, P<0.001), with highest levels observed in centres in northern and western Europe (72.6 nmol/l), lower levels in southern Europe (60.5 nmol/l), and the lowest levels in eastern Europe (53.9 nmol/l).
The results from the regression models exploring the association between 25(OH)D levels and cognition are summarised in table 3. In age adjusted linear regressions, higher 25(OH)D levels were associated with higher scores in the ROCF copy score (β per 10 nmol/l = 0.096; 95% CI 0.049 to 0.144), the CTRM test (β per 10 nmol/l = 0.075; 95% CI 0.026 to 0.124), and the DSST (β per 10 nmol/l = 0.318; 95% CI 0.235 to 0.401). After additional adjustments for age left education, depression, BMI, physical activity, physical performance, smoking, alcohol consumption, season and centre, higher 25(OH)D concentrations were found to be associated with only higher DSST scores (β per 10 nmol/l = 0.152; 95% CI 0.051 to 0.253). No association was observed between 25(OH)D levels and scores on the ROCF copy score, the ROCF recall score, and the CTRM test in fully adjusted models. The association between higher 25(OH)D levels and higher DSST scores was also observed when 25(OH)D levels were classified into suboptimum (50–74.9 nmol/l), insufficient (25–49 nmol/l) and deficient (<25 nmol/l) groups. When participants who reported taking any form of vitamin D or calcium supplements were excluded from the regression analyses, the results remained the same (data not shown). Excluding the season and centre covariates from the regression analyses did not significantly affect the results (DSST: β per 10 nmol/l 0.126; 95% CI 0.043 to 0.209). The ROCF copy score was left skewed; however, linear regression performs well in very non-normal data if the sample size is moderately large (n>500).25 Nevertheless, to verify the results of the linear regression models we inverted the ROCF copy scores and considered them as count data. The transformed data followed a negative binomial distribution (variance larger than the mean, data overdispersed). We then carried out a negative binomial regression analysis using the same covariates as in the linear model and found the same result—no evidence of an independent association between the ROCF test copy component score and 25(OH)D levels (data not shown).
Additional regression models demonstrated a significant age by 25(OH)D interaction effect with DSST as the outcome (pinteraction = 0.01). In fully adjusted linear regressions stratified by age decade with 25(OH)D level as a continuous variable, higher DSST scores were found to be associated with 25(OH)D level only among older men (β per 10 nmol/l 0.258, 95% CI 0.135 to 0.381 (60–69 years); β per 10 nmol/l 0.215, 95% CI 0.105 to 0.326 (over 70 years)) and not among younger men (β per 10 nmol/l 0.044, 95% CI −0.153 to 0.242 (40–49 years); β per 10 nmol/l 0.097, 95% CI −0.124 to 0.317 (50–59 years)). There were no age by 25(OH)D concentration interactions for ROCF test copy component scores (pinteraction = 0.5), ROCF test recall component scores (pinteraction = 0.7) and CTRM test scores (pinteraction = 0.3), nor evidence of any significant season by 25(OH)D levels, centre by 25(OH)D levels, or season by physical activity interaction effects for any of the four cognitive outcomes (data not shown).
The LOWESS plots (fig 1) suggested that the relationship between 25(OH)D levels and the four cognitive outcomes may not be best explored by a single linear function and that the slope of the relationships changed at around 30–40 nmol/l 25(OH)D. We used spline regression models, therefore, to better describe the 25(OH)D level–cognitive function relationship (table 4). The breakpoint at which the slope of the linear relationship was allowed to change was estimated to be 35 nmol/l 25(OH)D. Spline models adjusted only for age confirmed that the strength of the association between 25(OH)D levels and cognitive function (as assessed by the relative magnitude of the β coefficients) was greater at 25(OH)D levels 35 nmol/l or less as compared to higher levels. Although the same pattern was evident in spline models adjusted for age and the other covariates, none of the β coefficients reached statistical significance.
DISCUSSION
In this population-based study of European men aged 40 years or older we observed a significant, independent association between a slower information processing speed (as assessed by the DSST) and lower levels of 25(OH)D This association appeared strongest among men with a 25(OH)D level of less than ∼35 nmol/l.
Previous studies exploring the relationship between vitamin D and cognitive performance in adults have produced inconsistent findings, with only one other large population-based study having specifically examined the relationship between vitamin D and cognition in community-dwelling individuals. Using data from NHANES III, McGrath et al.15 found that serum 25(OH)D levels were not associated with neurocognitive performance in adults. One of the neuropsychological tests McGrath and co-workers used (the Symbol Digit Substitution test) assesses broadly the same cognitive domain as the DSST; that is, speed of information processing. Their study included both men and women, however, and the age range of the group assessed using the Symbol Digit Substitution test was significantly younger (20–59 years) than that of our sample. McGrath et al. did observe an association between vitamin D status and learning and memory tasks in their oldest group (60–90 years),15 but presented no data on speed of information processing in this group. Interestingly, when we stratified our regression analyses by age decade the association between increased 25(OH)D concentration and a higher DSST score was only significant among the older men; that is, those aged 60–69 years and those aged 70–79 years. Although the lack of an association between 25(OH)D level and DSST score among men under 60 years of age may have been due to insufficient power in the stratified analyses, it is intriguing to speculate that any ‘potential’ beneficial effect of 25(OH)D on psychomotor processing speed may be more pronounced in older men.
It was notable that the only significant association in fully adjusted regression models was that observed between 25(OH)D levels and DSST scores. Although we are unable to specifically explain this observation, the DSST appears robust to ceiling effects, unlike the ROCF copy score and, to a lesser extent, the CTRM test. This characteristic of the DSST may in part have enhanced the sensitivity of the test at upper levels in our cognitively intact, generally healthy sample. Further exploration of potential differential relationships across cognitive domains would require more sensitive and more exhaustive neuropsychological test batteries than our study schedule allowed.
Although experiments in animals models and in vitro studies point to the biological plausibility of low 25(OH)D levels resulting in impaired cognitive performance, the mechanisms by which vitamin D affects adult cerebral functions remain unknown. Possible positive effects could be direct, as suggested by the observation that 1,25(OH)2D treatment increases choline acetyltransferase activity in rat brain nuclei,27 or could operate via a neuroprotective pathway, as demonstrated by the stimulation of neurotrophin production28 and modulation of neuronal Ca2+ homeostasis9 by vitamin D. It is also plausible that additional factors not included in this analysis, such as parathyroid hormone and calcium levels, may be involved, generating a more complex relationship between vitamin D and cognitive function. Evidence for such a relationship comes from the Tromsø health study, where a subset of participants with secondary hyperparathyroidism were found to perform less well than normal controls on cognitive tests assessing working memory capacity and speed of information processing.14 Although the Tromsø study data derives from individuals with an overt endocrine disorder, the investigators found no evidence of any independent associations between 25(OH)D levels and cognitive performance. They did observe, however, that low levels serum 25(OH)D were significantly associated with higher depression scores. The relationship between vitamin D and mood/depression has yet to be substantiated,3 although we did find an inverse association between 25(OH)D levels and the BDI score (table 2).
In the context of the cross-sectional nature of the data presented here, any association between 25(OH)D levels and cognitive function can be interpreted in a number of ways. It is possible that a low serum 25(OH)D concentration is merely a ‘risk marker’ and is mechanistically separated from the biological processes that result in declining cognitive performance in older adults. Low levels of 25(OH)D have been shown to be associated with a number of unfavourable health outcomes, including cardiovascular disease,29 increased cancer risk and mortality,30 sarcopaenia31 and diabetes.32 Cognitive impairment has been linked to cardiovascular and metabolic diseases in several population-based studies.33–35 When we additionally adjusted for self-reported cardiovascular disease and diabetes in our regression models, the associations between 25(OH)D levels and DSST scores remained unchanged (data not shown). Conversely, cognitive impairment itself may contribute to lower levels of 25(OH)D by reducing the level of outdoor physical activity undertaken and hence exposure to sunlight. Interestingly, there is increasing evidence supporting the association between vitamin D deficiency and decreased physical performance,36 although cause and effect have yet to be differentiated. This relationship raises the possibility that the positive association between 25(OH)D and psychomotor processing speed seen in our study may, in part, reflect improved physical motor speed. In an attempt to better control for this confounder in our data, we included only the score from the seven timed elements of the PPT (in place of the total score) in our regression models. The relationship between 25(OH)D level and DSST score remained unchanged, however, suggesting that the association may be more to do with neuronal processing speed than muscle/motor speed. Overall, we attempted to adjust for potential confounders in our analysis but cannot exclude the possibility that some of our findings may be due to unmeasured factors and/or residual confounding.
There remains uncertainty as to what level of vitamin D indicates a suboptimum or deficient status. There is strong evidence that 25(OH)D levels below 12.5 nmol/l can result in bone diseases such as rickets in infants and osteomalacia in adults,37 although to the best of our knowledge no previous studies have assessed cognitive function in participants with such overt hypovitaminosis D. Serum 25(OH)D concentrations above 50 nmol/l are generally defined as sufficient, although recent studies have suggested that serum 25(OH)D levels below 75 nmol/l are suboptimum for health.38 39 Nonetheless, our data showing that 8% of participants had 25(OH)D levels below 25 nmol/l (deficient) and 33% had levels between 25 nmol/l and 50 nmol/l (insufficient) broadly agrees with previous reports from Europe.5 40 In terms of any relationship between a given threshold level of 25(OH)D and reduced cognitive performance, our data suggest that cognitive function is increasingly negatively associated with 25(OH)D at levels below around 35 nmol/l. In spline regression models adjusted for age and other covariates (see Table 4), however, none of the associations between 25(OH)D concentration (either above or below 35 nmol/l) and cognitive function were statistically significant. This may in part be due to insufficient power to detect the relatively modest changes in, for example the DSST score, with varying levels of 25(OH)D.
Although we have referred to 25(OH)D throughout, vitamin D exists in two common forms; vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol). The form mainly produced in the skin and derived from natural dietary sources is vitamin D3, whereas the primary source of vitamin D2 is multivitamin preparations and some fortified foods.41 There have been conflicting reports as to whether vitamin D2 and vitamin D3 are equally effective at maintaining 25(OH)D levels,42 43 with another study suggesting that the D2 form may actually have a negative effect on 25-hydroxycholecalciferol (25(OH)D3) status.44 The immunoassay used in our study has the same reported sensitivity to both forms of 25(OH)D (data from manufacturers manual), so the reported 25(OH)D levels here are the sum of 25(OH)D2 and 25(OH)D3. As we have no information as to the relative abundance of each form within samples, we are unable to draw any conclusions as to the difference in the associations, if any, between 25(OH)D2 and cognitive function and between 25(OH)D3 and cognitive performance. Future studies in animals or in vitro may shed more light on whether or not the D2 and D3 forms of vitamin D are differentially associated with brain function and/or development.
The main strengths of our study are that it is based on a large population-based sample and used uniform methods to not only assess vitamin D status, but also potential confounders such as depressed mood, physical activity and physical function. In addition, the battery of cognitive tests was specifically selected on the basis that the tests could be standardised across different centres and applied to individual participants independent of language and culture. Methodological limitations inherent to the EMAS study have been described in detail previously,15 although a number of specific factors need to be considered in interpreting the results presented here. The overall response rate for participation in the study was 41%. Those individuals who participated may have differed to those who did not participate with respect to levels of cognitive function and vitamin D status and some caution, therefore, is needed in interpreting our data. The main findings, however, were based on an internal comparison of responders and, therefore, any selection factors were unlikely to have had any important effect on these data. Our analysis was restricted to vision-based tests of cognitive function. This protocol was used primarily to avoid language and cultural effects inherent in many text-based tests, but also due to the practical constraints of a large population-based study. Although serum 25(OH)D levels remain the accepted metric of vitamin D status, it is questionable whether the single serum 25(OH)D measurement performed in our study reflects each participant’s long-term vitamin D status. The single 25(OH)D value would be an indicator of sun exposure and dietary intake over the past few weeks rather than years, thereby increasing random measurement error. The net result of such an error would be to reduce the reported associations between 25(OH)D concentration and cognitive function toward the null rather than produce spurious associations. Finally, our results were obtained from a predominantly Caucasian European population and should be extrapolated beyond this setting with care.
In this population-based study of middle-aged and older European men, lower levels of serum 25(OH)D were significantly associated with slower psychomotor processing speed as measured by the DSST test. This relationship may be more pronounced among men with 25(OH)D levels below 35 nmol/l and in age-stratified analyses appeared to be restricted to older men. The magnitude of the association between 25(OH)D concentration and processing speed was comparatively small; however, if cognitive function could be improved by a simple intervention such as vitamin D supplementation, our results would have potentially important implications for population health. In light of our findings, and the fact that vitamin D inadequacy is common among adults, further prospective studies are warranted to determine whether vitamin D supplementation could aid in minimising ageing-related declines in specific cognitive domains.
Acknowledgments
The European Male Ageing Study is funded by the Commission of the European Communities Fifth Framework Program “Quality of Life and Management of Living Resources” Grant QLK6-CT-2001-00258. Additional support was provided by the Arthritis Research Campaign (UK). The authors wish to thank the participating patients in the eight countries, and the following the research and nursing staff for their data collection: C Pott, Manchester; E Wouters, Leuven; M Nilsson, Malmö; M del Mar Fernandez, Santiago de Compostela; M Jedrzejowska, Lodz; H-M Tabo, Tartu; A Heredi; Szeged. The authors also wish to thank C Moseley, Manchester, for data entry and project co-ordination and E Van Herck, Leuven, for performing the 25(OH)D assays. The EMAS Study Group members are based in the following cities: Florence, Italy (Gianni Forti, Luisa Petrone, Antonio Cilotti); Leuven, Belgium (Dirk Vanderschueren, Steven Boonen, Herman Borghs); Lodz, Poland (Krzysztof Kula, Jolanta Slowikowska-Hilczer, Renata Walczak-Jedrzejowska); London, UK (Ilpo Huhtaniemi); Malmö, Sweden (Aleksander Giwercman); Manchester, UK (Frederick Wu, Alan Silman, Neil Pendleton, Terence O’Neill, Joseph Finn, Philip Steer, Abdelouahid Tajar, David Lee, Stephen Pye); Santiago de Compostela, Spain (Felipe Casanueva, Mary Lage); Szeged, Hungary (Gyorgy Bartfai, Imre Földesi, Imre Fejes); Tartu, Estonia (Margus Punab, Paul Korrovitz); Turku, Finland (Min Jiang).
REFERENCES
Footnotes
Competing interests: None.