


Abstract
Background/Aim: The present research was performed to clarify the differences in circulating tumor cells (CTCs) counts between non-muscle-invasive (NMIBC) and muscle-invasive (MIBC) bladder cancer following transurethral resection of bladder tumor (TURBT). Patients and Methods: The cohort in the prospective research was categorized into the NMIBC (n=13) and the MIBC (n=13) groups. The pre- and postoperative number of CTCs was counted by the FISHMAN-R® system. Results: The difference of the number of preoperative CTCs between the NMIBC group (2.3±2.6) and MIBC group (4.8±4.2) did not reach statistical significance (p=0.08). However, there was a significantly greater increase in postoperative CTC count in the MIBC group (14.6±14.6) than in the NMIBC group (3.1±2.1, p=0.01). Conclusion: After TURBT, more carcinoma cells can be discharged from the bladder in the MIBC. Excessive deep layer resection and excessive pressure of the infusion fluid during TURBT should be avoided in patients with MIBC.
About 90% of bladder tumors are urothelial carcinomas (1). Urothelial carcinoma is divided into non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC). Transurethral resection of bladder tumor (TURBT) is the standard of care for management of urothelial carcinoma, both NMIBC and MIBC (2). However, the main purpose of TURBT is quite different in NMIBC and MIBC. That is, the main purpose of TURBT for NMIBC is radical treatment irrespective of follow-up therapy with intravesical bacillus Calmette-Guérin injection. On the other hand, the main purpose of TURBT for localized MIBC is pathological confirmation of muscle invasion for subsequent radical cystectomy (3). Thus, TURBT for localized MIBC has ordinarily been used for diagnostic purposes.
Distant metastases, e.g. of the lung or liver, have sometimes been found in the early postoperative period after radical cystectomy. In fact, 5-year survival of patients with localized MIBC after radical cystectomy was reported to be only 50% (4). The prognosis after radical cystectomy has not changed for over three decades (5). Therefore, we hypothesized that one of the causes of distant metastasis in the early postoperative period was the induction of micrometastases by TURBT. The reason that our hypothesis was generated was as follows. TURBT is a procedure in which the bladder tumor is minced with continuous infusion of irrigation fluid into the bladder. This irrigation fluid used during TURBT has the possibility of containing many cancer cells. Furthermore, the pressure of the irrigation fluid (about 50 cm H2O) ordinarily exceeds the venous pressure (3.5-9.5 cm H2O) during TURBT (3). As a result, cancer cells included in the irrigation fluid may spread into the systemic circulation through venous blood flow during TURBT.
In recent years, the presence of circulating tumor cells (CTCs) has been used as a predictive indicator of cancer prognosis in many malignancies (6-9). In addition, several reports that measured CTC counts demonstrated that invasive treatment had the possibility of expelling cancer cells into the systemic circulation (10-12). For example, Tsumura et al. observed an increase of the CTC counts after brachytherapy for prostatic carcinoma (12). In this study, whether a change of CTC count was observed in the bloodstream following TURBT for NMIBC or MIBC was determined in order to clarify the mechanism of cancer metastasis after TURBT.
Patients and Methods
Patient cohort and design of the study. This single-center, prospective cohort study included the patients for whom TURBT were performed at a university hospital between December 2018 and September 2019. The study protocol was approved by the institutional review board (IRB) at our tertiary academic center (IRB registration number: 29031). The protocol in the present study was in line with the ethical guidelines described in the Declaration of Helsinki (1975) and informed consent was sought from all the patients.

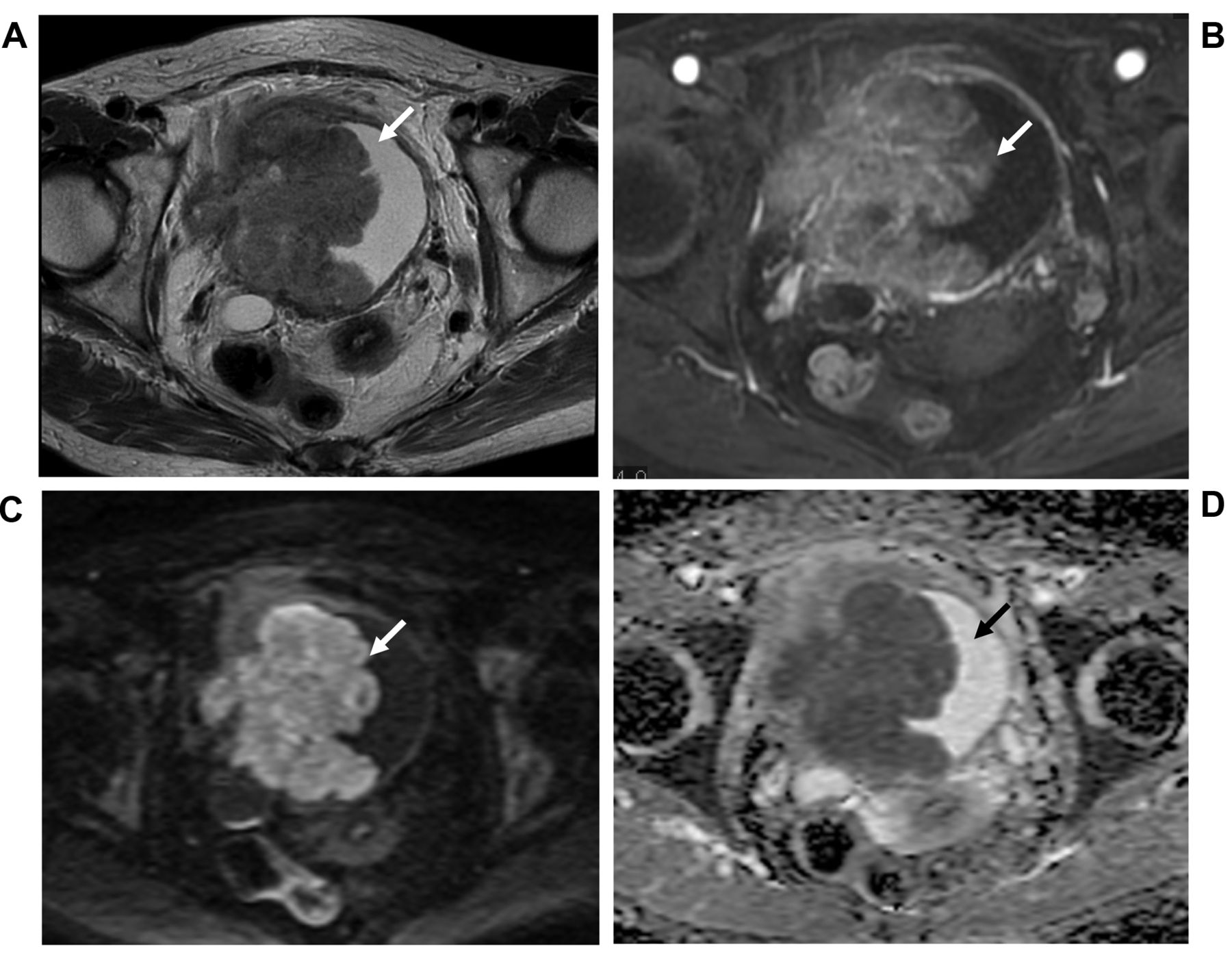
Typical multi-parametric magnetic resonance imaging in non-muscle invasive bladder cancer. A: Axial T2-weighted image shows a 1.3-cm exophytic tumor, with a sessile/broad-based tumor and a high-signal-intensity, thickened inner layer. B: Dynamic contrast-enhanced image shows early enhancement of the inner layer without early enhancement of muscularis propria. C: Diffusion-weighted image showing high-signal-intensity tumor and muscularis propria with intermediate continuous signal intensity. D: Apparent diffusion coefficient map showing a hypointense tumor. These figures suggest that a Vesical Imaging-Reporting and Data System Score of 1, which was composed of a T2-weighted imaging score of 1, dynamic contrast-enhanced imaging score of 1, and diffusion-weighted imaging score of 1, can be obtained. White and black arrows indicate the bladder tumor.
Bladder tumor was diagnosed by cystoscopy. The maximum diameter of the tumor and the number of tumors were determined based on the findings of both cystoscopy and magnetic resonance imaging (MRI). Discrimination between MIBC and NMIBC was based on the findings of multi-parametric MRI (mpMRI), which was performed using a 1.5-T whole-body magnetic resonance scanner (Signa; GE Medical Systems, Milwaukee, WI, USA) before TURBT. A 5-point Vesical Imaging-Reporting and Data System (VI-RADS) was used to identify NMIBC or MIBC in the present study (Figures 1 and 2) (13). The patients in whom the final VI-RADS score was ≥3 were categorized into the MIBC group. The value was selected because a final VI-RADS score of ≥3 was found to have a sensitivity of 87.1% and a specificity of 96.5% for muscle-invasive disease (14). The VI-RADS was scored by a blinded reviewer (H.S.), a Board-certified urologist who had diagnosed a considerable number of bladder tumors using mpMRI.
Typical multi-parametric magnetic resonance imaging in muscle-invasive bladder cancer. A: T2-Weighted image showing extension of intermediate signal intensity tumor to extravesical fat, representing invasion of the entire bladder wall. B: Dynamic contrast-enhanced image showing tumor with early enhancement that extended to the entire bladder wall and to extravesical fat. C: Diffusion-weighted image showing high-signal-intensity tumor that extends to the entire bladder wall and to extravesical fat. D: Apparent diffusion coefficient map showinq low-signal-intensity tumor that extends to the entire bladder wall and to extravesical fat. These figures suggest that a Vesical Imaging-Reporting and Data System Score of 5, which was composed of a T2-weighted imaging score of 5, dynamic contrast-enhanced imaging score of 5, and diffusion-weighted imaging score of 5, can be obtained. White and black arrows indicate the bladder tumor.
To investigate the number of preoperative and postoperative CTCs, collection of the blood from a peripheral vein was carried out before and after TURBT in the operating room. TURBT was performed under the supervision of a senior urologist (N.H.). Bladder tumors diagnosed as NMIBC were completely resected for radical cure. On the other hand, bladder tumors diagnosed as MIBC were partially resected to confirm not only the pathological diagnosis of bladder tumor, but also muscle invasion of the bladder. All procedures were performed with the Olympus transurethral resection in saline (TURis) system with a continuous flow 26-F resectoscope and U-shaped cutting loop (Olympus Medical Systems, Tokyo, Japan). The fluid bag including 0.9% saline was placed 50 cm above the bladder.
The inclusion criterion was treatment-naïve primary bladder tumor without lymph node or distant metastases. The exclusion criteria were a personal medical history of carcinoma, double or more cancer of other organs, and another carcinoma without urothelial carcinoma, e.g. squamous cell carcinoma, adenocarcinoma, after TURBT. The main outcome measures were the preoperative and postoperative CTCs counts and perioperative changes in CTCs compared between the NMIBC and MIBC groups. At the same time that CTCs were measured in the patients who underwent TURBT, the number of preoperative and postoperative CTC were also measured in five patients who underwent radical cystectomy for preliminary analyses.
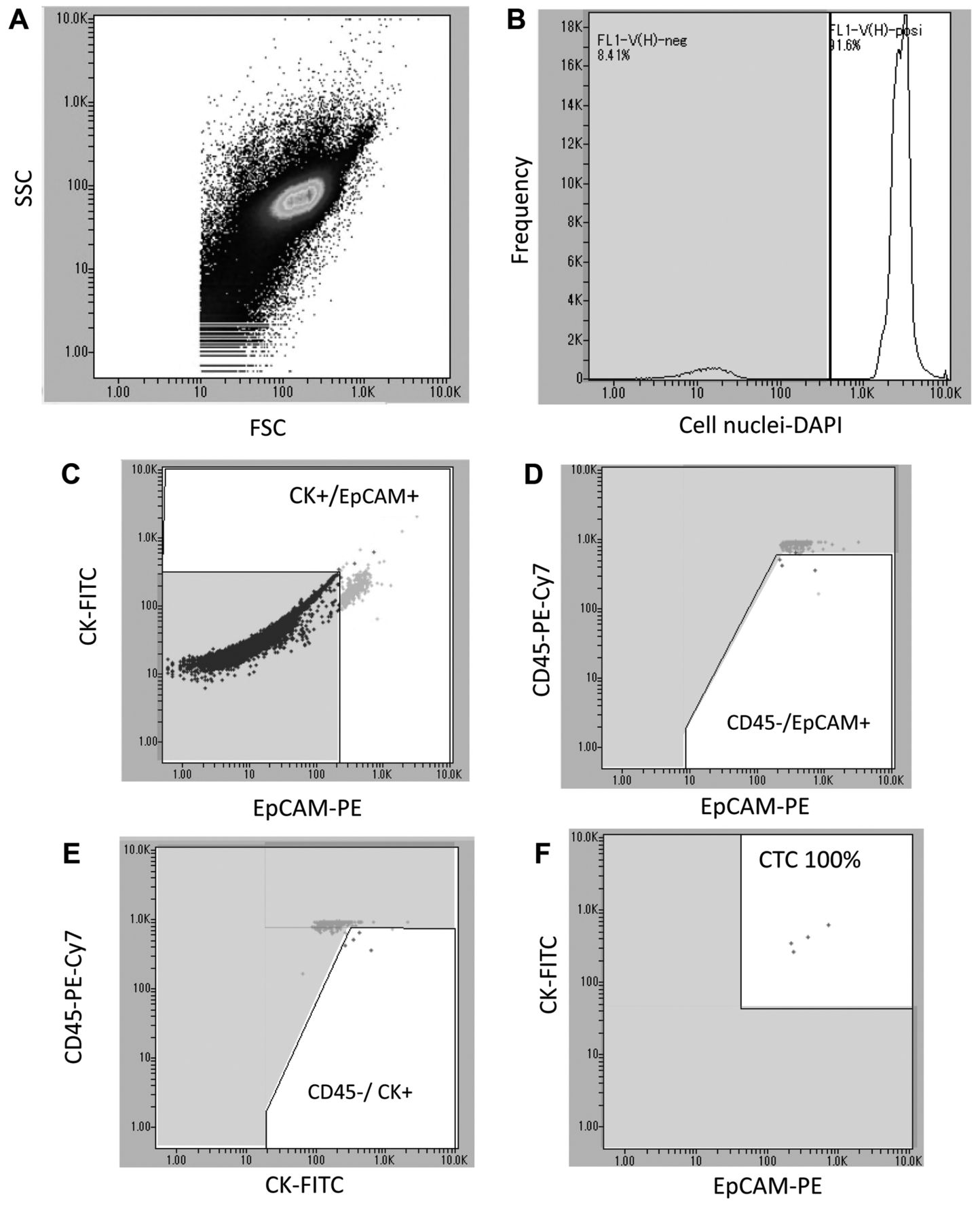
Measurement of the number of CTCs. Methods of the measurement of the CTC count used by FISHMAN-R flow cytometer (On-Chip Biotechnologies, Tokyo, Japan) has been reported by our Institution (15) (Figure 3A). Briefly, a blood sample was peripherally collected into 10-ml Cell-Free DNA BCT (Streck Inc., Omaha, NE, USA) in order to measure the number of CTC. An On-Chip pretreatment kit® was applied to carry out hemolysis, leukocyte depletion, and cell fixation, and staining for 4’,6-diamidino-2-phenylindole, fluorescein isothiocyanate, phycoerythrin (PE), and PE-Cy7 before detecting CTCs (16-19). 4’,6-Diamidino-2-phenylindole was applied to identify cell nuclei, fluorescein isothiocyanate was applied to identify cytokeratin, PE was applied to identify epithelial cell adhesion molecule (EpCAM), and PE-Cy7 was applied to identify CD45. This device consists of an expendable microfluidic chip-based flow cytometer, which promises absolute contamination-free admeasurement, whole volume admeasurement, and sample collectivity after the admeasurement. It has six channels for detection but four channels (FL1, 2, 3, and 6) were applied for counting the number of CTCs in this study. FL1 used a wavelength of 445/20 nm to detect 4’,6-diamidino-2-phenylindole (cell nuclei). FL2 used a wavelength of 543/22 nm to detect fluorescein isothiocyanate (cytokeratin). FL3 used a wavelength of 591.5/43 nm to detect PE (EpCAM). A wavelength of >710 nm for FL6 was used to detect PE-Cy7 (CD45) (Figure 3B-F). These data were analyzed using FlowJo software v7.6.5 (Tree Star, Ashland, OR, USA).

Flow cytometric detection of circulating tumor cells (CTCs) by the FISHMAN-R. CTCs are defined as cell nuclei-positive, cytokeratin (CK)-positive, epithelial cell adhesion molecule (EpCAM)-positive, and CD45-negative. After cells were detected by both forward scattered light (FSC) and side scattered light (SSC) (A), cell nuclei-positive cells were confirmed using 4’,6-diamidino-2-phenylindole (DAPI) (cell nucleus) (B). Both EpCAM-positive and CK-positive CTCs were identified using phycoerythrin (PE) against fluorescein isothiocyanate (FITC) density plots (C). EpCAM-positive cells were distinguished as CD45-negative using PE-Cy7 against PE density plots (D). CK-positive cells were distinguished as CD45-negative using PE-Cy7 against FITC density plots (E). Finally, the number of CTCs evaluated by FISHMAN-R was calculated using FlowJo software (F).
Patient characteristics and perioperative outcomes.
Statistical analysis. The differences in categorical variables between the NMIBC and MIBC groups were analyzed using the chi-squared test. Welch's t-test was applied to investigate the differences in continuous values. Simple regression analysis was used to investigate the correlations between continuous variables. Ekuseru-Toukei 2012 software (Social Survey Research Information Co., Ltd., Tokyo, Japan) was used for data analyses. Values of p<0.05 were judged as statistically significant.
Results
A total of 26 patients (13 with NMIBC and 13 with MIBC) were enrolled in the present study during the observation period. Table I demonstrates the basal characteristics of the patients and the outcomes of perioperative parameters in both the NMIBC group and MIBC group. The VI-RADS score was 1.3±0.5 in the NMIBC group and 4.1±0.9 in the MIBC group. Differences in the mean age and the ratio of males to females between the NMIBC group and the MIBC group did not reac statistical significance. Significantly greater main tumor diameter was observed in the MIBC group than in the NMIBC group (p=0.0004). Multiple tumors were significantly more common in the MIBC group than in the NMIBC group (p=0.04). Concerning perioperative parameters, there was no significant difference in the ratio between lumbar anesthesia and general anesthesia between the two groups (p=0.37). However, the operative duration (p=0.01) and the volume of irrigation fluid used during TURBT (p=0.01) were significantly greater in the MIBC group than in the NMIBC group. On pathological diagnosis, noninvasive urothelial carcinoma was not observed in the MIBC group.
Comparison of CTC counts between the two groups. Preliminary analysis of five patients who underwent radical cystectomy demonstrated that the mean number of CTCs preoperatively was 4.8±3.1, postoperatively was 2.6±2.4, and the change in the preoperative to postoperative CTC count was −2.2±3.6.
In the comparison between the NMIBC and MIBC groups, no statistically significant difference was observed with regard to the preoperative CTC counts between the two groups (NMIBC 2.3±2.6, MIBC 4.8±4.2, p=0.08) (Figure 4A). However, there was a significantly greater increase in the postoperative CTC count in the MIBC group (14.6±14.6) than in the NMIBC group (3.1±2.1, p=0.01) (Figure 4B). In addition, there was a significantly higher change in CTC counts in the MIBC group (9.7±12.1) than in the NMIBC group (0.8±2.8, p=0.02) (Figure 4C). In comparing the CTC counts before and after TURBT, no significant difference was observed in the NMIBC group (preoperative=2.3±2.6, postoperative=3.1±2.1, p=0.30). On the other hand, there was a significant increase in the MIBC group after TURBT (preoperative=4.8±4.2, postoperative=14.6±14.6, p=0.01).
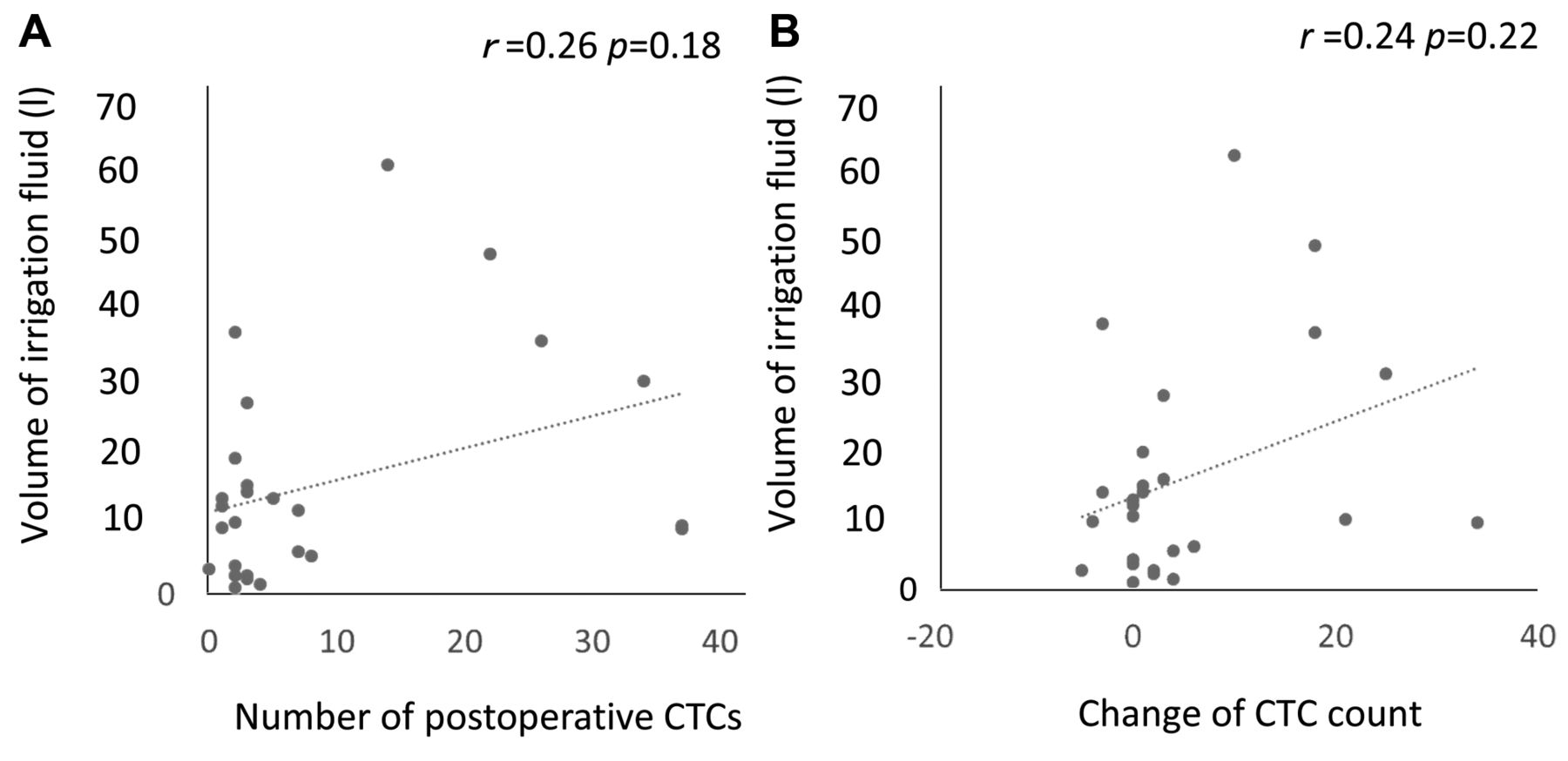
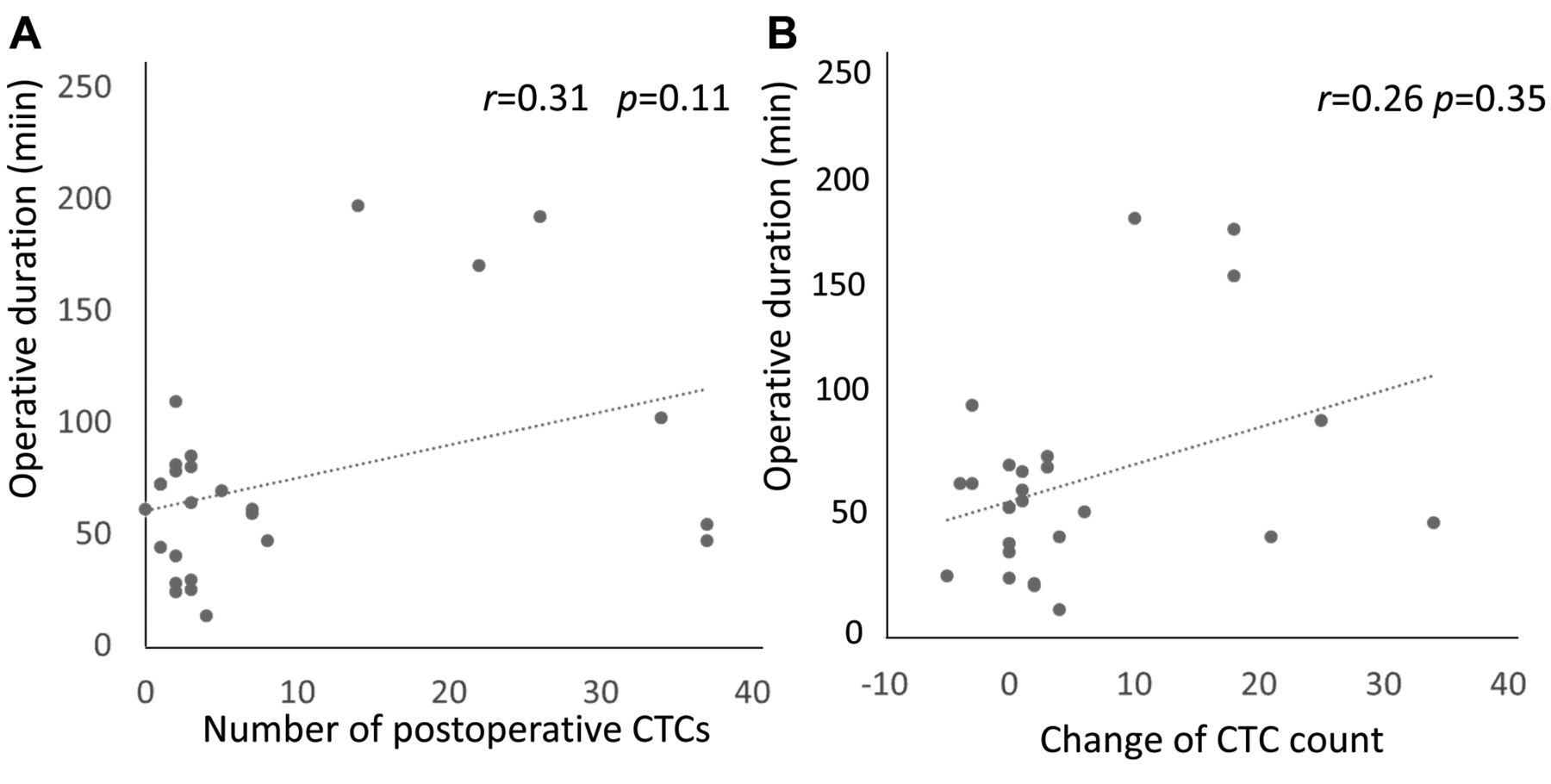
Next, the effect of perioperative parameters on the number of postoperative CTCs was investigated. No significant correlations were observed between the volume of irrigation fluid used during TURBT and the postoperative CTC counts (p=0.18) or the perioperative change in CTCs (p=0.22) (Figure 5). In addition, no significant correlations were observed between the duration of the operation and postoperative CTC count (p=0.11) nor in the change of preoperative to postoperative CTC counts (p=0.35) (Figure 6).

Comparison of the number of circulating tumor cells (CTCs) between non-muscle-invasive (NMIBC) and muscle-invasive (MIBC) bladder cancer. A: Number of preoperative CTCs. B: Number of postoperative CTCs. C: Perioperative change in CTCs. Lines indicate the median, boxes indicate the interquartile range, and bars indicate the minimum and maximum. *Significantly different at p<0.05.
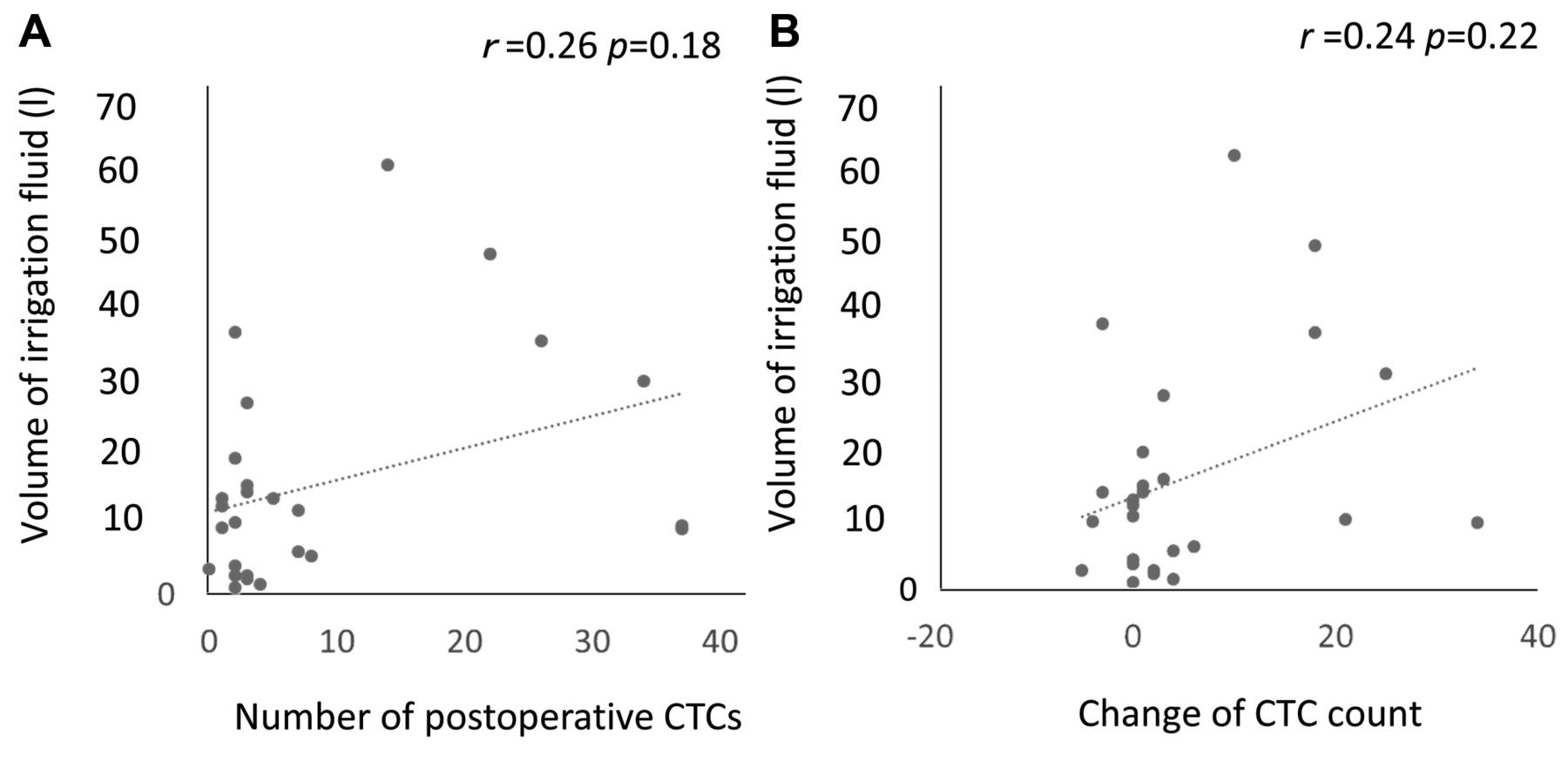
Correlation of the volume of irrigation fluid used during transurethral resection of bladder tumor with the number of CTCs postoperatively (A) and change in the number of CTCs (postoperative–preoperative) (B).

Correlation of the duration of surgery with the number of circulating tumor cells (CTCs) postoperatively (A) and change in the number of CTCs (postoperative–preoperative).
Discussion
In this research, no significant difference was observed regarding the number of CTCs before TURBT between the NMIBC and MIBC groups. However, after TURBT, the CTC count was a significantly greater in the MIBC than in the NMIBC group. Regarding the change in the number of CTCs in the NMIBC and MIBC groups, a significant increase in CTCs was observed only in the MIBC group. Although there have been several studies concerning the possible spread of cancer cells after TURBT (10, 20-22), definitive conclusions were not drawn from these. The present study is the first to demonstrate a significant increase of postoperative CTC counts and a significantly greater change in perioperative CTCs in the MIBC group.
The reasons why there were significant differences regarding the postoperative CTC counts and in the change in perioperative CTCs between the NMIBC and MIBC groups are likely to be as follows. In MIBC, the normal bladder structure is thought to be destroyed due to the cancer invasion of the detrusor muscle (3). Thus, irrigation fluid containing many cancer cells is able to flow into the systemic circulation through the venous system, leading to the increase in postoperative CTCs. On the other hand, there was almost no change in the number of CTCs between before and after TURBT in the NMIBC group. One of the reasons why there was no change in the CTC counts between before and after TURBT in the NMIBC group might be that both the volume of irrigation fluid and the duration of surgery were significantly lower in the NMIBC group than in the MIBC group. However, no significant correlations between the postoperative CTC count and the volume of the irrigation fluid or the surgical duration were observed. Therefore, because in NMIBC normal bladder structure is not destroyed, the spread of cancer cells into the systemic circulation might be avoided despite the occurrence of excessive pressure of the irrigation fluid during TURBT.
The present results showed that TURBT performed for NMIBC was safe from the perspective of the dissemination of cancer cells. However, performing TURBT for MIBC requires more attention to the excessive pressure of the infusion fluid and excessive resection of the tumor in the deep layer because cancer cells might be spilled into the venous system (3). VI-RADS using mpMRI was recently developed (13). Several validation studies demonstrated that VI-RADS accurately assessed muscle invasion (14, 23, 24). If bladder cancer definitely invades the muscle layer as evaluated by VI-RADS, excessive resection for pathological confirmation of muscle invasion might be avoided. By doing this, because the change in CTCs between before and after radical cystectomy was not observed in the preliminary investigation of the present study, distant metastasis in the early postoperative period after radical cystectomy might be prevented. Further studies are needed to clarify the possibility of provoking distant metastases due to excessive resection during TURBT for MIBC.
Several limitations must be considered in the present study. Firstly, this study was conducted at a single center. Investigations at multiple centers would be preferable. Secondly, the observation period was too short to determine any association between the emergence of CTCs in the peripheral veins and distant metastasis. A longer observation period would be needed to make definite conclusions. Finally, the CTC count might be diminished by the percolatory function of the capillary bed in the lung because the specimen of blood analyzed was gathered from a peripheral vein in this study. Engilbertsson et al. placed a venous catheter into the inferior vena cava to directly collect the CTCs before and after TURBT (10). However, even in their study, CTCs were detected from the peripheral vein, although the number of CTCs detected was less from the peripheral vein than from the inferior vena cava (10). In the present study, considering the invasiveness for the patients, insertion of a venous catheter into the inferior vena cava was not performed. However, the FISHMAN-R flow cytometer that was used in the present study has superior sensitivity compared to the CellSearch system that was used in the study conducted by Engilbertsson et al. (10, 11). In fact, the number of CTCs detected from the peripheral vein was greater in the present study than in that by Engilbertsson et al. (10, 11).
Conclusion
The present study showed that more carcinoma cells were discharged from the bladder in patients with MIBC than in those with NMIBC after TURBT. Excessive resection of the deep layer and excessive pressure of the infusion fluid should be avoided to prevent expelling cancer cells into the systemic circulation. To avoid distant metastases in the early postoperative period, careful and sufficient follow-up is needed for patients in whom CTCs are detected.
Footnotes
Authors' Contributions
Nobuhiro Haga contributed to the conception and design of the study. Kazuna Tsubouchi and Hiroko Maruta drafted the manuscript. Tomoyuki Koguchi contributed to the acquisition of the data. Seiji Hoshi contributed to the analysis and interpretation of the data. Soichiro Ogawa and Junya Hata performed the statistical analysis. Hidenori Akaihata contributed to the administrative, technical or material support. Yoshiyuki Kojima was the study supervisor.
Conflicts of Interest
The Authors have no conflicts of interest in regard to this study.
- Received June 7, 2020.
- Revision received June 30, 2020.
- Accepted July 2, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}