


Abstract
Background/Aim: Little evidence exists regarding a relationship between survivin expression and prognosis in small cell lung cancer (SCLC). We investigated the relationship between survivin expression, clinical characteristics and prognosis in SCLC patients. Materials and Methods: We retrospectively reviewed medical records of study patients and analyzed their tumor sections using nuclear survivin labeling index (LI). Results: A significant correlation between nuclear survivin LI and clinical stage was found (p=0.012). In multivariate analysis, a significant association was found between survival and clinical stage (hazard ratio (HR)=2.09; 95 % confidence interval (CI)=1.08-4.31; p=0.027) but not between survival and nuclear survivin LI (HR=0.96; 95 % CI=0.91-1.02; p=0.2). Conclusion: We did not find any positive relationship between nuclear survivin expression and survival in SCLC patients. Conversely, we found a positive relationship between clinical stage and nuclear survivin LI, which is considered to be useful in deciding treatment strategies.
Survivin is a 16.5-kDa protein, which belongs to the human inhibitors of apoptosis protein family (1). Survivin inhibits caspase activity and apoptosis (2). Survivin is expressed in the nucleus and/or cytoplasm of cells in a variety of malignant tumors. In the cytoplasm, survivin functions as an inhibitor of apoptosis, while, in the nucleus, survivin interacts with aurora kinase B and the inner centromere protein to complete mitosis (3).
Survivin is over-expressed in various types of malignant tumors, including lung cancer. Prognostic values of survivin in lung cancer are still controversial. Most studies investigating survivin expression in lung cancer have focused on non-small cell lung cancer (NSCLC), rather than small cell lung cancer (SCLC) (4-6). Recently, an inconsistent relationship between survivin expression and prognosis in SCLC has been reported. Rosato et al. reported that survivin expression does not impact prognostically on SCLC (7), conversely Chen et al. reported that over-expression of survivin in SCLC might predict poor prognosis (8).
In earlier studies, survivin expression has usually been evaluated using a scoring system (5-8). In two previous reports with regard to SCLC, survivin expression was observed in the cytoplasm of cells in SCLC. However, in general, cell cytoplasm in SCLC patients is considered to be difficult to observe and evaluate such expression. In fact, potential pitfalls in determining localization of survivin by immunohistochemistry have been discussed (9).
Association of survivin expression with prognosis in SCLC is controversial. We, therefore, investigated the relationship between survivin expression, clinical characteristics, and prognosis of SCLC patients. In the present study, we evaluated nuclear survivin expression only, rather than cytoplasmic survivin.
Material and Methods
Patients. A total of 32 tissue blocks were used from the files of the Laboratory Medicine in Toneyama National Hospital. Of these, 16 were obtained by trans-bronchial or computed tomography (CT)-guided needle biopsy from SCLC patients between January 2010 and December 2011, while 16 were obtained by surgical resection between April 2003 and March 2012. We also reviewed the medical records of patients and focused on age, gender, smoking status, tumor size and clinical stage.
The present study was approved by the Toneyama National Hospital Institutional Review Board (Approval number: 1407). This approval allowed for retrospective chart review and anonymous reporting of results without informed consent.
Patients' characteristics.
Immunohistochemistry. For immunohistochemical analysis of survivin, one representative tissue block from each tumor was used from which 5-μm-thick sections were prepared. Immunohistochemical staining was performed using an avidin-streptavidin immunoperoxidase method with an anti-human survivin rabbit polyclonal antibody (Novus Biologicals, Littleton, CO, USA) at a 500-fold dilution. Antigen retrieval was performed by incubation of deparaffinized sections in the cell condition 1 solution at standard degree and immunohistochemical staining using an automated Benchmark system (Ventana Medical Systems, Tsucon, AZ, USA) according to the manufacturer's instructions.
To estimate nuclear survivin labeling index (LI) in each tumor, nuclei stained positively or negatively were counted automatically using the Win Roof software (Mitani Co, Tokyo, Japan). Nuclear survivin LI was calculated after counting 500-1,500 tumor cells. More than 10% of LI was defined as positive survivin expression and we investigated patients who were positive for such expression.
Data analysis. All comparisons were performed with the JMP version 8 statistical software package (SAS Institute, Cary, NC, USA). Comparisons were performed using the Wilcoxon rank sum test for continuous variables. Spearman's correlation analysis was used to analyze correlations between nuclear survivin LI and clinical characteristics of study patients. The impact of survivin expression on survival was assessed by the Kaplan–Meier method and determined by the log-rank test. The influence of clinical variables, including nuclear survivin LI on survival, was assessed with the Cox regression model. For all analyses, a value of p<0.05 was considered to indicate a statistically significant difference.
Results
Patients. The characteristics and nuclear survivin expression of study patients are shown in Tables I and II. Nuclear survivin LI was above 10% in most patients.

Differences of nuclear survivin labeling index.

Kaplan-Meier survival curve of SCLC patients.
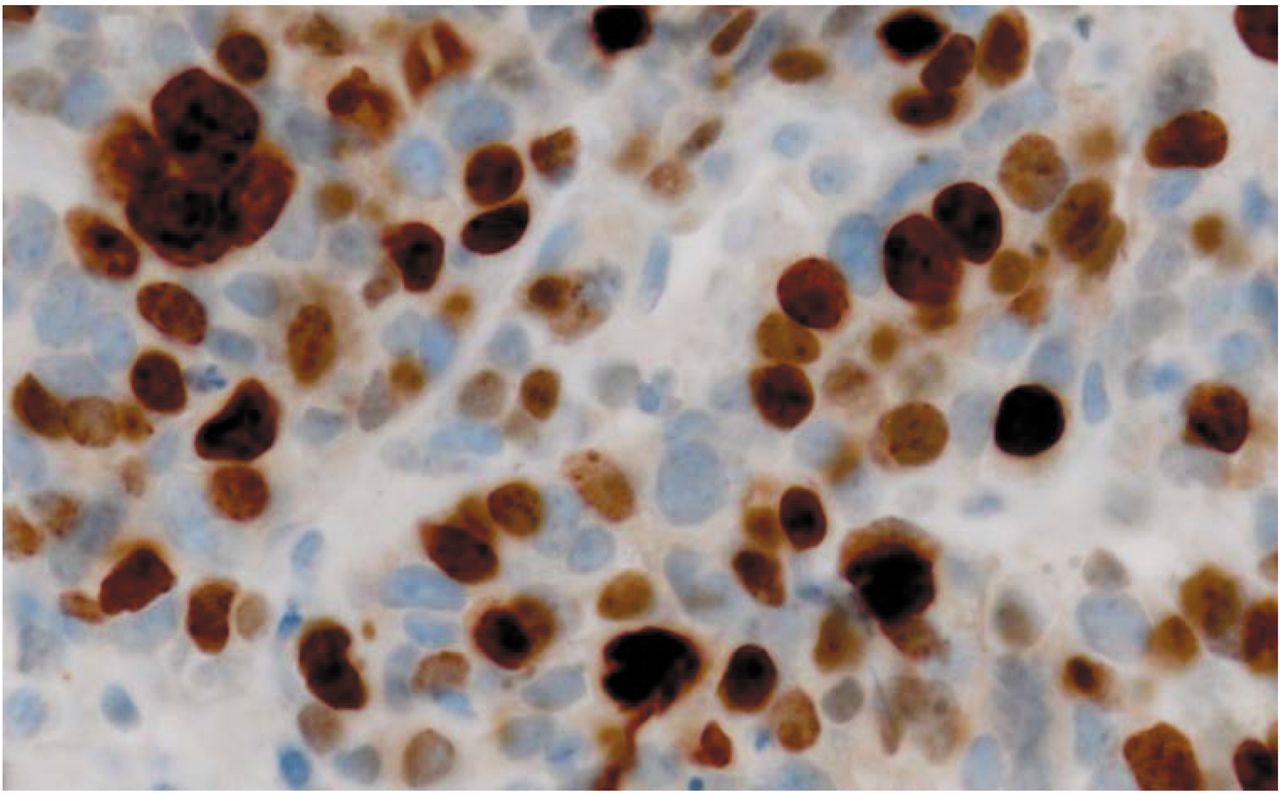
Immunohistochemical staining of nuclear survivin expression in small cell lung carcinoma.
Nuclear survivin expression in SCLC patients.
Correlation between nuclear survivin LI and clinical characteristics of SCLC patients.
Multivariate survival analysis.
Nuclear survivin expression. The differences in nuclear survivin LI between each stage in study patients are shown in Figure 1. The advanced stages showed high nuclear survivin LI and a significant difference between the I, II-stage group and the III, IV-group was seen (stage I, II vs. III, IV, p=0.0045, limited disease vs. extended disease, p=0.039). Correlations between nuclear survivin expression and patients' characteristics. Correlations between nuclear survivin LI and clinical characteristics of study patients are shown in Table III. A statistically significant correlation between nuclear survivin LI and clinical stage of study patients was found (p=0.012).
Survival analysis. Analysis of nuclear survivin LI relationship with overall survival (OS) is shown in Figure 2. The median OS in the groups with LI <36 and >36 were 464 days and 790 days, respectively, but the difference in OS between the groups was not statistically significant (log-rank p=0.671). According to multivariate analysis with the Cox regression model using characteristics of study patients, including clinical stage, tumor size, and nuclear survivin LI, a significant association between survival and clinical stage was found (hazard ratio (HR)=2.09; 95 % confidence interval (CI)=1.08-4.31; p=0.027). However, no significant association between survival and nuclear survivin LI was found (HR=0.96; 95 % CI=0.91-1.02; p=0.2) (Table IV).
Discussion
We did not find any positive relationship between nuclear survivin expression and survival in SCLC patients. Therefore, we conclude that nuclear survivin expression could not indicate prognosis of SCLC patients. On the other hand, in the present study, nuclear survivin LI was elevated with advance of clinical stage and a positive correlation was also found between nuclear survivin LI and each clinical stage of SCLC patients. Furthermore, a significant association between survival and clinical stage was also found. In general, clinical stages would indicate prognosis of patients and clinicians would choose their treatment strategy based on this concept. Therefore, nuclear survivin LI is considered to be a useful factor in deciding for treatment strategy in SCLC.
Only two previous reports have investigated the relationship between survivin expression and survival of SCLC patients. One report concluded that survivin expression did not impact prognostically on SCLC (7); on the other hand, the second report concluded that over-expression of survivin in SCLC might predict poor prognosis (8). In addition to these two studies, a further study investigated survivin expression in SCLC patients. The authors concluded that expression of survivin was decreased in SCLC compared to NSCLC; however, they did not investigate the relationship between survivin expression and survival in SCLC patients (10). According to a report by Li et al., there is much controversy regarding relationships between expression of survivin and prognosis of cancer patients (9). A considerable amount of data has been accumulated up to now in NSCLC in comparison with SCLC (4-6); however, the relationship between expression of survivin and prognosis of NSCLC patients is controversial. Taking these studies, including the present study into consideration, we conclude that the prognostic impact of nuclear survivin expression in SCLC remains to be determined.
Functions of survivin in the cell depend on its location. The nuclear pool of survivin is considered to be involved in promoting cell proliferation, whereas the cytoplasmic pool of survivin may participate in controlling cell survival (9). In general, cell cytoplasm in SCLC patients is difficult to observe and, therefore, evaluation of survivin expression becomes a hard task to accomplish. Cells in small cell carcinomas are of small dimensions with tiny amounts of cytoplasm (11). In fact, potential pitfalls in determining localization of survivin by immunohistochemistry have been discussed (9). In the present study, we could not observe cytoplasm in most cells of SCLC patients (Figure 3). Considering the difficulty in identifying cytoplasmic survivin, we excluded cytoplasmic expression of survivin from the analysis.
In conclusion, we did not find any positive relationship between nuclear survivin expression and survival in SCLC patients. Conversely, we found a positive relationship between clinical stage and nuclear survivin LI. Thus, nuclear survivin LI is considered to be a useful factor in deciding strategies for SCLC treatment.
- Received February 6, 2015.
- Revision received February 16, 2015.
- Accepted February 17, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Factors and Treatment of Early-stage Small-cell Lung Cancer
- Karnofsky Performance Score, Radiation Dose and Nodal Status Predict Survival of Elderly Patients Irradiated for Limited-disease Small-cell Lung Cancer
- Prognostic Factors Including the Expression of Thyroid Transcription Factor 1 (TTF1) in Patients Irradiated for Limited-disease Small Cell Lung Cancer
- Impact of the Radiation Dose on Survival after Radiochemotherapy for Small-cell Lung Cancer
- Karnosky Performance Score and Radiation Dose Predict Survival of Patients Re-irradiated for a Locoregional Recurrence of Small Cell Lung Cancer