


Abstract
Anaplastic lymphoma kinase (ALK) gene re-arrangements are present in approximately 4% of patients with non-small cell lung cancer (NSCLC), mostly in non-smokers with adenocarcinoma. V-KI-RAS2 Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations are more common in smokers. These molecular lesions were usually described as are mutually exclusive. We herein describe a rare case of co-existence of ALK and KRAS abnormalities in adenocarcinoma tumor with massive local growth (disproportionality of clinical symptoms) and rapid central nervous system (CNS) metastases spread. T3N1M0 stage tumor (size: 10×12×13 cm) in upper lobe of the right lung was diagnosed in a 56-year-old Caucasian male smoker. Adenocarcinoma of solid predominant was surgically resected with chest wall reconstruction. One month after surgery, CNS metastases were diagnosed and subsequently treated with radiotherapy. We noted an 8-month overall survival from tumor resection. In the case of comorbidity of disorders in the ALK (uncertain prognostic significance) and KRAS gene (described as unfavorable prognostic factor), these abnormalities may ultimately decide the course of the disease in the form of brain metastases.
Anaplastic lymphoma kinase (ALK) re-arrangements occur in approximately 4% of patients with non-small cell lung cancer (NSCLC), mostly in non-smokers with adenocarcinoma. Recently described ALK gene rearrangements, mostly in the form of echinoderm microtubule-associated protein-like 4 - anaplastic lymphoma kinase (EML4-ALK) fusion gene may lead to malignant transformation. The molecularly-targeted drug - crizotinib - a selective inhibitor of ALK and MET proto-oncogene (hepatocyte growth factor receptor - HGFR) was registered in patients with the presence of ALK fusion gene. Available data show that patients with ALK rearrangement, who were treated with crizotinib or LDK378 demonstrate a significant improvement in objective response rates (ORR) and progression-free survival (PFS) in comparison to standard second-line chemotherapy or best supportive care (BSC) in previously treated patients with NSCLC (1, 10, 9). Overall survival (OS) in crizotinib-naive patients with advanced adenocarcinoma may also vary depending on the status of ALK rearrangements, which indicates its potential prognostic significance (11).
V-KI-RAS2 Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations are present in approximately 20-30% of Caucasian patients with lung adenocarcinoma, usually in former or current smokers. Despite many clinical trials assessing various compounds, effective targeted-therapy for NSCLC patients with a mutation in the KRAS gene is still unknown. A novel promising drug - selumetinib (AZD6244, ARRY-142886) - is a potent and selective inhibitor of the mitogen-activated protein kinase kinase 1 (MAP2K1, MEK1) and MEK2, which block downstream of the KRAS pathway. Available data show that patients with advanced NSCLC, with KRAS mutations, who were treated with selumetinib and docetaxel showed a significant improvement in PFS in comparison to docetaxel-alone therapy. KRAS mutations allow to predict shorter disease-free survival (DFS) and OS both for patients treated with surgery and/or standard chemotherapy (7).

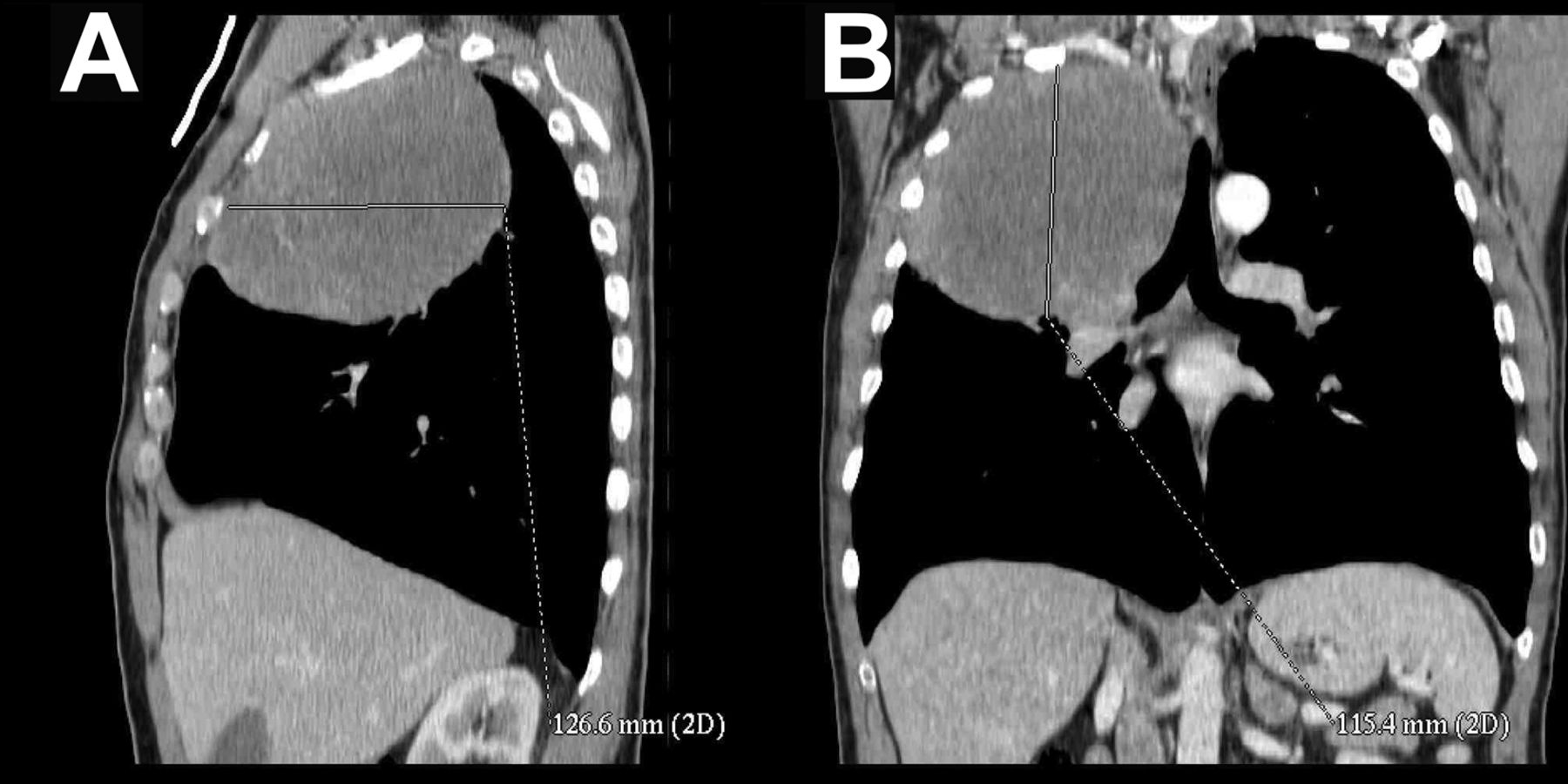
Tumor of the upper lobe of the right lung visible on CT-scan in lateral (A) and anterio-posterior projection (B).
In the present case report, we describe a rare case of lung adenocarcinoma with massive locally advanced tumor, which initially grew without distant metastases and clinical symptoms in a 56-year-old Caucasian male smoker. After a detailed molecular analysis a rare coexistence of ALK gene rearrangement, ALK amplification and KRAS gene mutation was detected in this patient.
Case Report
In February 2013, a 56-year-old Caucasian male reported to his general practitioner because of recurrent infection of upper respiratory tract, chest and spine pain. Patient has no familial history of cancers. He was treated with standard non-steroid anti-inflammatory drugs. In march 2013, patient was admitted to the Department of Thoracic Surgery with the initial diagnosis of a right lung tumor. At the time, he denied any respiratory symptoms or paraneoplastic syndromes and remained in good performance status (PS=1 according Eastern Cooperative Oncology Group - ECOG scale). He was heavy-smoker of more than 30 cigarettes per day between his 25th to 56th years. Two years before tumor diagnosis, computed tomography (CT) scans showed small nodule in upper lobe of right lung.
Recent CT scans showed large (size: 10×12×13 cm) tumor in upper lobe of the right lung without noticeable infiltration or metastases (Figure 1A and B) (Figure 2). Results of pulmonary function tests had normal values. Until march 2013 the patient had undergone right-sided pneumonectomy with chest wall reconstruction. Using immunohistochemical staining, moderately-differentiated adenocarcinoma with solid predominant and weak mucus production (cytokeratin, thyroid transcription factor-1and grade status: CK7+, CK20− and TTF1+, G2 respectively) was diagnosed. Pathomorphological stage of T3N1M0 was defined because of presence of metastases in two regional lymph nodes and also by chest wall infiltration. In April 2013, central nervous system (CNS) metastases were diagnosed. Therefore, he was qualified to CNS radiotherapy with initially remission of metastases in CNS. In October 2013, patient died because of progression of multiple CNS metastases.

Tumor of the upper lobe of the right lung visible on CT-scan.

Representative figure of amplification and rearrangement of ALK gene region. Multiplied ALK gene copy number (A, B) and single signal from red probe (B), as shown by FISH analysis.
The molecular testing for searching of driver mutations in different oncogenes was performed in formalin-fixed, paraffin-embedded (FFPE) tumor tissue obtained during pneumonectomy. To detect for mutations in the epidermal growth factor receptor (EGFR), KRAS and V-raf murine sarcoma viral oncogene homolog B1 (BRAF) genes, we used real-time PCR technique (EGFR Mutation Analysis Kit for Real-Time PCR, EntroGen, Los Angeles, California, USA and Ras/B-Raf Mutation Analysis Panel Kit for Real-Time PCR, Los Angeles, California, EntroGen, USA). The following mutations in the EGFR gene were not detected: G719X in exon 18, S781I, T790M and insertions in exon 20, deletions in exon 19 as well as L858R, L861Q in exon 21. We detected KRAS gene mutation in codon 12 (c.34G>T, G12C). We excluded the presence of another mutations in codon 12, 13 and 61 in the KRAS gene and V600E substitution in the BRAF gene. Moreover, using high-resolution melt (HRM) in the real-time PCR technique, substitution S768R in discoidin domain receptor family, member 2 (DDR2) gene and substitution E542K in phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha (PiK3CA) gene were excluded. For ALK gene re-arrangement estimation, we used a fluorescence in situ hybridization (FISH) technique with specific probes (Vysis ALK Break Apart FISH Probe Kit, Abbott Molecular, Chicago, Illinois, USA). Specimens evaluation was performed in duplicate by two independent observers. Average number of signals from the probe, which was tested, complementary to the ALK gene locus on cell was 6 (ALK gene amplification). Moreover, in the tested locus were found ALK gene rearrangement in 20% of the nuclei (Figure 3A and B).
Discussion
We herein demonstrated a heavy-smoking, adenocarcionoma patient with rare co-existence of ALK gene re-arrangement, ALK amplification and KRAS gene mutation in tumor cells. Importantly, the tumor grew to large size locally without clinical symptoms and metastases to mediastinal lymph nodes. This process could last for even 2 years or more. However, the patient progressed (CNS metastases) after 2 months from radical resection.
Re-arrangement of the ALK and EGFR gene mutations are detected the most frequently in never-smokers or light smokers with lung adenocarcinoma (5). On the other hand KRAS mutations are detected in patients with the same histological type of cancer but usually in former or current smokers (7). This abnormalities, which may have a key role in developing NSCLC usually were considered as mutually-excluding (12). In the available literature there are limited articles (mainly case reports) on the co-existence of these mutations (6).
Data show, that the survival of patients with ALK re-arrangement, who are going to have a surgery, may be worse than ALK-negative cases (2). This could be associated with a high incidence of CNS metastases and malignant pleural effusion in patients with ALK gene abnormalities (8). However, the publication of Lee et al. did not confirm this information. In the quoted study, the incidence of CNS metastases in patients with ALK rearrangement were lower than in patients with wild type of ALK or in patients with EGFR gene mutations (4). The role of ALK re-arrangement in tumor spreading ability and metastases development remain unknown. Moreover, most of the studies report that a mutation in the KRAS gene is a negative prognostic factor for DFS and OS in NSCLC patients after surgery (3).
Conclusion
Co-existence of ALK rearrangement, ALK amplification and KRAS mutations is extremely rare but may occur in adenocarcinoma patients. We considered both ALK and KRAS abnormalities as unfavorable prognostic factors which might affect the course of lung adenocarcinoma and its susceptibility to CNS metastases development in a more aggressive, additive manner. In order to qualify for appropriate treatment, the widest possible determination of mutations in oncogenes associated with the development of NSCLC seems to be reasonable.
- Received March 4, 2014.
- Revision received May 6, 2014.
- Accepted May 8, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}