


Abstract
Aim: The aim of this study was to investigate the expression of CXC chemokine ligand-12 (CXCL12), CXC chemokine receptor 4 CXCR4 and of vascular endothelial growth factor receptor 3 (VEGFR3) in primary urothelial bladder carcinoma and their recurrence in relation to grade and pT status. Materials and Methods: Immunohistochemistry was applied to 67 primary tumor (PC) sections and their recurrenct tumors (RC). Results: The expression of CXCL12 both in PC and in RC was positively associated with tumor grade (p<0.0001 and p<0.0001, respectively) and pT stage (p=0.001 and p=0.007, respectively). The expression of CXCR4 in both PC and RC was also positively related to grade (p=0.001 and p<0.0001, respectively) and pT stage (p=0.008 and p=0.005, respectively). We compared the expression of CXCL12 and CXCR4 in PC related to RC and found that both were more intense in RC than in PC (p<0.0001 and p<0.0001, respectively). In PC and in RC there was no association between the expression of VEGFR3 with tumor grade and pT stage. Conclusion: CXCL12 and CXCR4 expression was related to adverse prognostic markers in urothelial bladder carcinoma through their association with grade and pT stage both in PC and RC. The CXCL12–CXCR4 axis may influence the expression of VEGFR3 in urothelial bladder carcinoma and promote tumor recurrence.
Chemokines belong to a family of small-molecular weight proteins which cause immune inflammatory reactions (1). Moreover, they affect angiogenesis and collagen production, B-cell lymphopoiesis and bone marrow myelopoiesis (2). Chemokine receptors are seven transmembrane G-protein-coupled receptors. Chemokines and their receptors have significant roles in tumor growth, recurrence, metastasis and angiogenesis (3).
CXCL12 is a 68-amino acid small (8-kDa) cytokine, that belongs to the CXC chemokine family (4) and, with its receptor CXCR4, participates in tumor growth, survival and metastasis (5). CXCL12 stimulates cell proliferation through the activation of extracellular signal-regulated kinases (ERK1/2) and alpha serine/threonine –protein kinase (AKT) pathways (6). Tumor neoangiogenesis correlates with CXCL12. Zhongxing et al. (7) suggested that CXCL12/CXCR4 promotes the expression of vascular endothelial growth factor VEGF in human breast and prostate cancer cells through the AKT pathway.
Despite advances in early detection and therapy, urothelial bladder cancer (UC) remains life threatening due to the high incidence of recurrences and metastases (8). In this study, we investigated the expression of CXCL12, CXCR4, and VEGFR3 (receptor of VEGFC) in primary urothelial bladder carcinomas (PC) and their corresponding recurrent sites (RC). Our goal was the correlation of their expression with the prognostic markers grade and stage in the two subgroups of UCs. Moreover we investigated whether the CXCL12–CXCR4 axis is related to the recurrence process.
Materials and Methods
Patients and specimens. In this study, 67 patients with UCs were included. For all 67 patients, we had at our disposal samples from both the primary site and their recurrences (134 specimens in total). Formalin-fixed tissue samples were obtained from transurethral resection of bladder. Sections were evaluated with hematoxylin-eosin stain and were graded according to the WHO 1973 classification (9). In PC, five cases were classified as grade I, 40 as grade II, and 22 as grade III; in RC six cases as grade I, 31 as grade II, and 30 as grade III. Staging was performed according to the TNM (Unione of International Cancer Control (UICC) (2009) classification as follows: seven as pTa, 23 as pT1, seven as pT2, and five as pT3 in the PC subgroup, and eight as pTa, 20 as pT1, six as pT2 and 13 as pT3 in the RC subgroup (10). However, for investigative purposes, UCs were further classified histopathologically into two types: confined to the bladder wall (non-invasive of the muscularis propria) (pTa–T1 tumors) and invasive (stages pT2-4).
Immunohistochemistry. Immunohistochemical staining for CXCL12, CXCR4 and VEGFR3 proteins was performed on 4 μm-thick formalin-fixed paraffin sections, after heating overnight at 37°C with subsequent de-paraffinization in xylene and rehydration through graded alcohol. To enhance antigen retrieval, sections were microwave-treated in 0.01 M citrate buffer (pH 6.0) at 750 W for 15 min for CXR4 and VEGFR3, and in EDTA (pH 8.0) (Trilogy, Cell Marque, Rocklin, CA, USA) at 750 W for 15 min for CXCL12. Endogenous peroxidase activity was quenched with 0.3% hydrogen peroxide in Tris-buffered saline. After rinsing with Tris-buffered saline, normal horse serum was applied for 30 min to block non-specific antibody binding. Subsequently, sections were incubated overnight at 4°C with the following antibodies: mouse monoclonal antibody against human CXCL12 (clone 79018; R&D Systems, Minneapolis, MN, USA) at a dilution of 1:50; mouse monoclonal antibody against human CXCR4 (clone 44716; R & D Systems) at a dilution of 1:200; and rabbit polyclonal antibody against human VEGFR3 (C-20, sc:321; Santa Cruz Biotechnology, Santa Cruz, CA, USA) at a dilution of 1:50.
The sections were incubated in biotinylated horse anti-mouse/rabbit secondary antibodies, followed by peroxidase-conjugated avidin-biotin complex (ABC) (three-step Vectastain ABC Kit; Vector Laboratories, Burlingame, CA, USA), while 3’,3’-diaminobenzidine tetrahydrochloride was used as chromogen. Finally, sections were counterstained with hematoxylin and mounted.
Evaluation of immunohistochemistry. Evaluation of the immunohistochemical staining was performed independently by two pathologists through light microscopic observation and without previous knowledge of each patient‘s clinical data. The score was the average of 10 distinct high-power fields observed under ×400 magnification. As positive controls, we used a paraffin-embedded human breast carcinoma. Negative controls replaced the primary antibody with non-immune normal serum from the same species as the primary antibody.
Specific immunoreactivity of CXCL12 was observed in the cytoplasm of tumor cells (Figures 1 and 2). The extent, as well as the intensity of staining, was categorized into five semi-quantitative classes based on the cut-off value of 50% of tumor cells: 0-1, <50% moderately positively stained cells; 2, <50% strongly positively stained cells; 3, >50% strongly positively stained cells; and 4, 100% strongly positively stained cells.
Immunoreactivity of CXCR4 was observed in the nuclei of tumor cells (Figures 3 and 4). The score was ascertained by consideration of the staining intensity. The intensity of staining was also categorised semiquantitatively on a scale of 0-3 as follows: 0, negative; 1, weakly positive; 2, moderately positive; and 3, strongly positive.
Immunoreactivity of VEGFR3 was observed in the nuclei of endothelial cells in thin-walled vessels as well as in cancer cells (Figure 5). The intensity of staining was determined as 1: weak, 2: moderate.

Cytoplasmic expression of CXC chemokine ligand-12(CXCL12) in primary site of urothelial cancer (pTa). Avidin Biotin Peroxidase Complex(ABC/HRP) ×100.
Statistical analysis. The statistical analysis was performed with IBM SPSS Statistics 20 (International Business Machines Corporation, Armonk, New York USA). The significance level was set at 0.05. Pearson's χ2 test (with continuity correction for 2×2 tables) was used to compare relationships between grade, pT status and immunohistochemical markers (CXCL12, CXCR4, VEGFR3).
Results
Expression of CXCL12 and CXCR4 and VEGFR3. We found a significant relationship of CXCL12 and of CXCR4 expression with tumor grade and pT stage in both the PC and RC groups.
The expression of CXCL12 was positively associated with tumor grade (p<0.0001) and pTstage (p=0.001) in PC (Figure 6). Similarly in the RC group, CXCL12 expression was found to be positively related to grade (p<0.0001) and pT stage (p=0.007) (Figure 7).
The expression of CXCR4 in primary cancer was positively associated with grade (p=0.001) and with pTstage (p=0.008) (Figure 8). In RC, the expression of CXCR4 was also positively associated with grade (p<0.0001) and stage (p=0.005) (Figure 9).
The expression of VEGFR3, was not correlated to grade and pTstage, both in PC and in RC groups.
Comparison of CXCL12 and CXCR4 expression in PCs with their corresponding RCs. Furthermore, we looked for any differences in expression of CXCL12 and CXCR4 between PCs and their RCs. Our results demonstrated that expression of both markers expression was more intense in RCs as compared to PCs. The expression of CXCL12 was positively related to the incidence of recurrence (p<0.0001), whereas the 57.1% of cases with CXCL12 expression score 0 in PC, progressed to expression score of 1 when the tumor recurred; likewise, 37.5% and 12.5% of cases with expression score 1 progressed to expression scores 2 and 3, respectively. Similarly the expression of CXCR4 was significantly up-regulated in the recurrent cases (p=0.0001), with 88.2% of PCs with expression score of 1 becoming score 2 in RCs, and 52.5% of those with expression score 2 becoming score 3, respectively.

Cytoplasmic expression of CXCL12 in the recurrence site of urothelial cancer (pT1). Avidin Biotin Peroxidase Complex(ABC/HRP) ×200.

Nuclear expression of CXCR4 in the primary site of urothelial cancer (pTa). Avidin Biotin Peroxidase Complex(ABC/HRP) ×200.

Nuclear expression of CXCR4 in the recurrence site of urothelial cancer (pT1). Avidin Biotin Peroxidase Complex (ABC/HRP) ×200.

Nuclear expression of VEGFR3 in tumor cells and endothelial cells in the recurrence site of urothelial cancer. Avidin Biotin Peroxidase Complex (ABC/HRP) ×200.
Discussion
In the present study, we observed that the expression of both chemokine CXCL12 and its receptor CXCR4 were correlated with grade and pT stage in PC and RC.
Most studies have stressed the role of chemokines and their receptors in cancer metastasis (11), while it is possible to use them as a prognostic markers. Many studies concluded that the expression of CXCL12 was a prognostic factor for colorectal and prostate cancer (12, 13). Retz et al. suggested that CXCR4 is the only chemokine receptor whose levels correlated with bladder cancer progression. Moreover they demonstrated that CXCR4 was not expressed by normal urothelial cells (14).
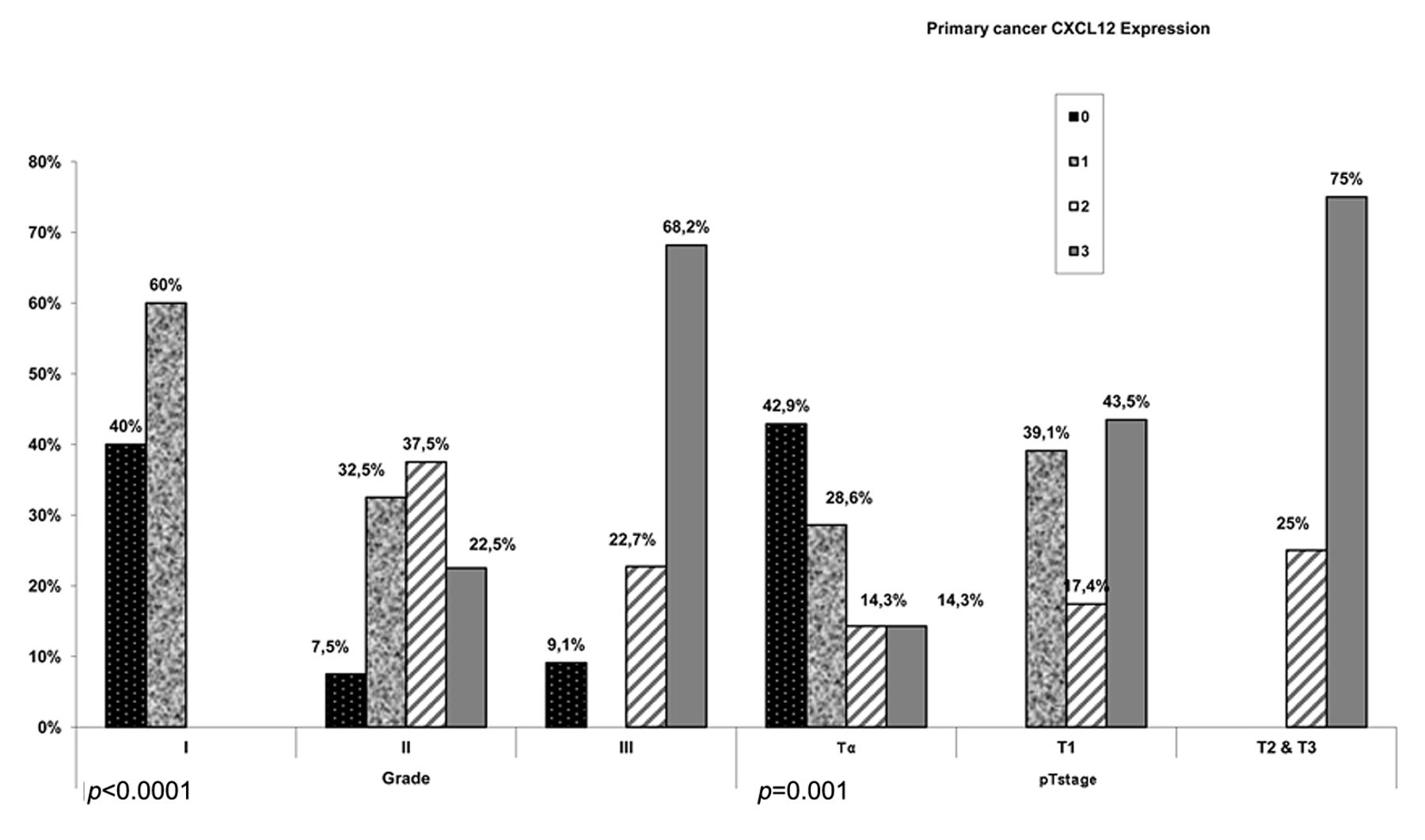
Schematic representation of the positive association of of CXC chemokine ligand-12(CXCL12) with grade and stage in primary cancer (PC).

Schematic representation of the positive relation of CXCL12 with grade and stage in RC.
We performed a cooperative study concerning the intensity of expression of both factors, CXCL12 and CXCR4, which may be prognostic for UC recurrence. In RCs, the staining of CXCL12 and CXCR4 was stronger. Previous knowledge about the effect of CXCL12 stimulation on cancer cells, in association with our results on the stronger expression of CXCL12 in RC, raises the exciting possibility that blocking the CXCL12 pathway may be a valid strategy to target the recurrence of UC (15, 16).

Schematic representation of the positive relation of CXCR4 with grade and stage in PC.

Schematic representation of the positive relation of CXCR4 with grade and stage in RC.
Nuclear localization of CXCR4 in lung cancer, according Spano et al. led to a positive outcome in comparison with cytoplasmic staining (17). Domanska et al. demonstrated that CXCR4 localization in metastatic sites of prostate cancer was nuclear, while that in primary cancer was cytoplasmic (18). In our study, we detected the expression of CXCR4 to be nuclear in both groups of tumors, and to be stronger in RC rather than in PC.
Since our data imply that nuclear staining, in particular, predicts prognosis through its positive association with the disease markers grade and stage, additional research should provide insight into the nuclear function of CXCR4 in UCs.
We investigated the expression of another angiogenic factor VEGFR3 in PCs as well as in RCs. VEGFR3 was expressed in the nuclei of tumor cells and endothelial cells in tumor vessels in both PCs and RCs. There was no statistically significant correlation of it with the grade and pT stage.
In conclusion, our results provide evidence that the expression of the CXCL12–CXCR4 axis was correlated with tumor grade and stage in tissue sections of PC and RC and were in accordance with those of previous studies. Moreover, the stronger expression of the CXCL12–CXCR4 axis in RC than in PC could be a helpful marker for evaluation and prediction of cancer recurrence. Further studies are required for the clarification of possible synergic activity of the CXCL12/CXCR4 axis and VEGFR3 in order to develop a targeted-therapy for bladder cancer recurrence.
Acknowledgements
The Authors would like to thank Miss Maria Grylli for technical assistance and Mr George Chelidonis for statistical results. We are grateful to Mrs Eleni Zacharaki and Dr Chryssanthi Anomitri for editing the manuscript.
- Received March 21, 2014.
- Revision received May 20, 2014.
- Accepted May 21, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}