


Abstract
Background: Bone morphogenetic protein-10 (BMP10), a novel member of the bone morphogenetic protein (BMP) family, has been indicated as a possible tumour suppressor in prostate and breast cancer. However, its role in urothelial tumours remains unknown. In the present study, we examined the role of BMP10 in urothelial cancer cells and the expression of BMP10 in human urethelial cancer of the bladder. Materials and Methods: The expression of BMP10 was examined in human bladder tissues and in the T24 human bladder cancer cell line using immunochemical staining and reverse transcription polymerase chain reaction (RT-PCR), respectively. The biological impact of modifying BMP10 expression, through genetic manipulation, in urothelial cancer cells was evaluated using in vitro models. Results: mRNA for BMP10 and receptors of BMPs was expressed in T24 cell lines. BMP10 protein expression was observed in normal urothelial and stromal cells, but was found to be decreased in or absent from urothelial cancer cells. The frequency of positive staining in normal tissues (9/9) was significantly higher than that in urothelial cancer tissues (6/15) (p=0.007). T24 cells were transfected with BMP10 expression plasmid. It was further demonstrated that overexpression of BMP10 reduced the growth rate of T24 cells, and markedly reduced the motility, and adhesion of T24 cells in vitro. No significant effects were seen on in vitro invasiveness of T24 cells following BMP10 transfection. Conclusion: Expression of BMP10 protein is reduced in cancer cells of bladder tumours. Overexpression of BMP10 has an inhibitory effect on the growth, adhesion, and migration of bladder cancer cells in vitro. This would suggest a potential tumour suppressor role of BMP10 in bladder cancer.
Bladder cancer is the ninth most common type of cancer worldwide (1), the second most common malignancy affecting the genitourinary system (2), and the 13th most common cause of death, accounting for 150,200 deaths from bladder cancer in 2008 worldwide (3). Approximately 90% of all bladder cancers are urothelial carcinomas which are also called transitional cell carcinomas (TCCs) (4). It is a heterogeneous disease with considerable variations of its natural history. The five-year survival rate is 97-98% for patients with a monofocal, well-differentiated and small papillary tumour, whereas this could be 0% if patients have muscle-invasive bladder cancer extending throughout the bladder wall and with gross nodal metastases (5). However, the majority (80%) of patients with bladder cancer present de novo muscle-invasive disease as its first manifestation. Deaths due to muscle-invasive bladder cancer inevitably occur as a result of distant metastases present at the time of locoregional therapy. Progression of cancer after definitive locoregional therapy commonly occurs within the first two years after treatment (6-9). Therefore, early diagnosis of muscle-invasive bladder cancer and its metastasis is a key point for designing systemic therapeutic strategies for these patients.
Recent studies suggest that several growth factors and cytokines that are measurable in peripheral blood are elevated in invasive bladder cancer and are associated with metastatic disease and increased risk of progression. They include insulin growth factor-1 (IGF-1), interleukin-6 (IL-6), and especially transforming growth factor beta-1 (TGF-β1) (10-12). Hemly et al. reported that the TGF-β1 protein can also be used as an attractive target for anticancer therapy, and the absence of TGF-β receptor-1 can be considered a marker of malignant transformation of urothelial cells in bladder cancer (13). Moreover, Eissa et al. reported that combined sensitivity of voided urine cytology with the transforming growth factor-beta (TGF-β) and vascular endothelial growth factor (VEGF) together, was higher than sensitivity of voided urine cytology-alone in detection of bladder cancer (14).
Bone morphogenetic proteins (BMPs) belong to the transforming growth factor-beta (TGF-β) superfamily and were first named by Marshall Urist in 1965 (15). To date, more than twenty members of this group have been identified in humans the since late 1980s (16-20). BMPs can exert their effects through a heteromeric receptor complex, which consists of two types of serine/threonine kinase transmembrane receptors. These are type-I, including BMP receptor type-IA (BMPRIA), type-IB (BMPR1B) and activin A receptor type-I (ACTR1); and Type-II including BMP receptor type-II (BMPR2), activin A receptor type-IIA (ACTR2) and activin A receptor type-IIB (ActR2B) (21, 22). BMPs and their receptors play an important role in bone formation and morphogenesis (23). Recently, there has been evidence that BMPs are involved in tumourigenesis, especially in the development of bone metastases.
In 1999, Arnold et al. reported that BMP2 reduces the proliferation of MCF-7 breast cancer cells, suggesting a crucial role of BMP2 as a member of TGF-β superfamily in repressing cell proliferation (24). Franzen et al., however, reported that BMP2 and BMP7 elicit both growth-stimulatory and -inhibitory effects in cell-specific and differentiation-specific states of breast cancer cells (25). BMP2 and BMP5 can inhibit proliferation and modulate steroidogenesis of human adrenocortical tumour cells in vitro through a BMP-dependent pathway (26). Moreover, BMP2 may act as an angiogenic factor along with VEGF in cancer (27, 28). In neurological tumours, BMP4 reduces tumor-initiating cell pools of human glioblastomas via the BMP-BMPR signalling system (29). BMP4 has been shown to have role in an number of other tumour types, including ovarian and lung cancers (30, 31).
Following the reported role of BMPs in bone formation and development, BMPs have been found to play a role in skeletal metastasis in prostate cancer (21, 32, 33). Brubaker et al. reported growth inhibitory effects of BMP2 and BMP4 in the LNCaP prostate cancer cell line, while PC3 was unaffected (34). In addition, BMP7 inhibited proliferation of androgen-dependent, androgen receptor-expressing LNCaP cells but not castration-resistant PC3 cells (35). Ye et al. reported the decrease or lack of expression of BMP9 and BMP10 in prostate cancer of higher pathological grade. Moreover, forced expression of BMP9 and BMP10 prevented in vitro growth, cell matrix adhesion, invasion, and migration of prostate cancer cells (36-38). These studies, thus, imply that BMPs plays a critical role in tumourigenesis. However, the role of BMPs in urothelial cancer of the bladder remains poorly understood. In the current study, the expression of BMP10 was examined in urothelial bladder cancer specimens and bladder cancer cell lines. The biological function of this molecule was investigated in cells which were manipulated to overexpress BMP10 in order to establish the functional role of BMP10 in bladder cancer cells.
Materials and Methods
Materials. T24 (European Collectio of Animal Cell Culture (ECACC), Porton Down, Salisbury, UK) and PNT2C2 (kindly provided by Professor N. Maitland, University of York, England, UK) were used. Cells were routinely cultured with Dubecco's modified Eagle's medium (DMEM) supplemented with 10% foetal calf serum. Polyclonal rabbit anti-human-BMP10 was purchased from Orbigen Inc. (San Diego, CA, USA). Monoclonal mouse antibody to human actin was purchased from Santa Cruz biotechnology, Inc. (sc-8432, Santa Cruz, CA, USA).
Twenty-four bladder samples were collected from the University Hospital of Wales, including fifteen bladder tumour tissues and nine normal background bladder tissues. These tissues were collected immediately after radical cystectomy and transurethral resection of bladder tumour. All protocols were reviewed and approved by the local Ethical Committee and all patients gave written informed consent.
Total RNA preparation and reverse transcription-polymerase chain reaction (RT-PCR). Total RNA was isolated from cells using a Total RNA Isolation Reagent (Advanced Biotechnologies Ltd., Epsom, Surrey, England, UK). cDNA was synthesized from 0.5 μg RNA using a reverse transcription kit (Sigma, Poole, Dorset, UK). The quality of cDNA was verified with amplifying a house-keeping gene, GAPDH. Primer sequences for BMP10, its receptors, and GAPDH are listed in Table I. PCR was performed in a GeneAmp PCR system 2400 thermocycler (Perkin-Elmer, Norwalk, CT, USA). PCR products were separated on a 1.4% agarose gel.
Immunohistochemical staining of bladder specimens. Frozen specimens of bladder cancer (n=15) and normal bladder tissue (n=9) were cut at a thickness of 6 μm using a cryostat (Leica CM 1900; Leica Microsystems UK Ltd., Buckinghamshire, UK). The nature of the samples was independently verified by two pathologists. After fixation, the sections were blocked with horse serum and probed with or without BMP10 antibody for one hour. Secondary biotinylated antibody and the Avidin Biotin Complex were subsequently applied to detect BMP10 expression in accordance with the Vectastain Universal Elite ABC kit protocol (Vector Laboratories, Peterborough, UK). After developing colour with diaminobenzedine (DAB), the sections were counterstained with Gill's haematoxylin. Staining was independently assessed by the Authors.
Construction of expression vector for human BMP10 and transfection. Sets of primers were designed to amplify the entire coding region of human BMP10 (Table I). The correct products were T-A cloned into the open reading frame of a mammalian expression vector, pEF6/V5-His vector (Invitrogen, Inc., Paisley, UK). The recombinant plasmid vectors were transformed into chemically-competent TOP10 Escherichia Coli (Invitrogen). After verification, the expression constructs and empty control plasmid were amplified, purified and used to transfect T24 cells by way of electroporation (Easyjet; EquiBio Ltd, Kent, England, UK). Following selection with a blasticidin, the overexpression of BMP10 in transfected T24 cells was verified and cells used for subsequent analysis.
Primer sequence for PCR.
Western blot analysis for BMP10 protein. Equal amounts of protein lysates from T24 cells were separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE), and blotted onto nitrocellulose sheets. Proteins were then probed with the antibody to BMP10 and peroxidase-conjugated secondary antibodies. Actin antibody was used as a housekeeping control. Protein bands were visualized using the Supersignal™ West Dura system (Pierce Biotechnology, Inc., Rockford, IL, USA), and photographed using an UVITech imager (UVITech, Inc., Cambridge, UK).
In vitro cell growth assay. We used the method previously reported by our laboratories (39). Briefly, the cells were plated into a 96-well plate (2,500 cells/well). Cells were then fixed in 4% formaldehyde on the day of plating, at days 1, 3, and 5 after plating, and then stained with 0.5% (w/v) crystal violet. Following washing, stained crystal was extracted with 10% (v/v) acetic acid and the absorbance determined at a wavelength of 540nm by using a spectrophotometer (BIO-TEK, ELx800, Wolf Laboratories, York, England, UK).
In vitro invasion assay. This was modified from a previously reported procedure (40-42). Transwell inserts with 8μm pore size (Alpha Laboratories, Hampshire, England, UK) were coated with 50 μg Matrigel (BD Matrigel™ Basement Membrane Matrix, BD Bioscience, Oxford, England, UK) and air dried. After rehydration, 20,000 cells were added to each well. After 96 hours cells that had migrated through the matrix to the other side of the insert were fixed in 4% formalin, stained with 0.5% (w/v) crystal violet and counted under a microscope.
In vitro cell-matrix adhesion assay. This procedure was previously described (40-42). Briefly, 40,000 cells were added to each well of 96-well plate previously coated with Matrigel (5 μg/well). After 40 minutes of incubation, non adherent cells were washed off using a balanced salt solution (BSS) buffer. The remaining adherent cells were then fixed and stained with crystal violet. The number of adherent cells was then counted.
In vitro motility assay using Cytodex-2 beads. We followed the protocol described elsewhere (40-42). 1×106 cells were incubated with 100 μl of cytocarrier beads (Sigma-Aldrich, Gillingham, Dorset, England, UK) in 10 ml DMEM overnight. The beads were washed twice to remove dead cells and then resuspended in 800 μl DMEM. 100 μl of beads/cells were transferred into each well of a 24-well plate. After incubation for four hours, the medium was aspirated and cells were fixed with 4% formalin for five minutes. They were then stained with 0.5% crystal violet for 5 minutes. The cells were washed and allowed to dry before counting in a minimum of three random fields per well.
In vitro migration assay (wounding assay). The migration of cells across a wounded surface of a near-confluent cell monolayer was examined (40-42). Cells at a density of 50,000/well were seeded into a chamber slide and allowed to reach near confluence. The layer of cells was then scraped with a fine gauge needle to create a wound of approximately 200 μm. The movement of cells to close the wound was recorded using a time lapse video recorder and analysed using the motion analysis feature in the software package Optimas 6.0 (Seatle, Washington, USA).
Statistical analysis. All statistical analysis was performed using the SPSS 16.0 software (Portsmouth Hampshire, England, UK). Two-sample t-test was used for normally distributed data. Fisher's exact test was used for analysing immunohistochemical staining in bladder tissues. Differences were considered to be statistically significant at p<0.05.
Results
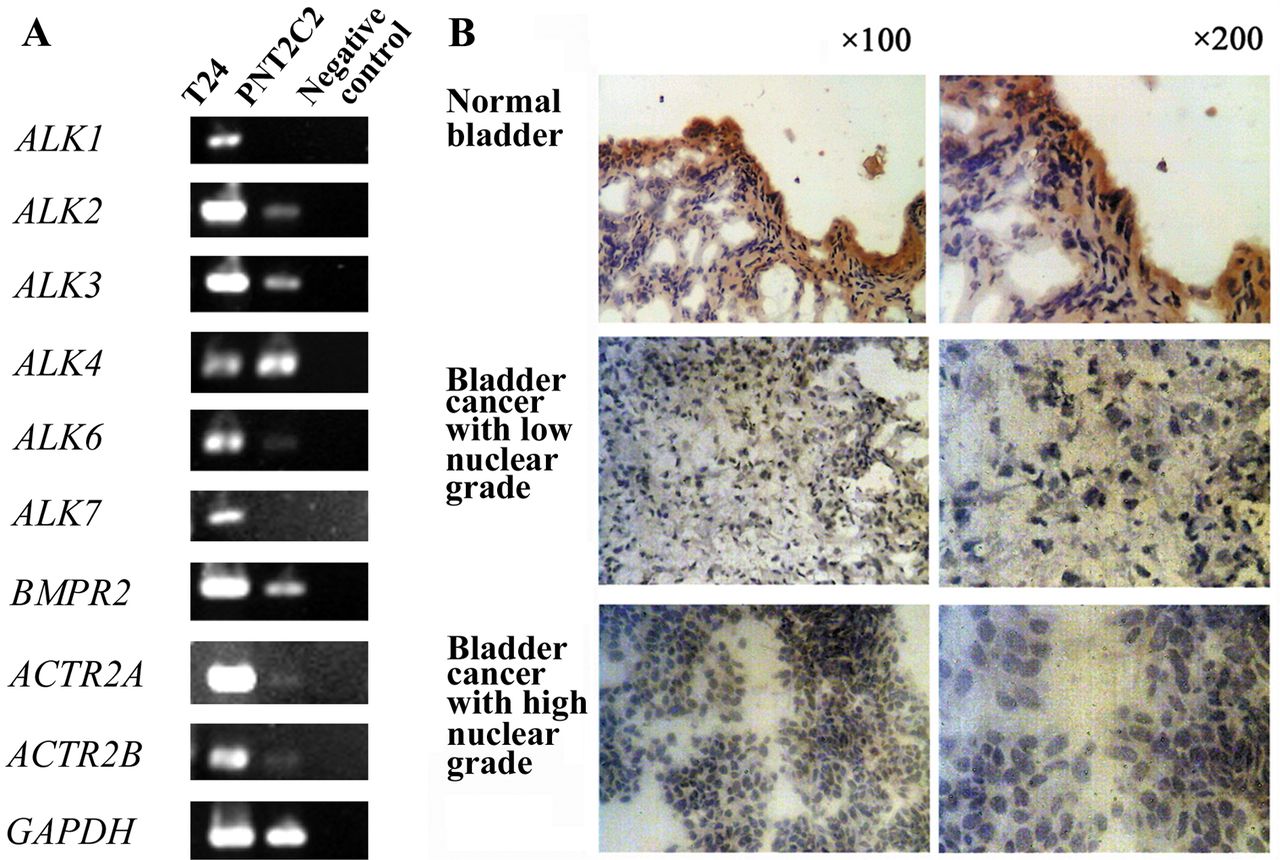
BMP10 and its receptor expressions in different cell lines. The expression of BMP10, ALK1, ALK2, ALK3, ALK4, ALK6, ALK7, BMPR2, ACTR2A, and ACTR2B were examined in T24 and PNT2C2 cell lines using conventional RT-PCR. The transcripts of all these factors were detected in T24 cell lines (Figure 1A). However, transcripts of ALK1 and ALK7 were not detected in PNT2C2 cells (a cell line used as control). Moreover, the expression of transcripts of ALK2, ALK3, ALK6, ACTR2A, and ACTR2B in PNT2C2 cells was lower than that of T24 cells.

Bone Morphogenetic Protein (BMP)-10 expression in T24 cells and bladder tissues. A: Detection of transcripts of BMP10 and its receptors in two cell lines. Type-I and type-II BMP receptor transcripts were all detectable in T24 cells. B: Immunohistochemical staining of human bladder specimens. BMP10 protein was found to be intensely stained in normal bladder urothelial and stromal cells, but the staining was reduced in or absent from malignant urothelial cells, particularly in specimens with higher nuclear grade.
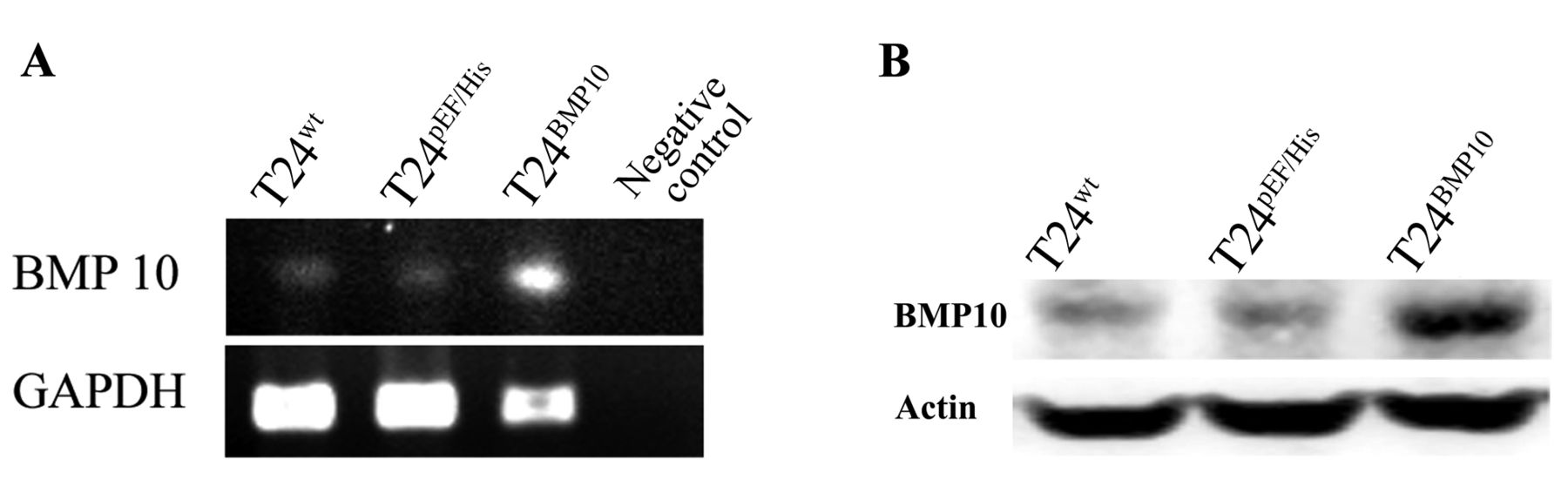
Confirmation of manipulation of BMP10 expression in T24 cells. A: Verification of forced expression of the BMP10 transcript in T24 cells. BMP10 mRNA expression in the T24BMP10 cells was higher than that in wild type (T24wt) and T24pEF/His cells. Representative image from four experiments showing results of RT-PCR. B: Forced expression of BMP10 at the protein level using western Blot analysis of T24 cells. BMP10 protein level was increased in T24BMP10 cells compared with that of wild-type and empty plasmid control cells.
BMP10 protein expression in bladder tissues. In immunohistochemical staining, BMP10 was seen to be present in normal bladder urothelial and stroma cells, but the staining was decreased, or absent from malignant urothelial cells, particularly in specimens with higher nuclear grade (Figure 1B). The frequency of positive staining of normal tissues (9/9) was significantly higher than that of bladder cancer tissues (6/15, p=0.007).
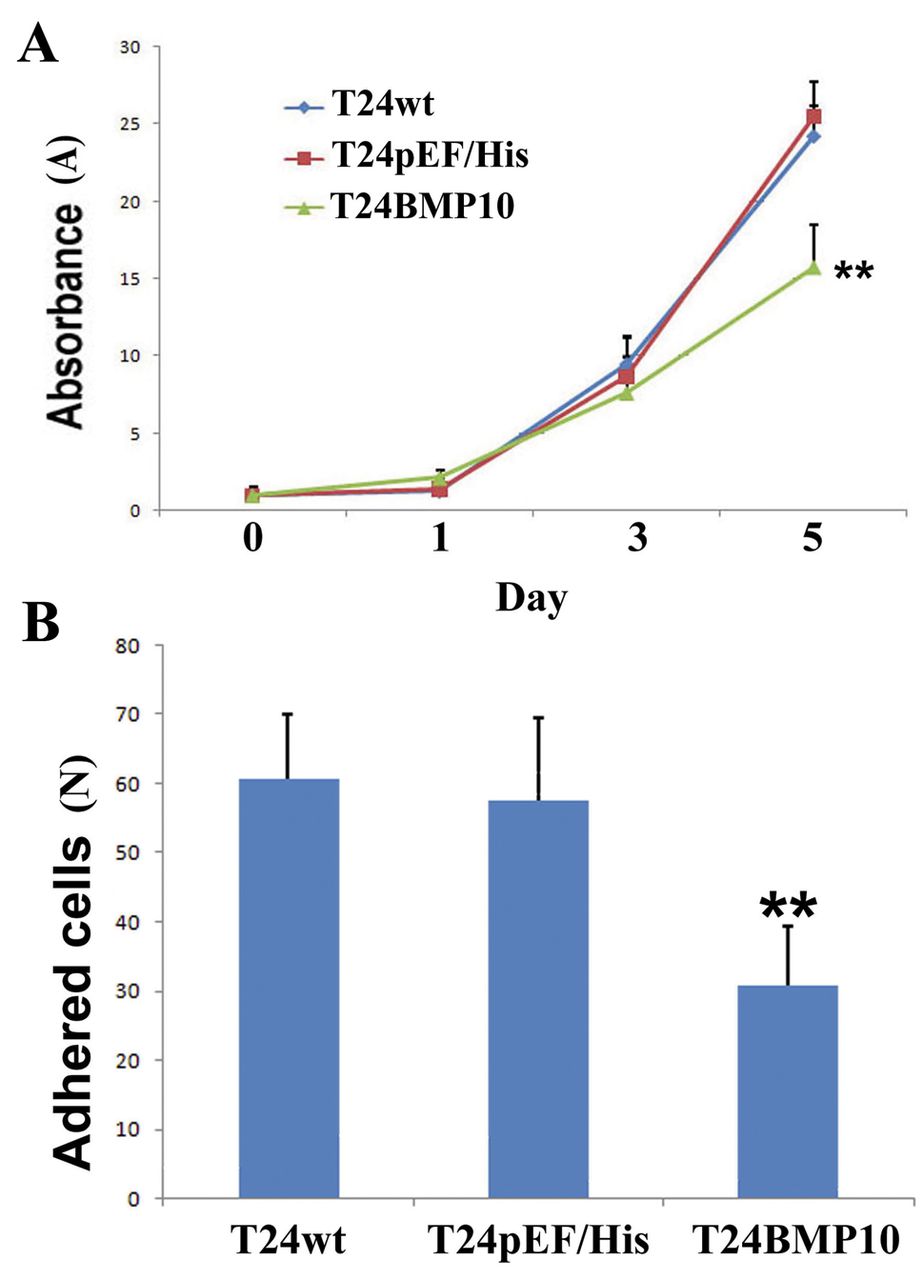
The effect of forced BMP10 expression on growth and cell matrix adhesion of T24 cells. A: BMP10 inhibited T24 cell growth. Reduced cell growth was seen at day 5 in T24BMP10 vs. T24WT and T24pEF/His cells (p<0.001). B: BMP10 expression and in vitro cell-matrix adhesion. All experiments were repeated 5 times. Forced expression of BMP10 reduced the number of adherent T24BMP10 cells (p<0.001). Error bars represent SD. Asterisks indicate significant at p<0.01.
Genetic manipulation of the T24 cell line. T24 cells which expressed a weak level of BMP10 transcripts were transfected with BMP10 expression construct. As shown by RT-PCR analysis (Figure 2A), BMP10 mRNA expression was increased in T24BMP10 cells compared with wild-type (T24wt) cells and empty plasmid control (T24pEF/His) cells (Figure 2A). Moreover, forced expression of BMP10 was also reflected at the protein level in western blot analysis (Figure 2B): an increase in the BMP10 protein level was seen in T24BMP10 cells, compared to controls (Figure 2B).

The effect of forced BMP10 expression on migration and invasiveness of T24 cells. A: The effect of forced expression of BMP10 on migration of T24BMP10 cells. All experiments were repeated four times. The motility of T24BMP10 cells was markedly reduced, compared with wild-type (T24WT) and empty-plasmid control (T24pEF/His) cells (p<0.001). B: The effect of forced expression of BMP10 on cell migration (scratch wounding assay). All experiments were repeated three times. Migration was reduced significantly in T24BMP10 cells compared with wild-type and empty-plasmid control cells (p<0.001). C: The invasiveness of T24BMP10 cells did not significantly differ from that of wild-type and empty plasmid control cells (p=0.77). The error bars represent SD. Asterisks indicate p<0.01.
The influence of BMP10 overexpression on in vitro cell growth. We first determined the effect of BMP10 overexpression on in vitro cell growth. An inhibitory effect on cell growth by BMP10 overexpression was seen in T24 cells. Compared with T24wt (24.18±1.96) and T24pEF/His (25.50±2.27) cells, the absorbance (proportional to cell numbers) of T24BMP10 cells (15.73±2.77) was significantly reduced (p<0.001 vs. both controls) (Figure 3A).
BMP10 overexpression reduced cell-matrix adhesion of bladder cancer cells. T24 cells that overexpressed BMP10 showed a markedly reduced cell-matrix adhesion compared to controls cells (30.8±8.5 for T24BMP10 vs. (60.8±9.3 and 57.7±10.9 for T24wt and T24pEF/His cells, respectively, p<0.001) (Figure 3B).
Cellular motility of bladder cancer cells was inhibited by overexpression of BMP10. The cellular motility was significantly reduced in T24BMP10 cells. The number of migrating cells in the cytocarrier assay was 40.6±16.3 for T24BMP10 cells and was significantly lower than that of T24wt (69.6±16.5) and T24pEF/His cells (70.1±16.3) (both p<0.001) (Figure 4A). In the scratch wounding assay, migration rate of T24BMP10 cells was also reduced significantly compared with the controls (35.77±7.29 μm for T24BMP10 vs. 61.67±11.94 μm for T24wt and 79.40±8.96 μm for T24pEF/His cells, p<0.001 (Figure 4B).
Finally, it was found that there was no significant change of the invasiveness of T24 cells after BMP10 transfection (p=0.77 vs. control cells) (Figure 4C).
Discussion
BMPs were originally isolated from bone extracts and were named for their effect on cartilage formation and de novo bone formation (19), but it was subsequently revealed that BMPs not only control bone formation but also regulate embryonic development and differentiation (43-45). BMPs also play a critical role in homeostasis of the cardiovascular, pulmonary, reproductive, urogenital, and nervous systems in mature organisms (46). Hence, BMPs have been linked to certain diseases, such as primary pulmonary hypertension, fibrodysplasia ossificans progressiva, and juvenile polyposis syndrome (47-49). Interestingly, BMPs have also been shown to have links to cancerincluding colorectal, ovarian and lung cancer and melanoma (30, 50-52).
In the genitourinary system, Kim et al. investigated the potential role of BMP6 and its receptors in renal cell carcinoma (RCC) cells (53). They demonstrated that human RCC tissues frequently had decreased levels of expression of BMPR2, which was associated with insensitivity to the growth-inhibitory effect of BMP6 in human RCC cells. These observations suggest abnormal expression of BMPR2 results in resistance to the growth-inhibitory effect of BMP6. In the case of BMP7, it was frequently overexpressed in prostate tumour and in metastatic bone lesions (32, 54-57). On the other hand, the expression of BMP7 tended to be lower during the development and progression of prostate cancer, whereas its expression was highest in normal prostate glandular tissue (58). In 2008, Ye et al. reported that BMP9 inhibits the growth of prostate cancer cells due to the induced apoptosis, which is related to an up-regulation of prostate apoptosis response-4 through a SMAD-dependent pathway (38).
BMP10 has a 40.5% amino-acid sequence homology with BMP9 and it is mostly abundant in the trabeculae of the embryonic heart, whereas expression is weaker in the liver and the lungs (59). The full gene of BMP10 is ~7.8 kb, which is maped to human chromosome 2p13.3. Initially, it was thought that BMP10 plays an important role in trabeculation of the embryonic heart (59, 60). Ye et al. reported that BMP10 also inhibits the growth of prostate cancer cells largely due to apoptosis induced via SMAD-independent signaling in which XIAP and ERK1/2 are involved. BMP10 can also prevent prostate cancer cell migration and invasiveness (36). In additional, the disease-free survival for the patients with breast cancer with a higher level of BMP10 was significantly longer than those with a lower level of BMP10 expression. Decreasing BMP10 expression correlates to poor prognosis and disease progression, particularly to lymphatic and bone metastasis. The overexpression of BMP10 has broad inhibitory effects on the in vitro growth, invasion, and motility of breast cancer cells (61).
However, to our knowledge, the role of BMP10 in bladder cancer has not been investigated. In the current study, we first noted that BMP10 protein levels were decreased in urothelial cancer of bladder tissues compared with that of normal bladder tissues. Intensive staining was observed within the normal urothelial and stromal cells and was much weaker in or absent from malignant urothelial cells. Unfortunately, due to a limited number of samples, no correlation of BMP10 expression and clinical aspects of the urothelial cancer could be assessed in this study. However, the decrease or absence of BMP10 expression in urothelial bladder cancer at least suggests that there might be a shift in the balance between the tumour and anti-tumour environment during disease progression.
Our results also show that the overexpression of BMP10 can directly affect the growth, motility and adhesion of urothelial tumour cells. By the in vitro cell growth assay, compared with wild-type cells, the growth rate was reduced by about 40% in T24 cells with BMP10 overexpression. In addition, cell-matrix adhesion in T24 cells transfected with the BMP10-expression plasmid was found to be greatly reduced, displaying approximately 50% of the level seen in wild type cells. Moreover, the average distance travelled by BPM10-overexpressing cells was also dramatically reduced compared with controls. Furthermore, according to our results, transcripts of BMPR2 and ACTRs were all detectable in T24 cells. Taken together, these results suggested that BMP10 can directly reduce the aggressiveness of urothelial cancer cells through two types of signal pathway. This is in line with the observation that the expression of BMP10 is decreased in urothelial cancer of bladder specimens. It is well-known that multifocality and polychronotropism are two main characteristics of urothelial bladder cancer. According to the evidence that multifocal tumours occurring in the same individuals demonstrated clonality (62), reimplantation of tumour cells is one of the most commonly accepted theories to explain these characteristics (63, 64). The reduced cell growth, adhesion, and motility, but lack of impact on the invasiveness of urothelial tumour cells suggests that BMP10 may be a key regulator for re-implantation of urothelial cancer of bladder. For muscle-invasive bladder cancer, metastasis of cancer after definitive locoregional therapy commonly occurs within the first two years after treatment, including to the liver, bone, even central nervous system, bowel serosa, and peritoneum. Together with reports that BMPs are involved in metastasis, epithelial-to-mesenchymal transformation, altered cellular behavior, and angiogenesis in human cancer (23), our report has provided further evidence to indicate a novel therapeutic implication of BMP10 in bladder cancer.
In conclusion, BMP10 expression is decreased in urothelial tumours of the bladder. It can suppress cell growth, adhesion, and migration of bladder cancer cells in vitro through two types of signal pathways. This suggests that BMP10 may be a putative tumour-suppressive factor and a novel potential target for therapeutic intervention of bladder cancer.
Acknowledgements
The Authors wish to thank the Albert Hung Foundation and Cancer Research Wales for supporting their work, and Drs David Griffiths and Varna for their expert help in histological evaluation.
Footnotes
-
↵* These Authors contributed equally to this study.
- Received March 18, 2013.
- Revision received April 13, 2013.
- Accepted April 15, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}