


Abstract
Background: Salvage chemotherapy using carboplatin (C), paclitaxel (P), and bevacizumab (BEV) for patients with pre-treated, advanced non-squamous non-small cell lung cancer (NSCLC) has not yet been reported. Patient and Methods: Medical records of patients with non-squamous NSCLC who received CP plus BEV between November 2009 and September 2011 and experienced progression after at least one platinum-based-chemotherapy regimen, were examined in this retrospective study. Results: Twenty-one patients were eligible for this study. The median number of prior chemotherapy regimens was 3 (range, 2 to 9). The median number of cycles of CP with BEV was 4 (range, 1 to 6). Seven patients underwent BEV maintenance therapy, and the median number of cycles of BEV maintenance was 8 (range, 2 to 13). Toxicity levels were acceptable. The overall median survival time was not reached and one-year survival rate was 54.95%. The overall progression-free survival was 6.1 months (95% confidence interval, 4.4-9.3 months). Conclusion: CP with BEV was effective and feasible as a salvage chemotherapy after failure of platinum-based chemotherapy for patients with non-squamous NSCLC.
Non-small cell lung cancer (NSCLC) is the leading cause of cancer-related deaths in Japan. The majority of patients with NSCLC have progressive disease. Use of a platinum doublet is the standard treatment for advanced NSCLC as first-line treatment (1, 2). However, the disease in the majority of patients going on the second-line therapy will be refractory to the initial chemotherapy used.
Docetaxel has been the standard treatment compared with best supportive care (BSC) for NSCLC patients who experience first-line failure (3, 4). Erlotinib, an epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI) improved overall survival (OS) in comparison (compared to placebo in the second or third-line treatment, as it was reported in a major clinical trial report (5). In addition, for non-squamous NSCLC, pemetrexed has been considered to be a reasonable standard of care (6). However, even in these reports, was response rate (RR) was approximately 10%, and progression-free survival (PFS) was about three months, such that satisfactory treatment results have not been obtained.
There is no guideline for chemotherapy (except erlotinib) for NSCLC patients who have failed two systemic therapy regimens. However, many patients have actually received third-line chemotherapy, but the results of salvage treatment are not satisfactory. A consistent approach to patients who become refractory to second-line treatment has not yet been established.
Bevacizumab, released to the market in 2006, is a recombinant humanized monoclonal antibody against vascular endothelial growth factor. A combination of carboplatin (C) and paclitaxel (P) and bevacizumab (BEV), or of cisplatin and gemcitabien and BEV is more useful against advanced NSCLC with a non-squamous histology, compared to conventional chemotherapy, and thus, these combination chemotherapies are now standard regimens for advanced non-squamous NSCLC (7, 8).
One phase III study and one Japanese phase II study of CP plus BEV in patients with previously untreated advanced NSCLC demonstrated an overall RR of 35% and 60.7%, respectively, and a median overall survival time (MST) of 12.3 months and 22.8 months, respectively (7, 9). In particular, CP plus BEV treatment improved overall survival (OS) in non-squamous NSCLC more than CP did alone. Therefore, CP plus BEV has become a standard regimen for non-squamous NSCLC.
As salvage therapy did not produced satisfactory therapeutic effect, we tried the administration of BEV. Since good results have also been reported also by re-administration of platinum in patients with good performance status (PS), we chose combination with CP for which there was evidence in Japan. In this retrospective analysis, we evaluated the efficacy of CP plus BEV as a salvage therapy for patients with advanced NSCLC. The local Institution Review Board approved this protocol prior to initiation of the study.
Patients and Methods
Patient selection. This retrospective analysis enrolled 21 patients who had histological and cytological confirmation of recurrent stage IIIB or IV NSCLC who had received CP plus BEV because of progression after previous treatment for non-squamous NSCLC, between November 2009 and September 2011, at the Osaka Prefectural Hospital Organization in the Osaka Prefectural Medical Center for Respiratory and Allergic Diseases and Kinki-Chuo Medical Chest Center. The cut-off date for this analysis was February 14, 2012.
All patients had received at least one platinum-based chemotherapy regimen, and all patients who harbored an EGFR mutation had received EGFR-TKI treatment prior to receiving CP plus BEV. Furthermore all patients had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0-2, and had measurable lesions by Response Evaluated Criteria in Solid Tumors (RECIST ver1.0).
Treatment methods. In two hospitals, the regimen of CP plus BEV as salvage chemotherapy was as follows. Carboplatin was administered at a dose calculated to produce an area-under-the-curve (AUC) of 5 or 6 mg/(ml ·min), paclitaxel was administered at 160 or 200 mg/m2, and bevacizumab at a dose of 15 mg/kg. All treatments were administered on day 1 of a 21-day cycle, and each cycle was repeated 4-6 times unless there was evidence of disease progression, unacceptable toxicity or patient/physician decision. In the absence of disease progression, patients who had been treated with bevacizumab and had completed at least three cycles of chemotherapy, were decided to procced with bevacizumab monotherapy until disease progression or unacceptable toxicity.
Patients' charactaristics.
In order to start treatement, all patients should have an absolute neutrophil count ≥1,500/mm3, a platelet count ≥100,000/mm3, aspartate aminotransferase and alanine aminotransferase values less than three times the maximum values of the normal range, and total bilirubin and creatinine values less than 1.5 times the maximum values of the normal range. Subsequent doses were modified on the basis of the hematological and non-hematological toxicities at the discretion of the physician in charge. Peripheral blood and biochemical examinations were repeated at least once every two weeks after the initial evaluation.
Evaluation of response and toxicity. Evaluation of efficacy and toxicity in the two hospitals was carried out as follows; tumor response was classified in accordance with the RECIST version 1.1. Patients were evaluated in order to determine the stage of their disease before the start of treatment, and at the time of determination of disease progression or relapse, by complete medical history and physical examination, chest radiography, computed tomography (CT) of the chest and abdomen, and other staging procedures such as magnetic resonance imaging (MRI) of the head. The adverse events of treatment were recorded and graded using the National Cancer Institute Common Toxicity Criteria, Version 3.0 grading system (10).
Statistical analyses. OS was measured from the first day of CP plus BEV treatment to the day of death or last follow-up. PFS was defined as the time between the initiation of treatment and failure (i.e. death or disease progression) or last follow-up. The time-to-event outcomes were compared using the log-rank test. The “R ver. 2.8.1” software (available at http://www.R-project.org; R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analyses.
Patient based hematologic and non-hematologic toxicities of therapy with CP plus BEV.
Results
Patients' characteristics. The characteristics of patients with recurrent or refractory NSCLC are listed in Table I. The majority of the patients (n=17, 81.0%) had an ECOG PS of 0 or 1. All patients had adenocarcinoma, and two patients (9.5%) harbored EGFR mutation status (exon 19 or 21). CP with BEV was administered at carboplatin AUC=6, paclitaxel 200 mg/m2, and bevacizumab 15 mg/kg to 19 patients, and at carboplatin AUC=5, paclitaxel 160 mg/m2, and bevacizumab 15 mg/kg to two patients.
Chemotherapy and toxicity. Eighty-six courses of CP plus BEV were administered in total (median number of course per patient was 4; range, 1 to 6), and seven patients underwent the maintenance therapy (median number of course per patient was 8; range, 2 to 13). All these courses were included in the toxicity analysis.
The principal toxicities of CP plus BEV treatment were neutropenia and neuropathic toxicities, such as numbness. An allergic reaction to paclitaxel was experienced by one patient. Hematological and non-hematological toxicities in the 21 patients are summarized in Table II. All patients experienced higher levels of hematological toxicities. Grade 3 or higher neutropenia, grade 3 decrease in hemoglobin, and grade 3 or higher thrombocytopenia were observed in 18 (85.7%), 1 (4.8%), and 2 patients (9.5%), respectively. Febrile neutropenia was observed in 6 patients (28.6%). The non-hematological toxicities show that CP plus BEV treatment caused six cases of grade 3 or higher toxicities (the main toxicity was neuropathy in 5 patients; one patient developed a grade 3 allergy to paclitaxel, and one developed a grade 3 infection). Dose-reduction was necessary for 6 patients due to the toxicities of CP plus BEV. However, no bleeding events occurred.
Treatment efficacy (n=21).
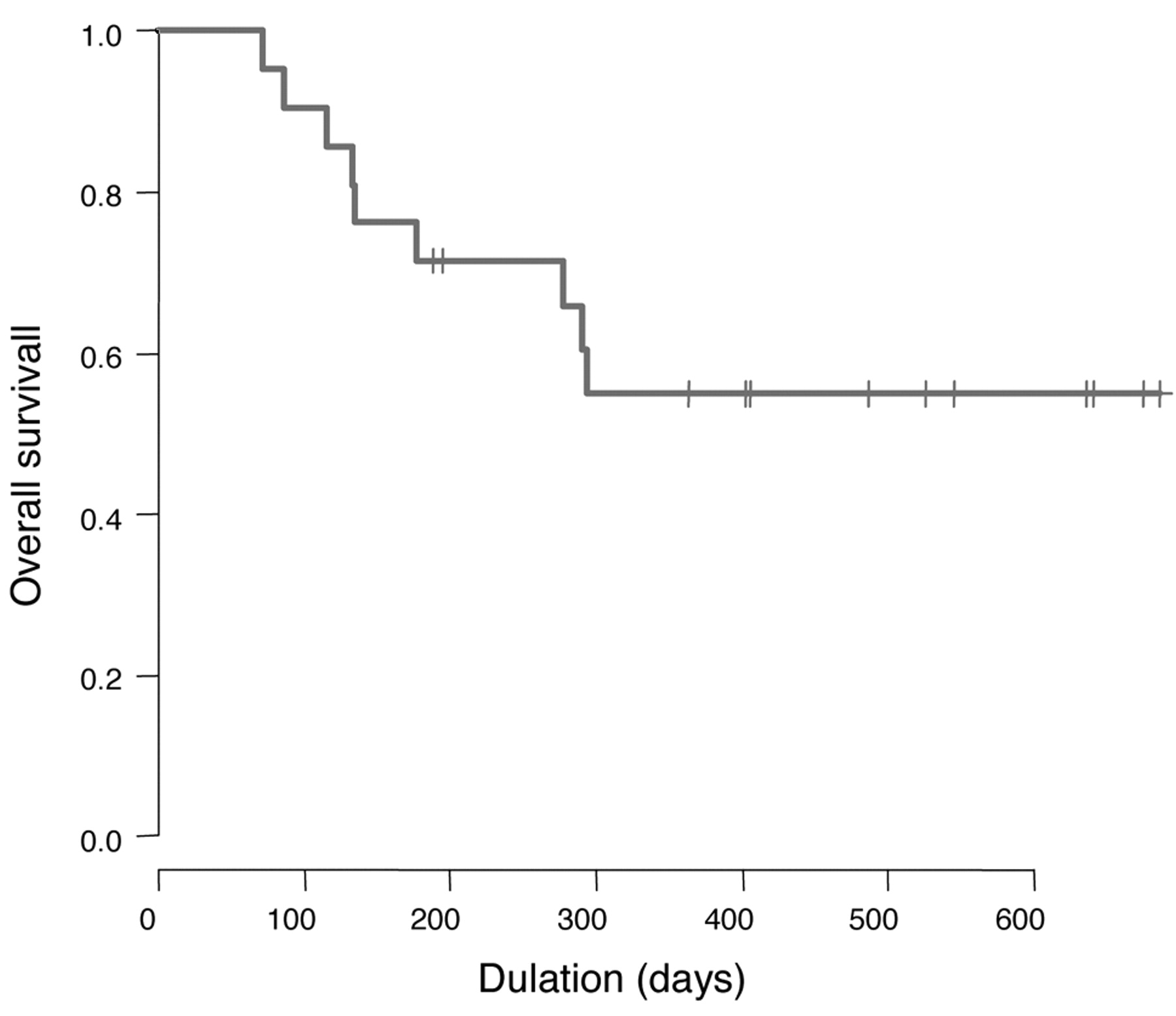
Response to therapy and survival. The objective tumor responses are shown in Table III. Among the 21 patients, 10 achieved a confirmed partial response and 5 had stable disease, for an overall RR of 47.6% and a disease-control rate of 71.4%. Overall survival data are shown in Figure 1 and PFS data are shown in Figure 2. The overall MST was not reached and the one-year survival rate was 54.95%. The overall PFS was 6.1 months (95% confidence interval, 4.4-9.3 months).
Discussion
Reports on salvage chemotherapy with single agents or platinum-doublet therapy for platinum-pre-treated patients with NSCLC have been published. It was reported that among 39 patients with recurrent NSCLC treated with amrubicin and had received two prior chemotherapy regimens including platinum and docetaxel, the best RR was 10.2%, the disease-control rate was 33.3%, and the median duration of OS from the start of the last treatment was 5.7 months (11). Shepherd et al reported on a phase III study that compared BSC with erlotinib in the treatment of platinum-pre-treated patients with relapsed NSCLC. OS and PFS were better in the erlotinib arm than in the BSC arm (6.7 months and 2.2 months vs. 4.7 months and 1.8 months) (5). Smit et al reported on a randomized phase II study, that compared pemetrexed with carboplatin and pemetrexed alone in the treatment of platinum-pre-treated patients with relapsed NSCLC. The RR and median time to progression (TTP) were better in the combination arm than in the pemetrexed monotherapy arm (17% and 4.2 months vs. 11% and 2.8 months) (12). Finally, Kim et al reported on a phase II study using pemetrexed and carboplatin as salvage therapy for platinum-pre-treated patients with NSCLC. The RR, TTP, and OS were 18.8%, 2.3 months, and 9.4 months, respectively (13). Platinum-based chemotherapy may lead to a better response rate and PFS than the use of a single agent for platinum-pre-treated patients with NSCLC (14).

Overall survival of all treated patients (N=21).
The results of the present study showed that CP plus BEV had favorable clinical outcomes (the overall RR, PFS, and MST were 47.6%, 6.1 months and not reached, respectively). There was no death due to toxicity; in fact, moderately tolerated toxicity profiles were observed, which were manageable with conventional supportive care among the patients who had failed standard chemotherapy, including platinum-doublet therapy and EGFR-TKI for these EGFR-activating mutations. Our results were more favorable compared to results of previous reports (12, 13). The addition of bevacizumab to platinum-based chemotherapy in the first-line setting showed benefits in the RR, PFS, and OS (5, 6). Our study suggested that CP plus BEV and bevacizumab maintenance after platinum-doublet therapy for non-squamous NSCLC may improve outcomes, in addition to treatment in the first-line setting.
The incidence of toxicities due to therapy with CP plus BEV was slightly high, especially for neutropenia and neuropathy. The high incidence of neutropenia indicates that more attention should be paid to infections, including febrile neutropenia (six patients; 28.6%). This is particularly true for severe neuropathies. The high incidence of these toxicities may be due to previous chemotherapy. However, in this study, no bleeding events occurred, and the safety for bleeding events was equivalent to first-line bevacizumab with chemotherapy for patients with advanced NSCLC (15).
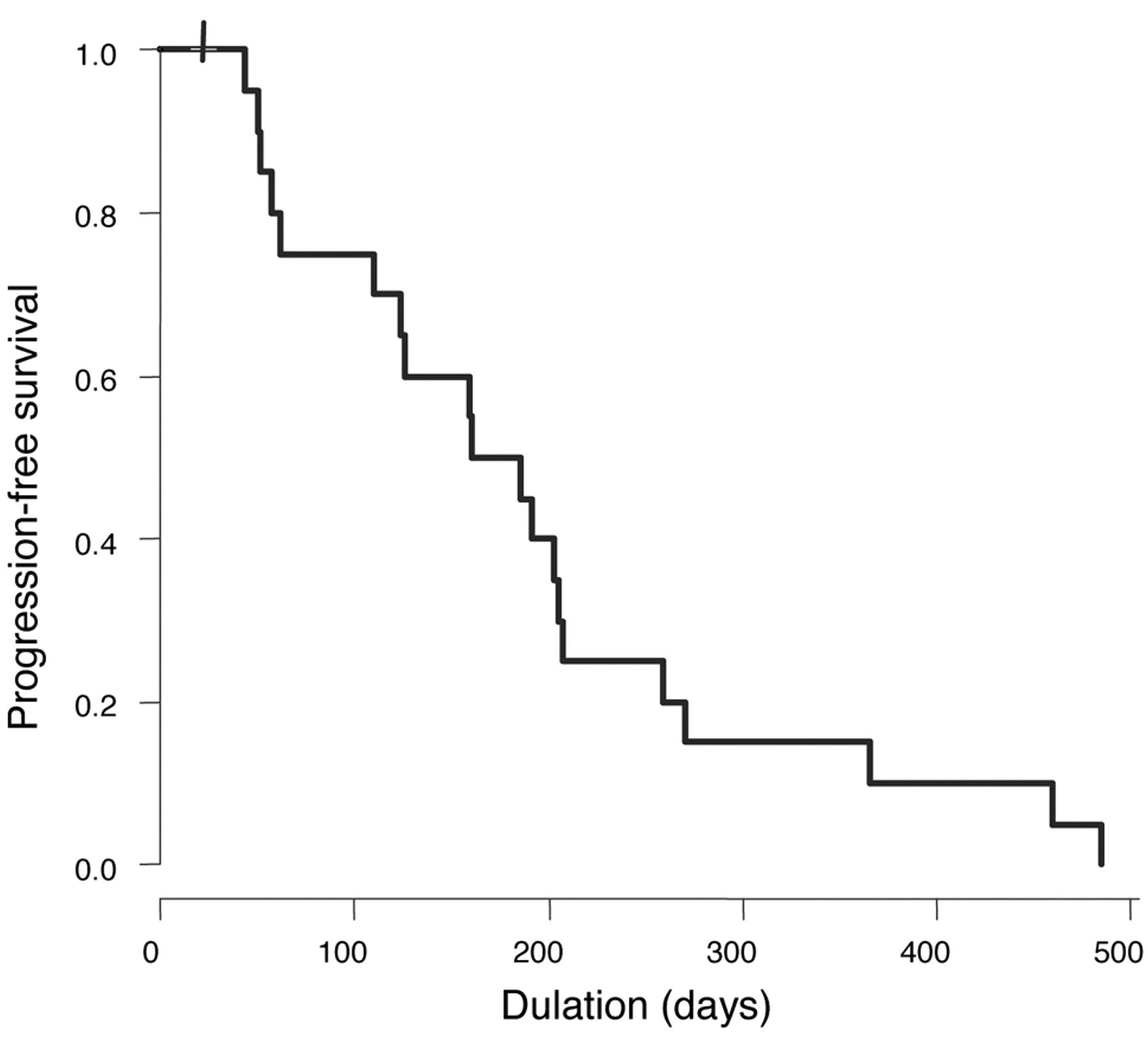
Progression-free survival of all treated patients (N=21).
There is controversy about the role of further administration of chemotherapy in patients failing second-line treatment. However, a number of patients that failed previous chemotherapy have a satisfactory PS to receive further chemotherapy or insist on receiving further treatment despite their poor PS. In these situations, the benefits of further chemotherapy should be carefully assessed.
Conclusion
CP plus BEV is an active treatment against NSCLC that may play a prominent role in second-line treatment and beyond, when the patient has a good PS and sufficient organ function. Patients who survive long enough to receive salvage chemotherapy are a very select population, with a clinical disease course very is different from that of the general population of patients with NSCLC undergoing first- or second-line chemotherapy. Such patients are candidates for treatment with novel therapies, including CP plus BEV as salvage chemotherapy, since there is currently no standard therapy for these patients. This report provides a description of the anticipated clinical course of patients with a good PS, after prior chemotherapy regimens, as well as a baseline for the statistical design of studies to identify novel therapies for such patients.
Acknowledgements
The Authors wish to thank all the participating patients.
Footnotes
-
Conflict of Interest Statement
The Authors have no financial arrangements or relationships with any individuals or organizations that could potentially influence their work.
- Received April 13, 2012.
- Revision received June 16, 2012.
- Accepted June 18, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}