


Abstract
Novel subcellular imaging technology has been developed in order to visualize drug efficacy on single cancer cells in the brain of mice in real time. The efficacy of temozolomide on cancer cells in the brain was determined by observation of subcellular cancer-cell dynamics over time through a craniotomy open window. Dual-color U87 human glioma and Lewis lung carcinoma (LLC) cells, expressing green fluorescent protein (GFP) in the nucleus and red fluorescent protein (RFP) in the cytoplasm, were imaged through the craniotomy open window 10 days after treatment with temozolomide (100 mg/kg i.p. for five consecutive days). After treatment, dual-color cancer cells with fragmented nuclei were visualized, indicating apoptosis. GFP-expressing apoptotic bodies and the destruction of RFP-expressing cytoplasm were also visualized. In addition, the terminal deoxynucleotidyltransferase-mediated deoxyuridine triphosphate nick-end labeling (TUNEL) assay was used to confirm apoptosis visualized by imaging of the behavior of GFP-labeled cancer-cell nuclei. Tumor volume in the treated group was significantly smaller than in the control group (at day 19, p<0.001). The present study demonstrates technology capable of subcellular real-time imaging in the brain that reports induction of cancer-cell apoptosis by therapeutic treatment. More effective drugs for brain cancer and brain metastasis can be screened and can be identified with this technology.
Imaging based on GFP expression in cancer cells (1) has enabled spontaneous metastasis to the brain to be imaged in three different orthotopic nude mouse model systems of human cancer: the PC-3 human prostate cancer cell line (2); the LOX human melanoma cell line (3); and spinal cord glioma model using the U87 human glioma cell line (4, 5).
We have also developed dual-color cancer cells, in which red fluorescent protein (RFP) is expressed in the cytoplasm and green fluorescent protein (GFP), linked to histone H2B, is expressed in the nucleus, in order to visualize nuclear dynamics including cell-cycle events and apoptosis (6-8).
In the present study, we utilized the dual-color cancer cells to image the efficacy of temozolomide at the subcellular level in live nude mice through a craniotomy open window (9).
Materials and Methods
Cells. To establish Lewis lung carcinoma (LLC) or U87 human glioma (U87) GFP-RFP cells, the cells were transfected with retroviral RFP and H2B-GFP vectors, as previously described (7). Cells were cultured in Dulbecco's Modified Eagle's Medium (DMEM) (Hyclone Laboratories, Logan, UT, USA) supplemented with 10% fetal bovine serum (FBS; Hyclone Laboratories).
Animals. Athymic NCR nude mice (nu/nu), 4-6 weeks of age (AntiCancer Inc., San Diego, CA, USA), were used in this study. Mice were kept in a barrier facility under HEPA filtration. Mice were fed with an autoclaved laboratory rodent diet. All animal studies were conducted in accordance with the principles and procedures outlined in the NIH Guide for the Care and Use of Laboratory Animals under assurance number A3873-1.
Craniotomy open window. Mice were anesthetized with a ketamine mixture (10 μl ketamine HCI, 7.6 μl xylazine, 2.4 μl acepromazine maleate, and 10 μl H2O) via s.c. injection. After fixing the mice in a prone position, a 1.5-cm incision was made directly down the midline of the scalp and the scalp was retracted and the skull was exposed. A 4-mm diameter craniotomy was made over the right parietal bone using a skin biopsy punch (Acuderm Inc., Ft. Lauderdale, FL, USA) and the scalp incisian was sutured closed. Only scalp retraction via a small incision was needed in order to subsequently image single cancer cells in the brain. The incision was then closed with a 6-0 surgical suture (ETHICON, Inc., Somerville, NJ, USA). All mice were kept in a warmed oxygenated chamber until they recovered from ketamine anesthesia described above (9).

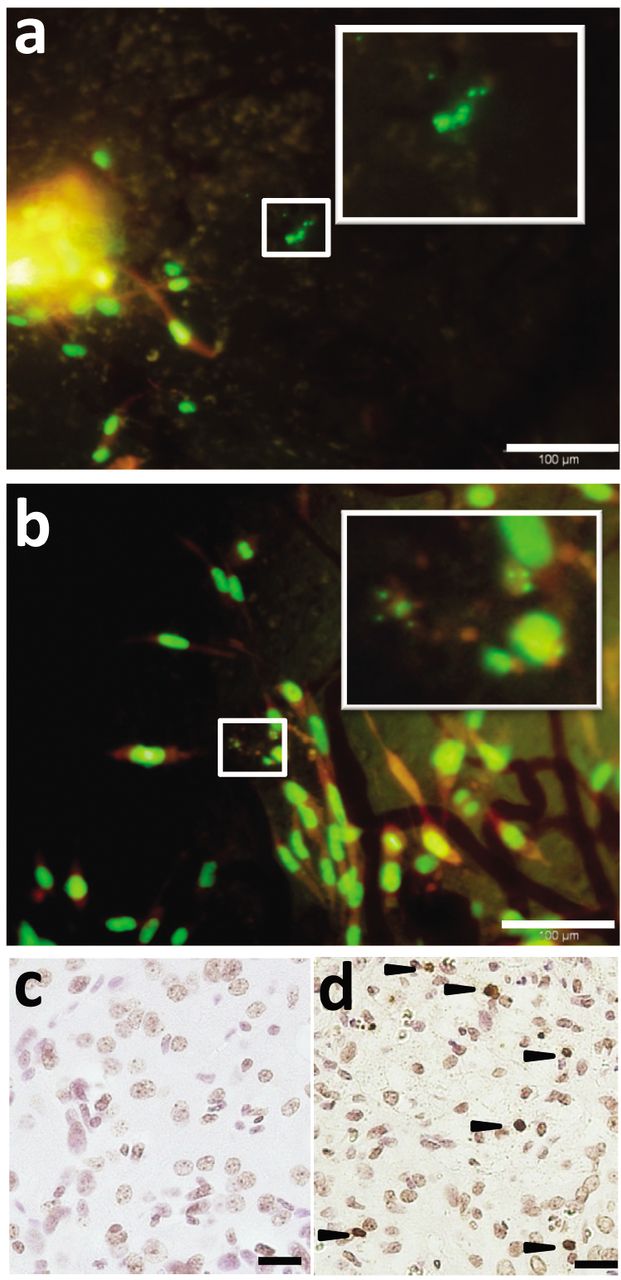
Real-time imaging of apoptotic cell death in the brain in live mice. Seven days after stereotactic injection of dual-color U87 cells, mice were treated daily with temozolomide (100 mg/kg, i.p.), for five days. Apoptotic cells were observed 10 days after treatment. a: Fragmented green fluorescent protein (GFP)-expressing nuclei of dual-color U87 cells were visualized in the brain of a live mouse. b: GFP-expressing apoptotic bodies and destruction of red fluorescent protein (RFP)-expressing cytoplasm of dual-color Lewis lung carcinoma (LLC) cells were visualized in the brain in a live mouse (representative images were chosen from four mice with each cell line). c, d: The terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay was used to confirm the presence of apoptotic DNA fragmentation in U87 glioma cells in the brain of mice treated with temozolomide. c: Non-treated U87 glioma tumor in the brain of mice. d: TUNEL-positive nuclei are indicated by a dark-brown stain in U87 glioma cells in mice treated with temozolomide (arrowheads).
Internal carotid artery injection of cancer cells. Dual-color LLC cells (1×106 cells in 20 μl) were slowly injected with a 31-gauge needle into the right internal carotid artery which then was pressed with a swab to prevent bleeding or leakage of injected cancer cells. The skin was closed with a 5-0 surgical suture (ETHICON, Inc.). The ketamine solution described above was used for anesthesia (9).
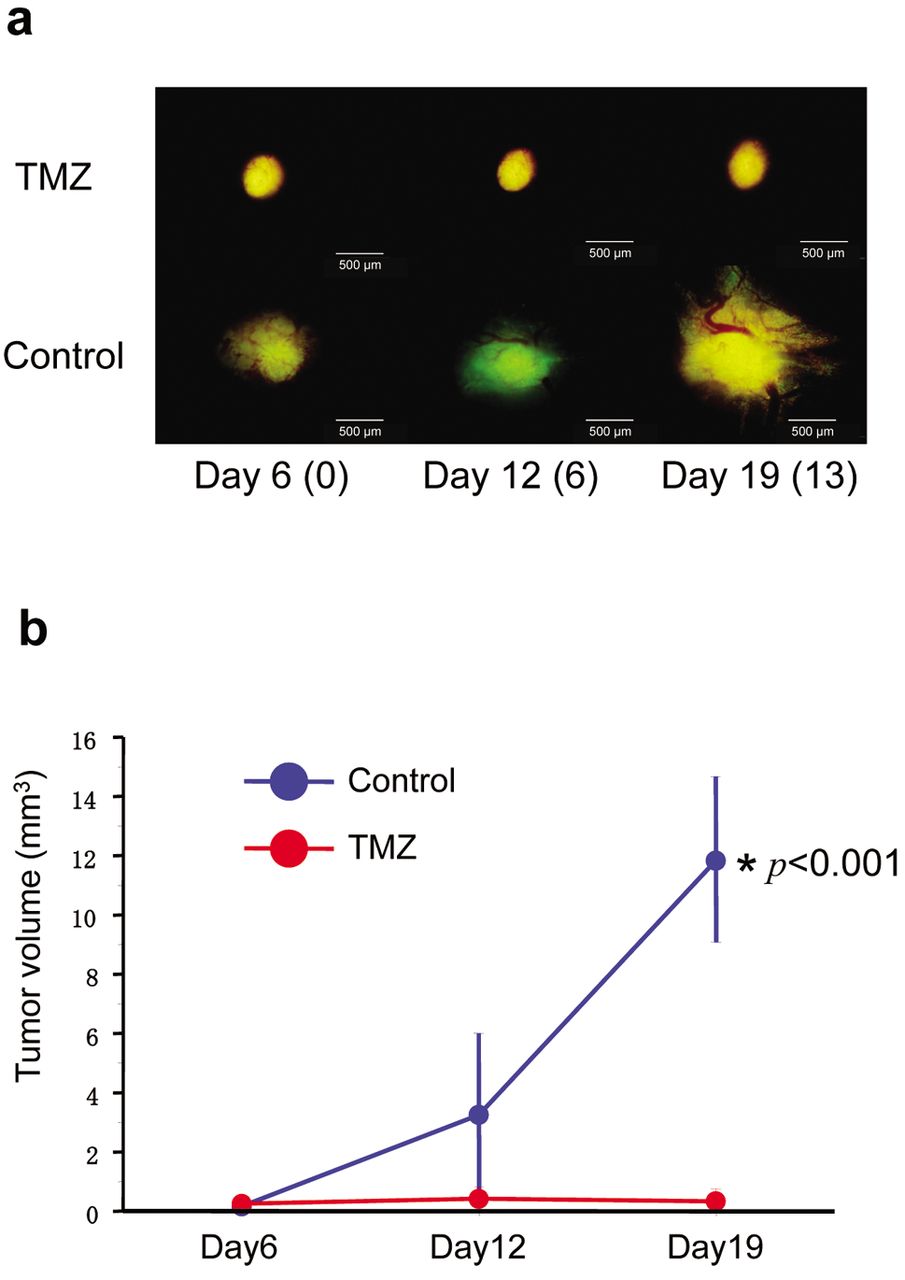
Efficacy of temozolomide (TMZ) on dual-color U87 glioma tumor growth in the brain. a: Representative images of tumor growth in the treatment group on days 6, 12, and 19 after tumor inoculation are shown. U87 cells were injected stereotactically. The number of days after treatment are shown in parentheses (scale bars=500 μm). b: The tumor volume of temozolomide-treated mice and untreated mice (as a control) was compared. Tumor volume in the treated group was significantly smaller than that in the control group (at day 19, p<0.001). Five mice were used in each group. The experimental data are expressed as the mean ± SD. Statistical analysis was performed using the Student's t-test. (p-values: day 6: 0.831, day 12: 0.085, day 19: <0.001).
Stereotactic injection of cancer cells into the brain. The craniotomy open window described above was used as a port to inject 1 μl, containing 1×105 dual-color U87 cells with a 10-μl Hamilton syringe (9).
Fluorescence imaging. An Olympus OV100 Small Animal Imaging System (Olympus Corp., Tokyo, Japan), containing an MT-20 light source (Olympus Biosystems, Planegg, Germany) and a DP70 CCD camera (Olympus), was used for imaging cancer cells in the brain of live mice and brain cross-sections (10).
Chemotherapy of cancer cells in the brain. Temozolomide was obtained from LKT Laboratories (St. Paul, MN, USA). Seven days after tumor-cell inoculation, mice were treated with temozolomide (100 mg/kg, i.p.) daily for five days. Temozolomide was dissolved in 30% dimethyl sulphoxide and 70% normal saline. The dose was determined from previous reports (4, 11, 12).
Terminal deoxynucleotidyltransferase-mediated deoxyuridine triphosphate nick-end labeling (TUNEL) assay. Apoptotic cancer cells were labeled using an in situ cell death detection kit, POD (Roche Diagnostics, Indianapolis, IN, USA) according to the manufacturer's instructions. Staining was achieved using 3,3’-diaminobenzidine tetrahydrochloride (Wako Pure Chemicals, Osaka, Japan). Subsequent to TUNEL staining, sections were counterstained with hematoxylin.
Statistical analysis. The experimental data are expressed as the mean ± SD. Statistical analysis was performed using the Student's t-test or the Kruskal-Wallis test. A p-value of less than 0.05 indicates a significant difference.
Results
Real-time imaging of temozolomide-induced apoptotic cancer cell death in the brain. To induce apoptotic cell death in the brain, mice were treated with temozolomide. The efficacy of temozolomide on cancer cells in the brain was determined by observation of apoptotic cancer cells and tumor colony growth inhibition over time through the craniotomy open window (Figure 1). Apoptotic U87 and LLC cells were observed through the craniotomy open window 10 days after treatment with temozolomide (100 mg/kg i.p. for five consecutive days) (Figure 1a and b). Dual-color U87 cells with fragmented nuclei were visualized (Figure 1a). GFP-expressing apoptotic bodies and destruction of RFP-expressing cytoplasm were also visualized (Figure 1b). In addition, the TUNEL assay was used to confirm apoptosis visualized by imaging the behavior of GFP-labeled cancer cell nuclei. Dark brown-stained U87 nuclei, indicating apoptosis with the TUNEL assay, were detected in the brain tumor in mice which were treated with temozolomide (Figure 1c and d).
Efficacy of temozolomide on dual-color U87 glioma tumor growth in the brain was determined. Tumor growth was imaged on days 6, 12, and 19 after inoculation of U87 cells. Tumor volume in the treated group was significantly smaller than in the control group (at day 19, p<0.001) (Figure 2).
Discussion
We have developed a novel mouse brain imaging model in which cancer cells in the brain can be observed at the subcellular level in live mice. The dual-color cancer cells, craniotomy open window and Olympus OV100 imaging system, all used in the present study, enabled longitudinal real-time subcellular nuclear-cytoplasmic dynamic imaging of cancer cells in the brain over a two-week period. With this imaging technology, we were able to observe, under very high resolution, nuclear and cytoplasmic dynamics of temozolomide-induced apoptosis of cancer cells in the brain as well as tumor colony growth. Temozolomide is an oral alkylating agent that crosses the blood–brain barrier, achieving effective concentrations in the CNS (13, 14). Apoptotic cancer cells were not observed in the untreated mouse brain.
This model can be used to evaluate new modalities for treatment of brain metastases or brain cancer at the subcellular level and opens up new possibilities for such treatment.
Acknowledgements
These studies were supported in part by National Cancer Institute grant CA132971.
Footnotes
-
Conflicts of Interest
None of the authors have a conflict of interest in regard to this study.
- Received October 25, 2012.
- Revision received November 16, 2012.
- Accepted November 19, 2012.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Color-coded Live Imaging of Heterokaryon Formation and Nuclear Fusion of Hybridizing Cancer Cells
- Use of {alpha}v Integrin Linked to Green Fluorescent Protein in Osteosarcoma Cells and Confocal Microscopy to Image Molecular Dynamics During Lung Metastasis in Nude Mice
- The Use of Living Cancer Cells Expressing Green Fluorescent Protein in the Nucleus and Red Fluorescence Protein in the Cytoplasm for Real-time Confocal Imaging of Chromosome and Cytoplasmic Dynamics During Mitosis
- Early Reporting of Apoptosis by Real-time Imaging of Cancer Cells Labeled with Green Fluorescent Protein in the Nucleus and Red Fluorescent Protein in the Cytoplasm
- Dynamic Subcellular Imaging of Cancer Cell Mitosis in the Brain of Live Mice