


Abstract
Background: We investigated patient positioning during radiosurgery of cranial lesions, and calculated clinical target volume (CTV) to planning target volume (PTV) margins using a modified common margin recipe. We simulated CTV-to-PTV margins for reduced image guidance, and repositioning for the first table angle only. Patients and Methods: Patients were immobilized with a thermoplastic mask. Positioning was verified and corrected using the ExacTrac/Novalis Body. Each patient was repositioned before each beam. A common margin recipe was adapted for estimation of CTV-to-PTV margins. Necessary margins were estimated to correct positioning for the initial table angle only in comparison. Results: In total, 269 radiosurgery treatments with 967 different-angle setups (mean 3.6 different angles) were performed on 190 patients. Residual translational errors were (one standard deviation) 0.3 mm in left-right (LR), superior-inferior (SI), and anterior-posterior (AP) directions, with a mean three-dimensional vector of 0.5 mm. Margins for residual errors after correction were calculated in LR, SI, and AP directions as 0.8 mm. For simulated reduced frequency setup correction, we calculated CTV-to-PTV margins as 1.9, 1.9, and 1.6 mm, respectively. Conclusions: The ExacTrac/Novalis Body system allows for accurate positioning of the patient with a residual error comparable to invasive mask fixation. If verification is only performed after initial positioning, adaption of CTV-to-PTV margins should be considered.
Frameless linac-based image-guided radiosurgery (SRS) has, currently, a significant role in the treatment of cranial lesions, including primary brain tumors, brain metastases and functional disorders of cranial nerves. The recent paradigm changes in oncological practice including more individualized and focused treatment for any individual patients requires, from the technical perspective highly sophisticated infrastructures. It needs, indeed, safe and effective SRS that is supposed to minimize normal tissue toxicity by employing sharp dose gradients which must be placed accurately at the margins of the tumor and, simultaneously, to be tumor-effective (1). This dynamics of technology and of concepts in the past decade has made it important to optimize patient comfort and treatment efficacy. The implementation of image-guided stereotactic localization using either optical image guidance (2), or stereoscopic X-ray imaging has provided the use of frameless SRS. The ExacTrac/Novalis Body using dual floor-mounted kilovolt (κV)X-ray tubes, generates stereoscopic oblique images through the gantry's isocenter. It creates an image fusion of the images with a digital reconstructed radiograph (DRR) library generated at the time of planning and generates a predicted position shift to place the patient such that the target is coincident with the planning isocenter. An infrared tracking system is used to verify relative shifts and to provide the initial patient position (3). Additionally, a frameless setup it is more convenient for the patient and demands fewer logistic resources. Frameless linac-based image-guided radiosurgery (SRS) is becoming a good alternative to the frame-based settings in clinical terms (4). However, the thermoplastic masks used facilitate intrafractional movement of the patient's head inside the immobilization mask and increase the magnitude of positional errors compared with frame-based SRS, which is presumably a major source of geometrical uncertainty. To counteract this, a certainty margin should be implemented around the target lesion. While the clinical target volume (CTV) is a clinical concept with respect to the possible extension of a tumor, the planning target volume (PTV), surrounding the CTV, is supposed to be an additional security measure to counteract inter- and intrafractional motion of the tumor and of the patient. This set-up margin emerges as a relevant issue to be understood and studied well.
Table rotations usually two to five angles are required in nearly all radiosurgical procedures, although they can also induce positioning errors. Because image guidance corrects patient intrafractional misplacements, usually before each radiation beam is initiated (4), the geometrical error can be reduced to a sub-millimeter range. However, in the case of fractionated stereotactic radiotherapy (FSRT), for example, the increased frequency of verification images is costly, and time constraints may be necessary to reduce both patient discomfort and intrafractional motion. Alternatively, image guidance performed only considering the initial angle could be considered. To reduce CTV-to-PTV margin to a minimum, it is essential to ensure that the coverage delivered to the patient is precisely as planned.
Since we implemented the image guidance system ExacTrac/Novalis Body (Brain LAB AG, Feldkirchen, Germany) in clinical practice, the question of adequate margins became essential to the quality of patient care in terms of accuracy, safety and outcome. The present study critically evaluated the modification of a common standard margin recipe and calculated the necessary CTV-to-PTV margin for SRS and FSRT with and without imaging at each subsequent table angle.
Patients and Methods
An update of the existing unit to the Novalis SD 5.03 ExacTrac/Novalis Body system was installed at our institution. In addition, a the Robotic Tilt Module™ was mounted underneath the Varian Exact Couch™ top (Varian Medical Systems, Milpitas, CA, USA), allowing for translational and rotational setup corrections. In this protocol, setup accuracy was evaluated in 269 treatment sessions in a consecutive non-randomized cohort of 190 patients undergoing definitive single-fraction SRS for cranial lesions.
The treatment procedure has been described previously in detail (5, 6), and was applied without significant changes. Treatment-planning computed tomography (Siemens, Erlangen, Germany) was performed at 1.25-mm intervals, followed by stereotactic localization. The typical treatment plan consisted of two to seven non-coplanar arcs, or three to 20 convergent-shaped beams. Irradiation times ranged from 12 to 20 min per lesion for most lesions. Doses between 12 and 26 Gy were prescribed, usually to the 80% isodose line covering. Conformal arc or conformal-field radiotherapy were delivered with a 6-MV photon beam through a m3™ mini-multileaf collimator (Novalis™; BrainLAB AG).
The ExacTrac repositioning system has also been described previously (5-7). After infrared-guided patient setup, an initial pair of two non-coplanar oblique isocentric (stereoscopic) kV X-ray images of the skull's bony structures was acquired using two amorphous silicon detectors. A set of shift and rotational corrections was calculated (8), and the patient's position was corrected in cases that exceeded the preset tolerance limits of the system (0.7 mm for translation and 1° for rotation) otherwise, treatment was started. The process of κV imaging with table shift correction was repeated until reaching linear offsets within the limits. Typically, only one additional shift iteration was needed to position the target accurately after positioning. Positioning was verified after each table rotation within the treatment session, and corrected again, if necessary.
To calculate margins, we grouped two types of verification data. The pre-beam correction data represented the residual errors, which remained before treatment was started for the respective field. The pre-fraction correction data consisted of the residual error of the initial field and the first uncorrected displacement error after each table rotation (within or above treatment limits), to simulate reduced frequency verification.
Errors were recorded on the basis of different treatments for different patient positions within each treatment. Errors were calculated separately for the pre-beam and the pre-fraction data groups. The group systematic error (μ) was obtained as the mean of all treatment means, with the standard deviation of the systematic error (Σ) equal to the SD of all means over all treatments. The treatment random error was the root mean square of the random errors of all positions, with the group random error (Σ) equal to the SD of all treatment random errors.
To calculate the margin width around the target volume, we used the prescription suggested by van Herk (9). This margin recipe is verified for multifraction treatments with positioning errors varying daily. In the present study, we adapted this margin recipe for single-fraction treatments by considering positioning errors varying between table rotations. According to van Herk et al., the margin around the CTV should be the sum of 2.5-times the SD of the systematic error (Σ) and 0.7-times the SD of the random error (Σ) (9).
In our study, the margin recipe had to be modified (9, 10). Because doses in the present study were prescribed to the 80% isodose line, the random variation term was to be approximated by 0.4-times Σ. Given that the number of table rotations per treatment was comparably small (mean=3.6 rotations per treatment), an additional systematic error term was applied. The SD of the random error divided by the square root of the mean number of table rotations had to be combined in a quadratic way with the SD of the systematic errors.
Statistical analysis was performed using JMP v7 (SAS Institute, Cary, NC, USA) and R version 2.14.0 (R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org). Descriptive parameters are provided as mean, SD, minimum, and maximum. Translational deviations are depicted as scatterplots with 95% confidence regions.
Results
A non-randomized, consecutive cohort of 190 patients representing 269 radiosurgical treatments (corresponding to 269 isocenters) was analyzed. There was an average of 1.4 treatments per patient (range=1-16), reflecting different isocenters. The mean number of couch positions per treatment was 3.6 (range=2-22). In total, 1,710 error measurements were performed, including 269 pairs of images after pre-positioning, 967 pairs of verification images, and 474 additional correction images.
Overall, 698 table rotations were performed. After 363 (52%) table rotations, the first pair of verification X-rays showed that no localization error exceeds the limits. For the remaining 335 table rotations, one or more corrections were necessary. The mean number of table rotation correction steps was 1.5 (range=1-7).
Pre-beam correction data. Average residual translational and rotational deviations (mean, overall SD, minimum, and maximum), as well as systematic and random errors for all 967 setups after X-ray–guided corrections of all displacements exceeding the limits (0.7 mm, 1°).
Simulated prefraction correction data for prefraction positioning correction only. Average translational and rotational deviations (mean, overall SD, minimum, and maximum), as well as systematic and random error for all 967 setups after X-ray-guided corrections of only the initial displacement exceeding the limits (0.7 mm, 1°).
For the pre-beam correction data group, the residual deviations for translation and rotation after six-dimensional corrections resulting in deviations within the preset limits are presented in Table I and Figure 1 A-C. The SD of residual translational errors was low with 0.3 mm in each direction and a mean variation of 0.5 mm. The rotational residual errors were (1 SD) 0.3° each.
For the pre-fraction correction data group, translational and rotational errors for all 967 setups are presented in Table II and Figure 1 D-F. By contrast, the SDs of displacements were more than doubled (0.6-0.7 mm, respectively), with a mean variation of 0.9 mm. The rotational errors remained low: (1 SD) 0.4° - 0.5° each.
Necessary clinical target volume-planning target volume margins for 967 treatments. Margins after X-ray-guided corrections of all displacements exceeding the limits (0.7 mm, 1°) and of only the initial angle displacements exceeding the limits (0.7 mm, 1°).
For CTV-PTV margins, calculated as described, please refer to Table III. From residual errors in the pre-beam group, we estimated margins of 0.8 mm in all three directions (Table III). Without corrections after table rotation to achieve a new angle in the pre-fraction group (verifying only the initial angle), the margins would have been nearly doubled to 1.6-1.9 mm (Table III).
Calculating CTV-to-PTV margins as described in the unmodified recipe, we would have estimated 0.7 mm in all directions, respectively, for the pre-beam group and 1.6, 1.7, and 1.4 mm, in LR, SI and AP respectively, for the pre-fraction group, and would have underestimated the CTV-TO-PTV margins by approximately 15%.
In 94 out of 269 treatments (35%), translational deviations exceeding the preset limits were recorded after each table rotation. The necessary CTV-to-PTV margins for this subset of cases were even higher: 3.0, 3.0, and 3.1 mm in LR, SI, and AP directions, respectively.
Discussion
The question of an adequate margin definition from CTV to PTV during the delivery of SRS or FSRT for cranial lesions remains important, while attempts are made to change so-called standards. Residual errors were evaluated by Verbakel et al. (11). For 135 fractions, translational deviations of (1 SD) 0.2, 0.3, and 0.3 mm were observed in LR, SI, and AP directions, respectively, which our results confirm. In 109 stereotactic radiosurgery and 166 stereotactic radiotherapy treatments, Ackerly et al. reported means of translational errors of approximately 0.3, 0.3, and 0.2 mm in LR, SI, and AP directions, respectively, for FSRT and 0.4, 0.4, and 0.3 mm, respectively, for SRS (12), which our results compare well with. These data demonstrate that the 6-dimensional fusion-based, image-guided localization for patient setup is clinically reliable, and features localization accuracy similar to that of the phantom study conducted by Jin et al. (8), with translation errors (1 SD) of 0.2 to 0.3 mm. Our data for rotational errors are comparable with these of Gevert et al. (13), which were (1 SD) 0.35°, 0.31°, and 0.33°, respectively.
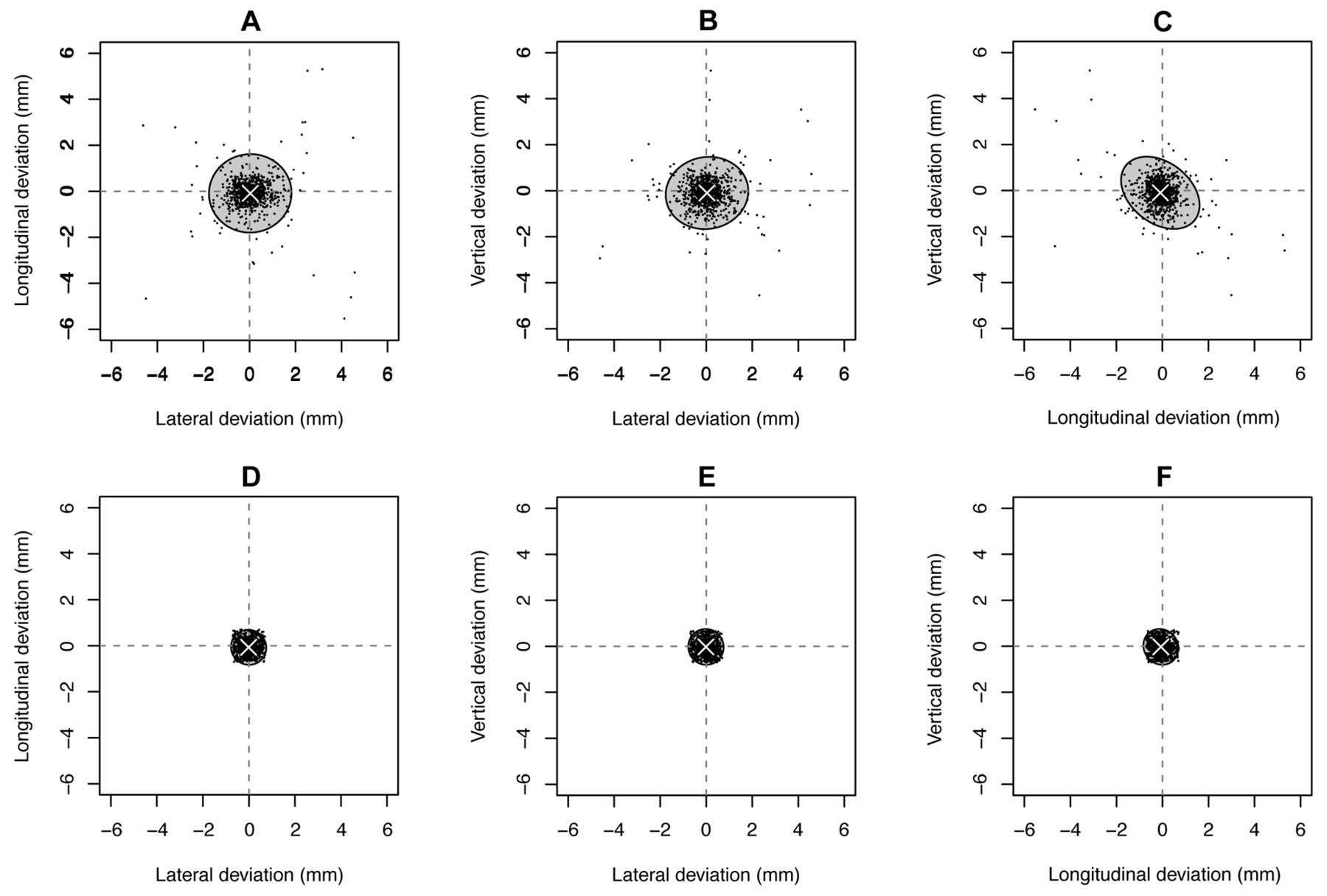
Scatter plots with mean (cross) and 95% confidence regions of translational deviations for all 967 setups for the pre-fraction group (A-C) with correction of only the initial angle, and the pre-beam group (D-F) leaving only residual errors (0.7 mm, 1°) uncorrected.
The treatment duration of approximately 15 min suggests that pre- and post-treatment imaging is not a sensitive method with which to assess intrafractional target motion. Ramakrishna et al. published data obtained with pre- and post-treatment imaging for 110 treatments, and observed a mean shift of 0.7 mm (1 SD, 0.5 mm) (6), which differ from our data. Verbakel et al. reported data for 79 fractions with a mean shift of (1 SD) of 0.2 mm (11), lower than our results.
In our study, necessary CTV-to-PTV margins resulting from residual error would be 0.8 mm in all directions. Published data for treatment margins are sparse, especially in the context of single-fraction SRS. For FSRT with the BrainLAB mask system, Gevaert et al. recommended margins of 1.4, 2.8, and 2.0 mm in LR, SI, and AP directions, respectively, for the head and neck mask without intrafractional image guidance (14), and our values of 1.9, 1.9, and 1.6 compare well with these suggestions.
One limitation of this study is that van Herk's margin recipe is derived from probability calculations based on conformal radiotherapy with standard fractionation, and estimates the accuracy of target volume delineation by incorporating random errors and systematic errors. It is obvious that CTV-to-PTV margins calculated on the basis of different days and different table positions, respectively, must be compared carefully. However, margins calculated with the common formula versus the SRS-adapted formula are in a similar range. Therefore, we conclude that this approach is appropriate.
To our knowledge, the clinical consequences of enlarged intracranial safety margins have been evaluated for radiosurgery only. After enlarging the CTV-to-PTV margin from 1 mm to 2 mm, Nataf et al. noted more severe parenchymal complications (p=0.02) in a group of 93 patients with brain metastases (15). For FSRT, this finding may be important with respect to the close vicinity of structures at risk.
In summary, our results compared well with other data collected using the ExacTrac/Novalis Body system. For SRS, we calculated CTV-to-PTV margins of 0.8 mm in all three directions. Otherwise, if verification and correction are only performed after initial infrared pre-positioning, we would suggest institutional-based adaption of CTV-to-PTV margins in the dimension of 2 mm.
Footnotes
-
Conflicts of Interest
All Authors confirm that there is no conflict of interests to any financial and personal relationships with other people or organization.
- Received July 20, 2013.
- Revision received September 10, 2013.
- Accepted September 12, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}