


Abstract
Background: The benefits of adjuvant chemotherapy for completely resected non-small cell lung cancer (NSCLC) have been demonstrated using mainly cisplatin (CDDP)-based chemotherapeutic regimens. However, treatment-related deaths sometimes occur. Therefore, the development of a safer regimen is necessary. Patients and Methods: The patients were randomized to either carboplatin (CBDCA) area under the curve (AUC) 3 and paclitaxel (PTX) 90 mg/m2 (PCb arm) or CBDCA (AUC3) plus gemcitabine (GEM) (1000 mg/m2) (GCb arm) every 2 weeks for 8 cycles after surgery. The primary endpoint was the compliance with the regimen, while the secondary endpoints were safety and toxicity. Results: A total of 75 patients were enrolled in a multi-institutional study. Twenty-one out of 39 patients (54%) in the PCb arm and 25 of 36 patients (69%) in the GCb arm completed 8 cycles, and 59% in the PCb arm and 81% in the GCb arm completed ≥6 cycles. The predominant toxicity was neutropenia. Non-hematological adverse effects were infrequent and no treatment-related death was registered. The estimated disease-free survival and overall survival at 2 years were 70.8% and 66.3% in the PCb and 91.4% and 79.1% in the GCb arm, respectively. Conclusion: This adjuvant bi-weekly scheduled chemotherapy resulted in good compliance in both arms, and the regimen was feasible, with acceptable levels of toxicity in completely resected Japanese NSCLC patients. Therefore, these regimens represent a new treatment option suitable for outpatients with completely resected NSCLC.
Approximately 30% of all patients with non-small cell lung cancer (NSCLC) demonstrate a recurrence of the tumor despite undergoing a complete surgical resection (1). This suggests that occult metastases are often present at the time of surgical intervention (2). Therefore, adjuvant chemotherapy is needed to improve the prognosis of patients (3). The benefits of adjuvant chemotherapy have been demonstrated using mainly cisplatin (CDDP)-based chemotherapy (4). However, many problems still remain. For example, an inpatient setting is required over a long duration to achieve safe treatment of patients without good drug compliance. Furthermore, treatment-related deaths sometimes occur with CDDP chemotherapy, even though it might prevent recurrence in an adjuvant setting (5). In addition, CDDP-based chemotherapy yields a barely significant survival advantage compared with combination chemotherapy consisting of carboplatin (CBDCA) plus a second-generation agent in patients with advanced NSCLC (6).
We previously reported that a protocol of CBDCA combined with paclitaxel (PTX) also had acceptable toxicity in the adjuvant setting (7). On the other hand, a recent meta-analysis showed the superiority of gemcitabine (GEM)-containing regimens among other regimens for the treatment of advanced NSCLC (8). In fact, CBDCA with GEM has proven to be one of the best regimens for advanced NSCLC, with definite anticancer efficacy (9). Therefore, CBDCA with GEM may offer an acceptable alternative for patients with advanced NSCLC. However, severe thrombocytopenia was frequently observed with the tri-weekly schedule of CBDCA (AUC 5) with GEM (10). Therefore, the schedule of this regimen still needs improvement. Mancuso et al. reported that a biweekly regimen of CBDCA with GEM has a manageable toxicity profile without thrombocytopenia (11).
The purpose of this study was to test the completion rate as a primary endpoint and the adverse events (AE) and disease-free survival (DFS) as secondary endpoints in patients with stage IB-III NSCLC receiving bi-weekly carboplatin (CBDCA) area under the curve (AUC) 3 and paclitaxel (PTX) 90 mg/m2 (PCb arm) versus CBDCA (AUC3) plus gemcitabine (GEM) (1000 mg/m2) (GCb arm) in a multi-institutional study.
Patients and Methods
Eligibility criteria. Patients were eligible for the main trial if they fulfilled the following local criteria for pathologic diagnosis of stage IB, II, IIIA, or IIIB (pm1) NSCLC (12) after a curative lobectomy and a systematic mediastinal lymphadenectomy: age 20-80 years; Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 or 1; a leukocyte count of 4,000 mm3 and a neutrophil count of 2,000 mm3 or greater; hemoglobin level 9.5 g/dl or greater; a platelet count of 100,000 μl or greater; a serum bilirubin level less than 1.5 mg/dl; aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels equal to or less than 2 times the institutional normal, and creatinine less than 1.5 mg/dl. The patients were ineligible if they had a concurrent malignancy, uncontrollable complications, severe post operative morbidity; previous treatment including chemotherapy, radiotherapy, or immunotherapy, hypersensitivity to therapeutic agents; the possibility of being pregnant, and other conditions such as hepatic inflammation, as judged by the attending physician.
Treatment schedule and trial design. This was a multi-institutional prospective study. Patients with completely resected stage IB-IIIB NSCLC were randomized to either CBDCA (AUC3) plus PTX (90 mg/m2) (PCb arm) (12) or CBDCA (AUC3) plus GEM (1,000 mg/m2) (GCb arm) (13), bi-weekly for 8 cycles within 8 weeks after surgery, mainly in an outpatient setting. Calvert's formula was used to calculate the dose of the AUC for CBDCA (14), whereas the creatinine clearance was determined with the Jellifie formula (15). A short pre-treatment with 20 mg of dexamethasone, 5 mg of D-chlorpheniramine maleate and 50 mg of ranitidine was administered intravenously 30 minutes before the patients received PTX. A short pre-treatment with 8 mg of dexamethasone was administered intravenously 30 minutes before administration of GEM. CBDCA and PTX or GEM were administered by intravenous drip infusion over 30 min and 60 min, respectively.
Complete blood cell counts were measured before the beginning of a new treatment course. Treatment was delayed 1 week if the leukocyte count was less than 3000 μl or the platelet count was less than 75,000 μl. The patient was withdrawn from the study if these conditions were not resolved within 1 week. The dose of PTX was reduced to 80 mg/m2 and 800 mg/m2 of GEM, and the dose of CBDCA was reduced to AUC 2.5 only once through a full course when the neutrophil count was 1,000/μl or less, the patient had a fever of 38.0°C or higher, or the platelet count was 25,000/μl or less with previous treatment, or grade 3 non-hematological toxicities occurred. The therapy was terminated when grade 4 non-hematological toxicities occurred. The maximum grade on the NCI Common Toxicity Criteria for Adverse Events (AEs) was reported for hematological and non-hematological toxic effects (16). Patients did not receive prophylactic granulocyte colony-stimulating factor (G-CSF) during any cycle. The criteria for removal from the treatment arm was intolerable toxicity or withdrawal of consent. The choice of any subsequent treatment depended on the institution. The Institutional Review Board approved this study and informed consent was obtained from either the patients or from their legal guardians.
Observations and evaluations. The primary endpoint of this study was compliance with the chemotherapy protocol, while the secondary endpoints were AEs and DFS. All eligible patients who received any treatment were considered assessable for toxicity. The blood chemistry studies and serum levels of tumor markers were repeated every 2 cycles. DFS was calculated from the date of enrollment to the date of documented progression. Overall survival (OS) was calculated from the date of enrollment to the date of death or last known contact. The follow-up periods after accrual closure were 12 and 24 months.
Statistical analysis. The expected and threshold values of the treatment completion rate were 76 and 50%, respectively (7). The number of patients required was determined with an α risk of 0.05 and β risk of 0.1. Simon's optimal design was applied to recruit the patients (17) and the number of the patients in each arm was calculated to be 35 patients considering the cases with incomplete treatment. If completion of treatment was observed in <7 patients among the first 14 patients, this study was to be terminated; if it was observed to be ≥8 patients, recruitment of as many as 62 patients was allowed. The events considered in the DFS were locoregional and distant recurrence. The Kaplan-Meier method was used to estimate the probability of survival, and survival differences were analyzed by the log-rank test. The terminal event of the overall survival analysis was death attributable to cancer or non-cancer causes. The difference was considered to be significant if the p-value was less than 0.05. The data were analyzed using the Stat View software program (Abacus Concepts, Inc., Berkeley, California, USA).
Results
Patient characteristics. Seventy-six patients were enrolled in this multi-institutional trial from July 2005 to June 207. These patients were randomized, and one patient was excluded due to ineligibility criteria. Therefore, 75 were eligible for intent-to-treat analysis (39 in the PCb and 36 in the GCb arm). The histological types included adenocarcinoma (n=49), squamous cell carcinoma (n=20), large cell carcinoma (n=5), and adenosquamous cell carcinoma (n=1). The pathological stages were IB/IIA/IIB/IIIA/IIIB: 22/9/14/28/2. A total of 75 patients were evaluable. The baseline characteristics and patient disposition for the two groups are summarized in Table I. The study included 48 males and 27 females, with a median age of 65.1 years (range: 23-79 years). None of the patients received induction or postoperative radiotherapy. The patient characteristics in both arms were similar.
Patient characteristics.
Chemotherapy compliance. The regimen was judged to be safe and tolerable in the first stage, and therefore patients were accrued as planned. Twenty-one out of 39 patients (54%) in the PCb arm and 25 out of 36 patients (69%) in the GCb arm completed 8 cycles, and 23/39 (59%) in the PCb arm and 29/36 (81%) in the GCb arm completed ≥6 cycles. The median number of treatment cycles in the PCb and GCb arms was 6.0 and 6.9, respectively. The primary reason for premature discontinuation was hematological toxicity (n=11) (Table II).
Toxicity. The toxicity profiles are summarized in Table III. Severe (grade 3/4) hematological toxicities (%) in the PCb/GCb arm were respectively: neutropenia in 14 (35.9%)/19 (52.8%), anemia in 0/6, and thrombocytopenia in 1/0 of the patients. Severe non-hematological AEs were infrequent, and no treatment-related death was registered.
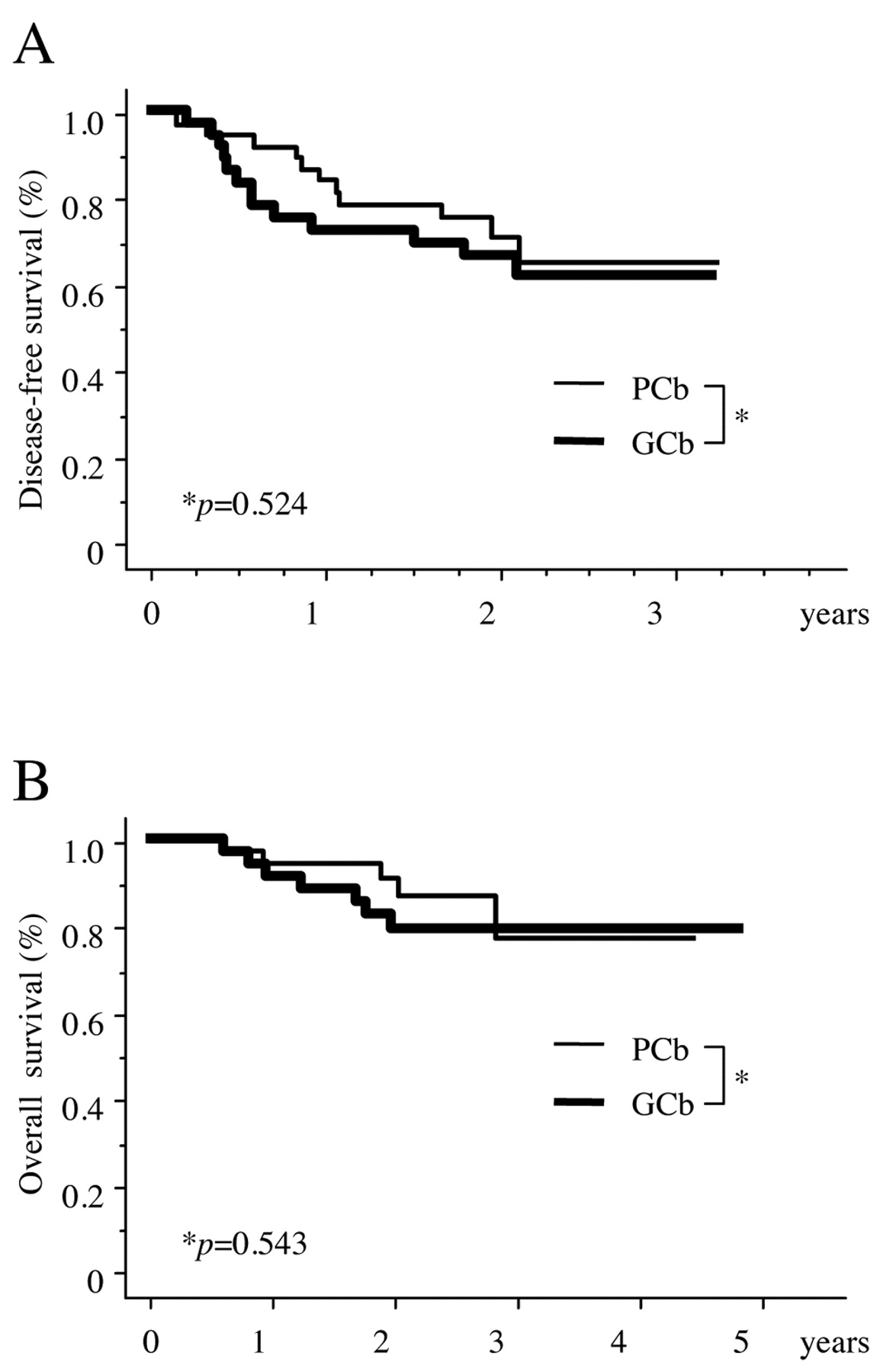
Survival. There were 26 events (14: alive with recurrence, 10: death with recurrence, and 2: death without cancer) in 67 patients. The majority of the sites of tumor recurrence were hematogenous metastases, and recurrence was more frequent in patients with advanced stage disease. The recurrence pattern in both arms was similar (Table IV). The overall median follow-up period for all patients was 28.9 months. The estimated DFS in the PCb and GCb arms at 2 years was 70.8% and 66.3%, respectively (p=0.524) (Figure 1A). The estimated OS in the PCb and GCb arms at 2 years was 91.4% and 79.1%, respectively (p=0.543) (Figure 1B).
Reasons for discontinuation of treatment.
Worst adverse events.
Pathological stage and type of recurrence.

Disease-free (A) and overall (B) survival of patients treated with carboplatin and paclitaxel (PCb) or with carboplatin and gemcitabine (GCb).
Discussion
CDDP-containing regimens pose unacceptable toxicity and require hydration to prevent renal toxicity (5). As a result, these regimens often have low patient compliance in the outpatient setting. On the other hand, CBDCA regimens have been shown to be equally effective, with lower toxicity. At present, various schedules are being evaluated for combination regimens with CBDCA and a third-generation chemotherapeutic agent for the treatment of advanced NSCLC (18). Furthermore, in addition to the differences in the response to different schedules, there might be large differences between chemotherapy for advanced NSCLC patients with a large tumor burden and patients receiving the treatment in the adjuvant setting who are macroscopically tumor-free. Therefore, development of a safe and effective regimen is necessary that is specifically tailored for patients with resected NSCLC. We previously reported that a bi-weekly schedule of CBDCA with PTX was well-tolerated as adjuvant chemotherapy. CBDCA with GEM regimens may offer an acceptable alternative with lower toxicity. Both treatment regimens used in this study are available for outpatients for a short duration of treatment. Additional studies will be needed to determine which is better. This phase II trial assessed the feasibility, safety and efficacy of the two novel outpatient treatment regimens. The compliance of both arms was shown to be relatively good.
In this study, severe neutropenia was observed in 44.0% of patients (33/75). However, the frequency of severe neutropenia in the GCb arm was much higher than in the PCb arm. The frequency of severe neutropenia for a biweekly schedule of CBDCA with PTX has been reported to be only 13% in past series (7). This discrepancy could be related to the small number of patients included in the present study. PTX and GEM have often been reported to cause severe peripheral disorder and thrombocytopenia, respectively (10, 19). However, no severe AEs were observed in either arm. This low level of toxicity might be due to the bi-weekly schedule. Two frequent reasons for premature discontinuation of treatment included pneumonia and cancer recurrence. The pneumonia might have been due to the fact that our study included elderly patients with low function of their intrinsic pulmonary capacity, in addition to the post-operative recovery. Tumor recurrence might be preventable by more aggressive treatment. Thus, selection of regimens with sufficient efficacy for restricting the growth of a recurrence might be needed. Recently, we launched a phase II trial with a tri-weekly schedule of CBDCA with docetaxel for post-operative adjuvant therapy. The 2-year DFS and OS rates were 70.8 and 66.3% in the PCb and 91.4 and 79.1% in the GCb arm, respectively. These data were within the acceptable range, although the data regarding survival are still preliminary.
Conclusion
Adjuvant chemotherapy with a bi-weekly schedule of CBDCA and PTX or GEM was feasible and had acceptable toxicity in Japanese NSCLC patients. In clinical practice, both regimens represent potential treatment options suitable for use on an outpatient basis.
Acknowledgements
We wish to thank Sumi Nakamura for their valuable technical assistance.
- Received September 4, 2010.
- Revision received October 18, 2010.
- Accepted October 19, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- TMPRSS4 Expression as a Marker of Recurrence in Patients with Lung Cancer
- Prediction of Recurrence after Complete Resection in Patients with NSCLC
- The Expression of CD146 Predicts a Poor Overall Survival in Patients with Adenocarcinoma of the Lung
- The EMT Status in the Primary Tumor Does Not Predict Postoperative Recurrence or Disease-free Survival in Lung Adenocarcinoma
- The Expression of Ki-67, but Not Proliferating Cell Nuclear Antigen, Predicts Poor Disease Free Survival in Patients with Adenocarcinoma of the Lung