Clinical Significance of Serum Glutamine Level in Patients with Colorectal Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement of Serum Glutamine Levels
2.3. Measurement of Proinflammatory Cytokine Levels
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
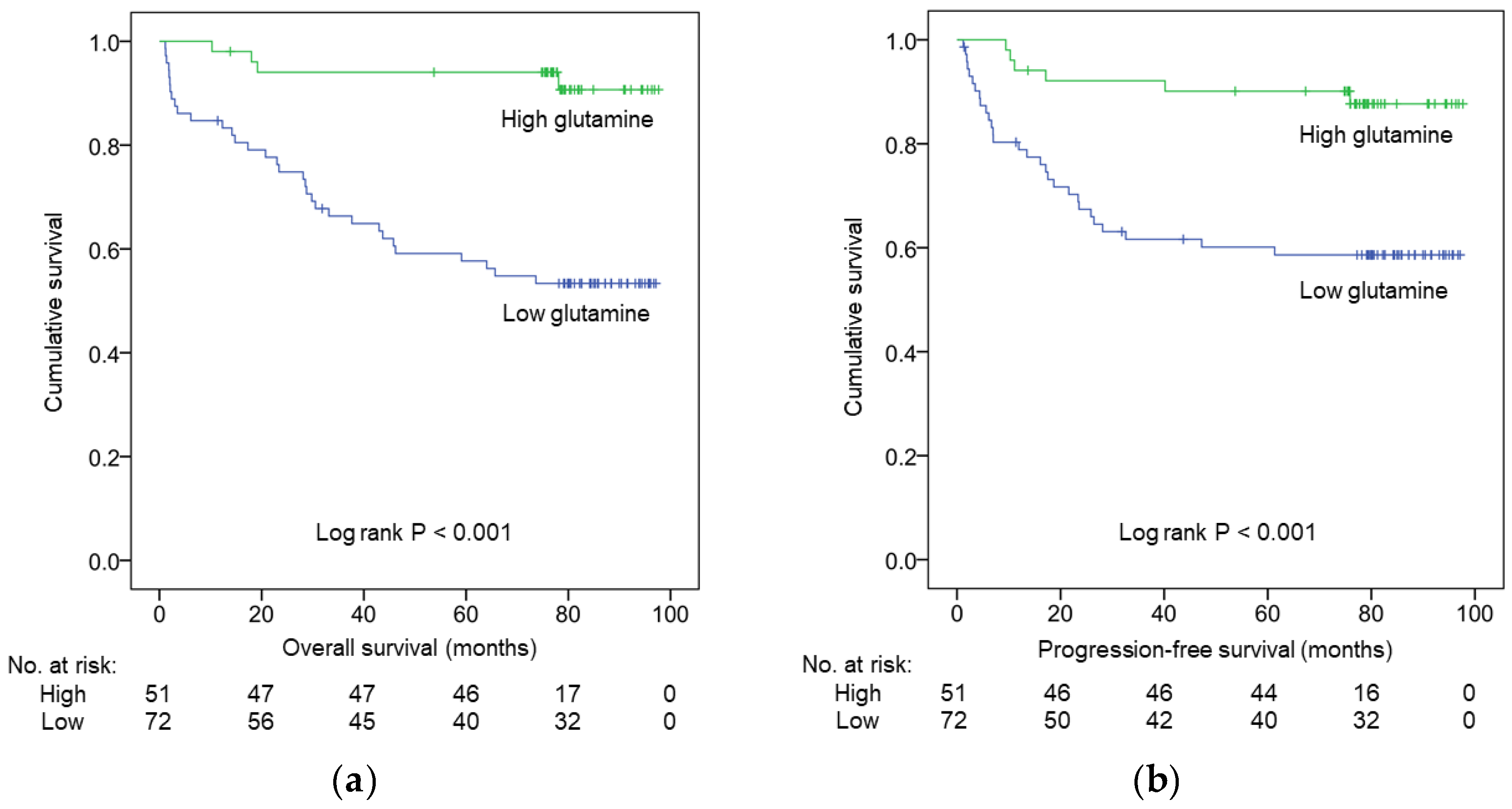
3.2. Survival Analysis
3.3. Prognostic Factors Influencing OS and PFS
3.4. Correlation between Serum Glutamine and Proinflammatory Cytokine Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; Dandona, L.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, M.; Hickey, B.E.; Hider, P.N.; See, A.M. Follow-up strategies for patients treated for non-metastatic colorectal cancer. Cochrane Database Syst. Rev. 2016, 11, Cd002200. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ma, J.; Zhang, S.; Deng, G.; Wu, X.; He, J.; Pei, H.; Shen, H.; Zeng, S. A prognostic analysis of 895 cases of stage III colon cancer in different colon subsites. Int. J. Colorectal Dis. 2015, 30, 1173–1183. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.; Lueza, B.; Douillard, J.Y.; Peeters, M.; Lenz, H.J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.S.; Lin, J.K.; Chiou, T.J.; Liu, J.H.; Fan, F.S.; Yen, C.C.; Lin, T.C.; Jiang, J.K.; Yang, S.H.; Wang, H.S.; et al. Preoperative carcinoembryonic antigen level as an independent prognostic factor in colorectal cancer: Taiwan experience. Jpn. J. Clin. Oncol. 2000, 30, 12–16. [Google Scholar] [CrossRef]
- Dereziński, P.; Klupczynska, A.; Sawicki, W.; Pałka, J.A.; Kokot, Z.J. Amino Acid Profiles of Serum and Urine in Search for Prostate Cancer Biomarkers: A Pilot Study. Int. J. Med Sci. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Plewa, S.; Horała, A.; Dereziński, P.; Klupczynska, A.; Nowak-Markwitz, E.; Matysiak, J.; Kokot, Z.J. Usefulness of Amino Acid Profiling in Ovarian Cancer Screening with Special Emphasis on Their Role in Cancerogenesis. Int. J. Mol. Sci. 2017, 18, 2727. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Ma, X.; Li, H.; Guo, G.; Li, P.; Li, H.; Gu, L.; Li, X.; Chen, L.; Zhang, X. The predictive and prognostic values of serum amino acid levels for clear cell renal cell carcinoma. Urol. Oncol. 2017, 35, 392–400. [Google Scholar] [CrossRef]
- Jing, F.; Hu, X.; Cao, Y.; Xu, M.; Wang, Y.; Jing, Y.; Hu, X.; Gao, Y.; Zhu, Z. Discriminating gastric cancer and gastric ulcer using human plasma amino acid metabolic profile. Iubmb Life 2018, 70, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Nishiumi, S.; Shinohara, M.; Yoshie, T.; Hatano, N.; Okuno, T.; Bamba, T.; Fukusaki, E.; Takenawa, T.; Azuma, T.; et al. Serum metabolomics as a novel diagnostic approach for gastrointestinal cancer. Biomed. Chromatogr. 2012, 26, 548–558. [Google Scholar] [CrossRef]
- Tan, B.; Qiu, Y.; Zou, X.; Chen, T.; Xie, G.; Cheng, Y.; Dong, T.; Zhao, L.; Feng, B.; Hu, X.; et al. Metabonomics Identifies Serum Metabolite Markers of Colorectal Cancer. J. Proteome Res. 2013, 12, 3000–3009. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Djukovic, D.; Deng, L.; Gu, H.; Himmati, F.; Chiorean, E.G.; Raftery, D. Colorectal Cancer Detection Using Targeted Serum Metabolic Profiling. J. Proteome Res. 2014, 13, 4120–4130. [Google Scholar] [CrossRef]
- Bertini, I.; Cacciatore, S.; Jensen, B.V.; Schou, J.V.; Johansen, J.S.; Kruhøffer, M.; Luchinat, C.; Nielsen, D.L.; Turano, P. Metabolomic NMR Fingerprinting to Identify and Predict Survival of Patients with Metastatic Colorectal Cancer. Cancer Res. 2012, 72, 356. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Gao, R.; Yan, X.; Qin, H. Research progression of blood and fecal metabolites in colorectal cancer. IJS Oncol. 2018, 3, e51. [Google Scholar] [CrossRef]
- DeBerardinis, R.J.; Cheng, T. Q‘s next: The diverse functions of glutamine in metabolism, cell biology and cancer. Oncogene 2010, 29, 313–324. [Google Scholar] [CrossRef]
- Bergstrom, J.; Furst, P.; Noree, L.O.; Vinnars, E. Intracellular free amino acid concentration in human muscle tissue. J. Appl. Physiol. 1974, 36, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Altman, B.J.; Stine, Z.E.; Dang, C.V. From Krebs to clinic: Glutamine metabolism to cancer therapy. Nat. Rev. Cancer 2016, 16, 749. [Google Scholar] [CrossRef] [PubMed]
- De Vitto, H.; Perez-Valencia, J.; Radosevich, J.A. Glutamine at focus: Versatile roles in cancer. Tumour Biol. 2016, 37, 1541–1558. [Google Scholar] [CrossRef]
- Choi, Y.K.; Park, K.G. Targeting Glutamine Metabolism for Cancer Treatment. Biomol. Ther. 2018, 26, 19–28. [Google Scholar] [CrossRef]
- Wang, L.B.; Shen, J.G.; Zhang, S.Z.; Ding, K.F.; Zheng, S. Amino acid uptake in arterio-venous serum of normal and cancerous colon tissues. World J. Gastroenterol. 2004, 10, 1297–1300. [Google Scholar] [CrossRef] [Green Version]
- Sirniö, P.; Väyrynen, J.P.; Klintrup, K.; Mäkelä, J.; Karhu, T.; Herzig, K.-H.; Minkkinen, I.; Mäkinen, M.J.; Karttunen, T.J.; Tuomisto, A. Alterations in serum amino-acid profile in the progression of colorectal cancer: Associations with systemic inflammation, tumour stage and patient survival. Br. J. Cancer 2019, 120, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Barni, S.; Coinu, A.; Bertocchi, P.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Zaniboni, A. The Modified Glasgow Prognostic Score and Survival in Colorectal Cancer: A Pooled Analysis of the Literature. Rev. Recent Clin. Trials 2015, 10, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Meyerhardt, J.A.; Giovannucci, E.; Jeon, J.Y. Association between body mass index and prognosis of colorectal cancer: A meta-analysis of prospective cohort studies. PLoS ONE 2015, 10, e0120706. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, C.H.; Neugebauer, R.; Meyerhardt, J.; Prado, C.M.; Weltzien, E.; Kwan, M.L.; Xiao, J.; Caan, B.J. Analysis of Body Mass Index and Mortality in Patients With Colorectal Cancer Using Causal Diagrams. JAMA Oncol. 2016, 2, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Shahjehan, F.; Merchea, A.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Kasi, P.M. Body Mass Index and Long-Term Outcomes in Patients With Colorectal Cancer. Front. Oncol. 2018, 8, 620. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.-L.; Chen, H.-H.; Chiu, H.-H.; Chiu, Y.-H.; Hwang, L.-C.; Wu, S.-L. Morbidity associated with overweight and obesity in health personnel: A 10-year retrospective of hospital-based cohort study in Taiwan. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Armitage, E.G.; Barbas, C. Metabolomics in cancer biomarker discovery: Current trends and future perspectives. J. Pharm. Biomed. Anal. 2014, 87, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Farshidfar, F.; Weljie, A.M.; Kopciuk, K.A.; Hilsden, R.; McGregor, S.E.; Buie, W.D.; MacLean, A.; Vogel, H.J.; Bathe, O.F. A validated metabolomic signature for colorectal cancer: Exploration of the clinical value of metabolomics. Br. J. Cancer 2016, 115, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Hensley, C.T.; Wasti, A.T.; DeBerardinis, R.J. Glutamine and cancer: Cell biology, physiology, and clinical opportunities. J. Clin. Investig. 2013, 123, 3678–3684. [Google Scholar] [CrossRef]
- Hao, Y.; Samuels, Y.; Li, Q.; Krokowski, D.; Guan, B.J.; Wang, C.; Jin, Z.; Dong, B.; Cao, B.; Feng, X.; et al. Oncogenic PIK3CA mutations reprogram glutamine metabolism in colorectal cancer. Nat. Commun. 2016, 7, 11971. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Song, P.; Zhu, L.; Aziz, N.; Zhou, Q.; Zhang, Y.; Xu, W.; Feng, L.; Chen, D.; Wang, X.; et al. Synthetic lethality of glutaminolysis inhibition, autophagy inactivation and asparagine depletion in colon cancer. Oncotarget 2017, 8, 42664–42672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Zhu, J.; Yu, M.; Cai, C.; Zhou, Y.; Yu, M.; Fu, Z.; Gong, Y.; Yang, B.; Li, Y.; et al. Glutamate dehydrogenase is a novel prognostic marker and predicts metastases in colorectal cancer patients. J. Transl. Med. 2015, 13, 144. [Google Scholar] [CrossRef]
- Huang, F.; Zhang, Q.; Ma, H.; Lv, Q.; Zhang, T. Expression of glutaminase is upregulated in colorectal cancer and of clinical significance. Int. J. Clin. Exp. Pathol. 2014, 7, 1093–1100. [Google Scholar] [PubMed]
- Feng, X.; Hao, Y.; Wang, Z. Targeting glutamine metabolism in PIK3CA mutant colorectal cancers. Genes Dis. 2016, 3, 241–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Ping, X.; Yu, B.; Liu, F.; Ni, X.; Li, J. Clinical trial: Prophylactic intravenous alanyl-glutamine reduces the severity of gastrointestinal toxicity induced by chemotherapy—A randomized crossover study. Aliment Pharm. 2009, 30, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.S.; Lin, J.K.; Lin, T.C.; Chen, W.S.; Jiang, J.K.; Wang, H.S.; Chiou, T.J.; Liu, J.H.; Yen, C.C.; Chen, P.M. Oral glutamine is effective for preventing oxaliplatin-induced neuropathy in colorectal cancer patients. Oncologist 2007, 12, 312–319. [Google Scholar] [CrossRef]
- Jolfaie, N.R.; Mirzaie, S.; Ghiasvand, R.; Askari, G.; Miraghajani, M. The effect of glutamine intake on complications of colorectal and colon cancer treatment: A systematic review. J. Res. Med. Sci. 2015, 20, 910–918. [Google Scholar] [CrossRef]
- Viana Veloso, G.G.; Franco, O.H.; Ruiter, R.; de Keyser, C.E.; Hofman, A.; Stricker, B.C.; Kiefte-de Jong, J.C. Baseline dietary glutamic acid intake and the risk of colorectal cancer: The Rotterdam study. Cancer 2016, 122, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Heianza, Y.; Huang, T.; Wang, T.; Sun, D.; Zheng, Y.; Hu, F.B.; Rexrode, K.M.; Manson, J.E.; Qi, L. Dietary glutamine, glutamate and mortality: Two large prospective studies in US men and women. Int. J. Epidemiol. 2018, 47, 311–320. [Google Scholar] [CrossRef]
- Klampfer, L. Cytokines, inflammation and colon cancer. Curr. Cancer Drug Targets 2011, 11, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-W.; Karin, M. A cytokine-mediated link between innate immunity, inflammation, and cancer. J. Clin. Investig. 2007, 117, 1175–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, P.H.; Pan, Y.P.; Fan, C.W.; Tseng, W.K.; Huang, J.S.; Wu, T.H.; Chou, W.C.; Wang, C.H.; Yeh, K.Y. Pretreatment serum interleukin-1beta, interleukin-6, and tumor necrosis factor-alpha levels predict the progression of colorectal cancer. Cancer Med. 2016, 5, 426–433. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (n = 123) | Low Glutamine (<52 ng/μL, n = 72) | High Glutamine (≥52 ng/μL, n = 51) | p-Value | ||
|---|---|---|---|---|---|---|
| n | n | % | n | % | ||
| Age (years) | <0.001 | |||||
| <65 | 52 | 21 | 29.20% | 31 | 60.80% | |
| ≥65 | 71 | 51 | 70.80% | 20 | 39.20% | |
| Sex | 0.077 | |||||
| Male | 78 | 41 | 56.90% | 37 | 72.50% | |
| Female | 45 | 31 | 43.10% | 14 | 27.50% | |
| BMI (kg/m2) | 0.75 | |||||
| <18.5 | 14 | 10 | 13.90% | 4 | 7.80% | |
| 18.5–23.9 | 61 | 35 | 48.60% | 26 | 51.00% | |
| 24–26.9 | 31 | 18 | 25.00% | 13 | 25.50% | |
| ≥27 | 17- | 9 | 12.50% | 8 | 15.70% | |
| Stage | 0.019 | |||||
| I | 27 | 12 | 16.70% | 15 | 29.40% | |
| II | 33 | 17 | 23.60% | 16 | 31.40% | |
| III | 41 | 24 | 33.30% | 17 | 33.30% | |
| IV | 22 | 19 | 26.40% | 3 | 5.90% | |
| Location | 0.871 | |||||
| Colon | 83 | 49 | 68.10% | 34 | 66.70% | |
| Rectum | 40 | 23 | 31.90% | 17 | 33.30% | |
| Differentiation | 0.804 | |||||
| Well | 39 | 22 | 30.60% | 17 | 33.30% | |
| Moderate | 76 | 46 | 63.90% | 30 | 58.80% | |
| Poor | 8 | 4 | 5.60% | 4 | 7.80% | |
| CEA (ng/mL) | 0.001 | |||||
| <5 | 75 | 35 | 48.60% | 40 | 78.40% | |
| ≥5 | 48 | 37 | 51.40% | 11 | 21.60% | |
| Albumin (g/dL) | 0.005 | |||||
| <3.5 | 47 | 35 | 48.60% | 12 | 23.50% | |
| ≥3.5 | 76 | 37 | 51.40% | 39 | 76.50% | |
| CRP (mg/L) | 0.003 | |||||
| <5 | 55 | 24 | 33.30% | 31 | 60.80% | |
| ≥5 | 68 | 48 | 66.70% | 20 | 39.20% | |
| mGPS | 0.004 | |||||
| 0 | 72 | 36 | 50.00% | 36 | 70.60% | |
| 1 | 17 | 8 | 11.10% | 9 | 17.60% | |
| 2 | 34 | 28 | 38.90% | 6 | 11.80% | |
| Variables | Univariate Cox Regression | Multivariate Cox Regression | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age (<65 vs. ≥65 years) | 1.878 | 0.928–3.801 | 0.080 | |||
| Sex (male vs. female) | 0.807 | 0.419–1.557 | 0.523 | |||
| BMI (<18.5 vs. ≥18.5 kg/m2) | 0.368 | 0.161–0.841 | 0.018 | |||
| BMI (<24 vs. ≥24 kg/m2) | 0.754 | 0.384–1.482 | 0.413 | |||
| Stage (I vs. II vs. III vs. IV) | 4.478 | 2.797–7.170 | <0.001 | 3.803 | 2.382–6.073 | <0.001 |
| Location (colon vs. rectum) | 1.681 | 0.871–3.242 | 0.122 | |||
| Differentiation (well vs. intermediate vs. poor) | 1.235 | 0.679–2.246 | 0.489 | |||
| CEA (<5 vs. ≥5 ng/mL) | 6.805 | 3.200–14.469 | <0.001 | |||
| Albumin(<3.5 vs. ≥3.5 g/dL) | 0.323 | 0.167–0.623 | 0.001 | 0.401 | 0.204–0.786 | 0.008 |
| CRP (<5 vs. ≥5 mg/dL) | 6.707 | 2.609–17.239 | <0.001 | |||
| mGPS (0 vs. 1 vs. 2) | 2.083 | 1.459–2.974 | <0.001 | |||
| Glutamine (<52 vs. ≥52 ng/μL) | 0.135 | 0.048–0.382 | <0.001 | 0.270 | 0.093–0.787 | 0.016 |
| Variables | Univariate Cox Regression | Multivariate Cox Regression | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age (<65 vs. ≥65 years) | 1.490 | 0.742–2.995 | 0.263 | |||
| Sex (male vs. female) | 0.799 | 0.406–1.572 | 0.517 | |||
| BMI (<18.5 vs. ≥18.5 kg/m2) | 0.382 | 0.158–0.922 | 0.032 | 0.231 | 0.085-0.631 | 0.004 |
| BMI (<24 vs. ≥24 kg/m2) | 0.976 | 0.496–1.919 | 0.943 | |||
| Stage (I vs. II vs. III vs. IV) | 7.631 | 4.310–13.511 | <0.001 | 7.305 | 3.996-13.355 | <0.001 |
| Location (colon vs. rectum) | 1.867 | 0.954–3.651 | 0.068 | |||
| Differentiation (well vs. intermediate vs. poor) | 1.721 | 0.930–3.187 | 0.084 | |||
| CEA (<5 vs. ≥5 ng/mL) | 4.746 | 2.319–9.716 | <0.001 | |||
| Albumin (<3.5 vs. ≥3.5 g/dL) | 0.454 | 0.234–0.882 | 0.020 | |||
| CRP (<5 vs. ≥5 mg/dL) | 4.213 | 1.837–9.662 | 0.001 | |||
| mGPS (0 vs. 1 vs. 2) | 1.689 | 1.179–2.419 | 0.004 | |||
| Glutamine (<52 vs. ≥52 ng/μL) | 0.234 | 0.097–0.564 | 0.001 | 0.367 | 0.143–0.941 | 0.037 |
| Cytokines (pg/mL) | Low Glutamine (<52 ng/μL, n = 72) | High Glutamine (≥52 ng/μL, n = 51) | p-Value |
|---|---|---|---|
| TNF-α | 92.9 ± 112.3 | 66.7 ± 24.9 | 0.104 |
| IL-1β | 26.2 ± 46.3 | 14.0 ± 5.5 | 0.030 |
| IL-6 | 16.4 ± 35.8 | 7.5 ± 4.3 | 0.041 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ling, H.H.; Pan, Y.-P.; Fan, C.-W.; Tseng, W.-K.; Huang, J.-S.; Wu, T.-H.; Chou, W.-C.; Wang, C.-H.; Yeh, K.-Y.; Chang, P.-H. Clinical Significance of Serum Glutamine Level in Patients with Colorectal Cancer. Nutrients 2019, 11, 898. https://doi.org/10.3390/nu11040898
Ling HH, Pan Y-P, Fan C-W, Tseng W-K, Huang J-S, Wu T-H, Chou W-C, Wang C-H, Yeh K-Y, Chang P-H. Clinical Significance of Serum Glutamine Level in Patients with Colorectal Cancer. Nutrients. 2019; 11(4):898. https://doi.org/10.3390/nu11040898
Chicago/Turabian StyleLing, Hang Huong, Yi-Ping Pan, Chung-Wei Fan, Wen-Ko Tseng, Jen-Seng Huang, Tsung-Han Wu, Wen-Chi Chou, Cheng-Hsu Wang, Kun-Yun Yeh, and Pei-Hung Chang. 2019. "Clinical Significance of Serum Glutamine Level in Patients with Colorectal Cancer" Nutrients 11, no. 4: 898. https://doi.org/10.3390/nu11040898