
High versus Standard Intensity of Thromboprophylaxis in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration and Reporting
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Certainty (Confidence) of the Outcome
2.7. Statistical Analysis
3. Results
3.1. Literature Search and Inclusion of Studies
3.2. Data Synthesis
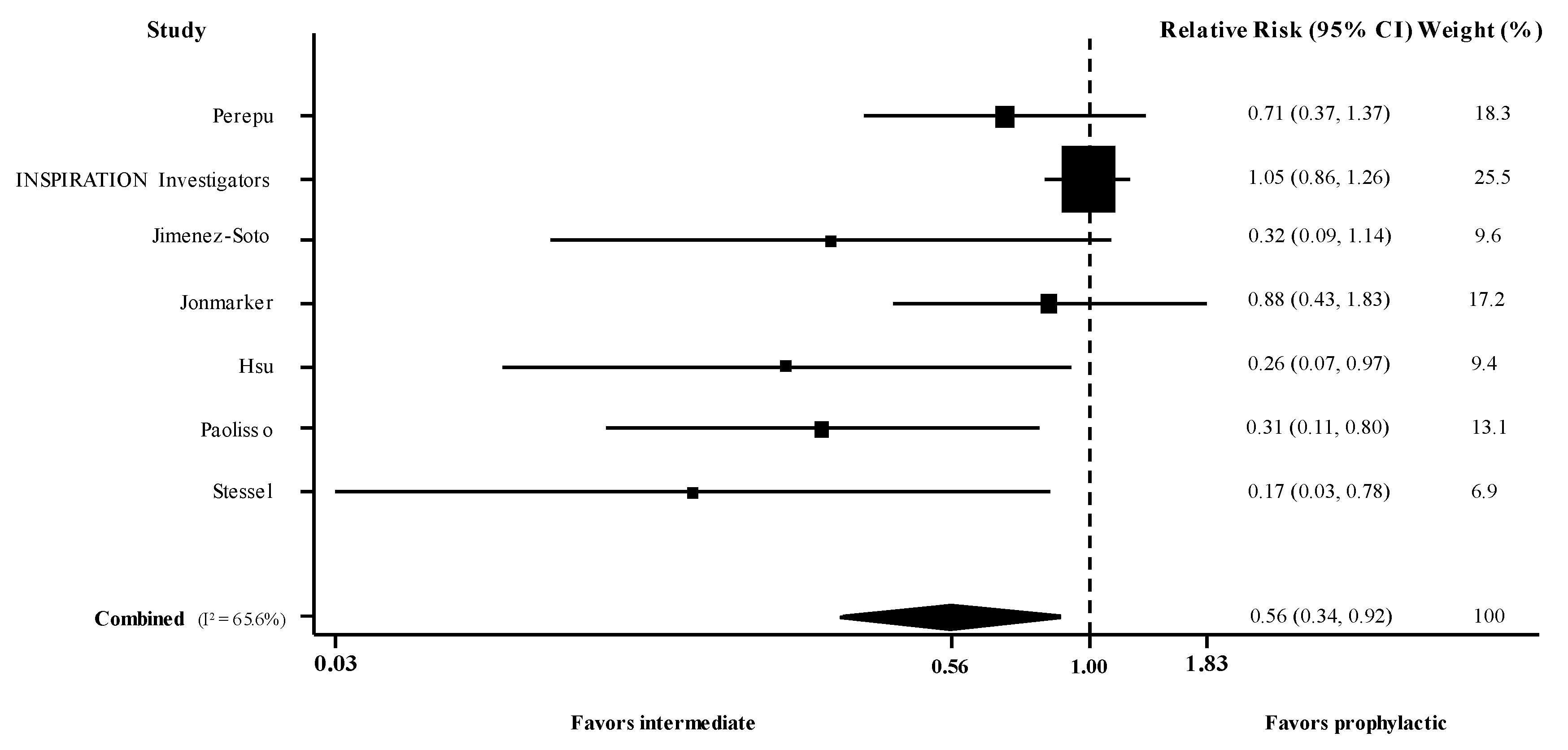
3.2.1. Intermediate versus Prophylactic Dose of Anticoagulation
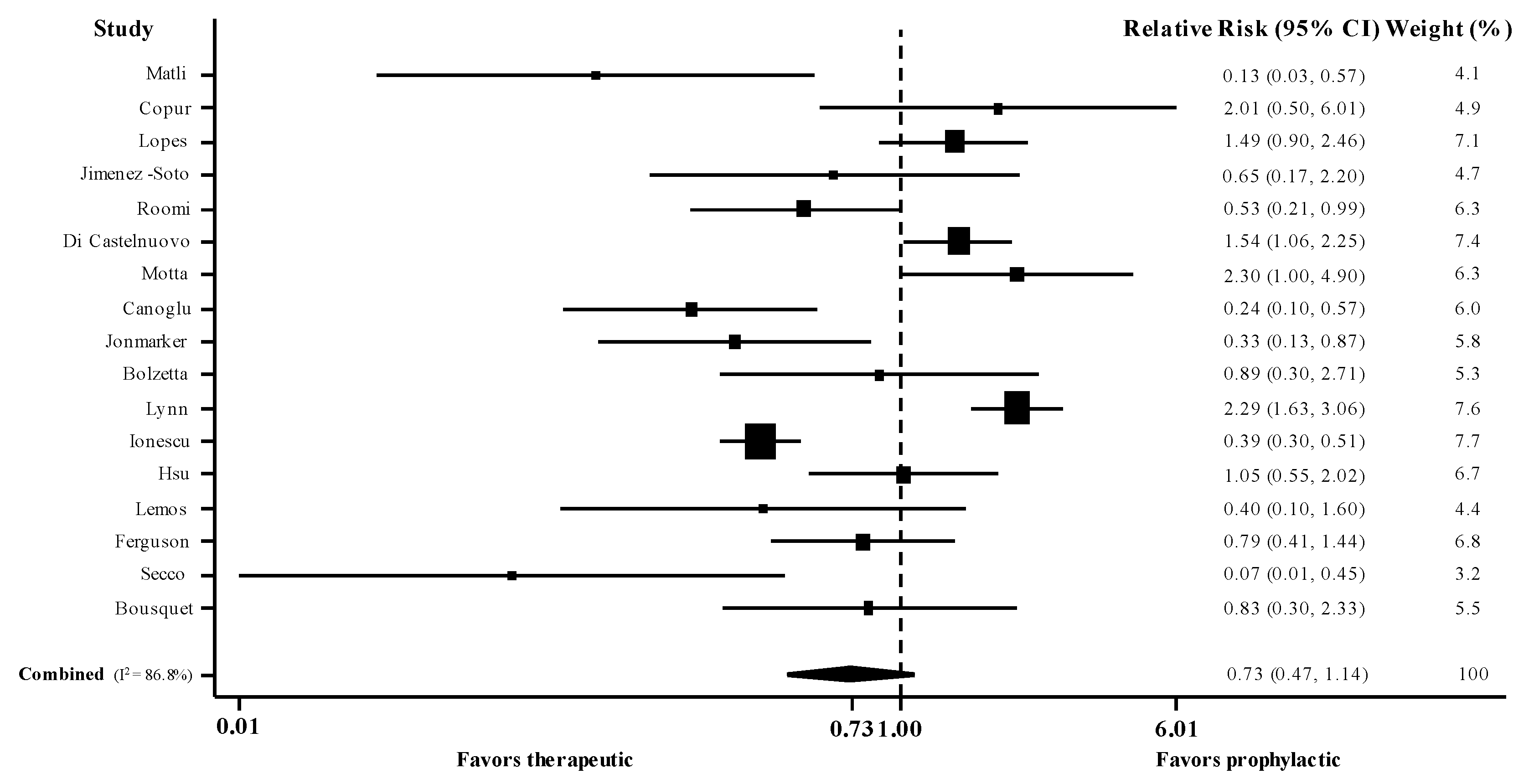
3.2.2. Therapeutic versus Prophylactic Dose of Thromboprophylaxis
3.3. Sensitivity and Meta-Regression Analyses
3.4. Risk of Bias, Publication Bias, and Certainty of the Evidence Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kollias, A.; Kyriakoulis, K.G.; Dimakakos, E.; Poulakou, G.; Stergiou, G.S.; Syrigos, K. Thromboembolic risk and anticoagulant therapy in COVID-19 patients: Emerging evidence and call for action. Br. J. Haematol. 2020, 189, 846–847. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Lagou, S.; Kontopantelis, E.; Stergiou, G.S.; Syrigos, K. Venous thromboembolism in COVID-19: A systematic review and meta-analysis. Vasc. Med. 2021, 26, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, D.; Garcia-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodriguez, C.; Hunt, B.J.; Monreal, M. Incidence of VTE and Bleeding Among Hospitalized Patients With Coronavirus Disease 2019: A Systematic Review and Meta-analysis. Chest 2021, 159, 1182–1196. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Nadkarni, G.N.; Lala, A.; Bagiella, E.; Chang, H.L.; Moreno, P.R.; Pujadas, E.; Arvind, V.; Bose, S.; Charney, A.W.; Chen, M.D.; et al. Anticoagulation, Bleeding, Mortality, and Pathology in Hospitalized Patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1815–1826. [Google Scholar] [CrossRef]
- Rentsch, C.T.; Beckman, J.A.; Tomlinson, L.; Gellad, W.F.; Alcorn, C.; Kidwai-Khan, F.; Skanderson, M.; Brittain, E.; King, J.T., Jr.; Ho, Y.L.; et al. Early initiation of prophylactic anticoagulation for prevention of coronavirus disease 2019 mortality in patients admitted to hospital in the United States: Cohort study. BMJ 2021, 372, n311. [Google Scholar] [CrossRef] [PubMed]
- Kyriakoulis, K.G.; Kollias, A.; Kyriakoulis, I.G.; Kyprianou, I.A.; Papachrysostomou, C.; Makaronis, P.; Kotronias, R.A.; Terentes-Printzios, D.; Toskas, I.; Mikhailidis, D.P. Thromboprophylaxis in Patients with COVID-19: Systematic Review of National and International Clinical Guidance Reports. Curr. Vasc. Pharmacol. 2021. [Google Scholar] [CrossRef]
- Kollias, A.; Poulakou, G.; Dimakakos, E.; Kyriakoulis, K.G.; Syrigos, K. Thromboprophylaxis in COVID-19: Early initiation might be as important as optimal dosing. Thromb. Res. 2021, 204, 134–135. [Google Scholar] [CrossRef]
- REMAP-CAP Investigators; ACTIV-4a Investigators; ATTACC Investigators; Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N.; Carrier, M.; et al. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- ATTACC Investigators; ACTIV-4a Investigators; REMAP-CAP Investigators; Lawler, P.R.; Goligher, E.C.; Berger, J.S.; Neal, M.D.; McVerry, B.J.; Nicolau, J.C.; Gong, M.N.; et al. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef]
- INSPIRATION Investigators; Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; Sezavar, S.H.; Payandemehr, P.; Dabbagh, A.; et al. Effect of Intermediate-Dose vs. Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients with COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar] [CrossRef] [PubMed]
- Lemos, A.C.B.; do Espirito Santo, D.A.; Salvetti, M.C.; Gilio, R.N.; Agra, L.B.; Pazin-Filho, A.; Miranda, C.H. Therapeutic versus prophylactic anticoagulation for severe COVID-19: A randomized phase II clinical trial (HESACOVID). Thromb. Res. 2020, 196, 359–366. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs. Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, e216203. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 August 2021).
- Cochrane Handbook for Systematic Reviews of Interventions. Chapter 14: Completing ‘Summary of findings’ Tables and Grading the Certainty of the Evidence. Available online: https://training.cochrane.org/handbook/current/chapter-14 (accessed on 1 August 2021).
- Kirmayr, M.; Quilodran, C.; Valente, B.; Loezar, C.; Garegnani, L.; Franco, J.V.A. The GRADE approach, Part 1: How to assess the certainty of the evidence. Medwave 2021, 21, e8109. [Google Scholar] [CrossRef]
- Grant, R.L. Converting an odds ratio to a range of plausible relative risks for better communication of research findings. BMJ 2014, 348, f7450. [Google Scholar] [CrossRef] [Green Version]
- StatsToDo: Combine Means and SDs into One Group Program. Available online: https://www.statstodo.com/CombineMeansSDs.php (accessed on 1 August 2021).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Secco, E.; Pasqualetto, M.C.; Bombardini, T.; Picano, E.; Rigo, F. A possible benefit from therapeutic anticoagulation in patients with coronavirus disease 2019: The Dolo hospital experience in Veneto, Italy. Kardiol. Pol. 2020, 78, 919–921. [Google Scholar] [CrossRef]
- Ionescu, F.; Jaiyesimi, I.; Petrescu, I.; Lawler, P.R.; Castillo, E.; Munoz-Maldonado, Y.; Imam, Z.; Narasimhan, M.; Abbas, A.E.; Konde, A.; et al. Association of anticoagulation dose and survival in hospitalized COVID-19 patients: A retrospective propensity score-weighted analysis. Eur. J. Haematol. 2021, 106, 165–174. [Google Scholar] [CrossRef]
- Motta, J.K.; Ogunnaike, R.O.; Shah, R.; Stroever, S.; Cedeno, H.V.; Thapa, S.K.; Chronakos, J.J.; Jimenez, E.J.; Petrini, J.; Hegde, A. Clinical Outcomes with the Use of Prophylactic Versus Therapeutic Anticoagulation in Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0309. [Google Scholar] [CrossRef] [PubMed]
- Roomi, S.S.; Saddique, M.; Ullah, W.; Haq, S.; Ashfaq, A.; Madara, J.; Boigon, M. Anticoagulation in COVID-19: A single-center retrospective study. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 17–22. [Google Scholar] [CrossRef]
- Stessel, B.; Vanvuchelen, C.; Bruckers, L.; Geebelen, L.; Callebaut, I.; Vandenbrande, J.; Pellens, B.; Van Tornout, M.; Ory, J.P.; van Halem, K.; et al. Impact of implementation of an individualised thromboprophylaxis protocol in critically ill ICU patients with COVID-19: A longitudinal controlled before-after study. Thromb. Res. 2020, 194, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Bergamaschi, L.; D’Angelo, E.C.; Donati, F.; Giannella, M.; Tedeschi, S.; Pascale, R.; Bartoletti, M.; Tesini, G.; Biffi, M.; et al. Preliminary Experience With Low Molecular Weight Heparin Strategy in COVID-19 Patients. Front. Pharmacol. 2020, 11, 1124. [Google Scholar] [CrossRef]
- Jimenez-Soto, R.; Aguilar-Soto, M.; Rodriguez-Toledo, C.A.; Camiro-Zuniga, A.; Demichelis, R.; Group, A.S. The impact of different prophylactic anticoagulation doses on the outcomes of patients with COVID-19. Thromb. Res. 2021, 202, 14–16. [Google Scholar] [CrossRef]
- Perepu, U.S.; Chambers, I.; Wahab, A.; Ten Eyck, P.; Wu, C.; Dayal, S.; Sutamtewagul, G.; Bailey, S.R.; Rosenstein, L.J.; Lentz, S.R. Standard prophylactic versus intermediate dose enoxaparin in adults with severe COVID-19: A multi-center, open-label, randomized controlled trial. J. Thromb. Haemost. 2021, 19, 2225–2234. [Google Scholar] [CrossRef]
- Matli, K.; Chamoun, N.; Fares, A.; Zibara, V.; Al-Osta, S.; Nasrallah, R.; Salameh, P.; Mokhbat, J.; Ghanem, G. Combined anticoagulant and antiplatelet therapy is associated with an improved outcome in hospitalised patients with COVID-19: A propensity matched cohort study. Open Heart 2021, 8, e001785. [Google Scholar] [CrossRef]
- Copur, B.; Surme, S.; Sayili, U.; Tuncer, G.; Zerdali, E.; Yazla, M.; Nakir, I.Y.; Buyukyazgan, A.; Kurt-Cinar, A.R.; Balli, H.; et al. Comparison of standard prophylactic and preemptive therapeutic low molecular weight heparin treatments in hospitalized patients with COVID-19. Bratisl. Lek. Listy 2021, 122, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; de Barros, E.S.P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Bronhara, B.; Damiani, L.P.; Barbosa, L.M.; de Aveiro Morata, J.; Ramacciotti, E.; de Aquino Martins, P.; et al. Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef]
- Hsu, A.; Liu, Y.; Zayac, A.S.; Olszewski, A.J.; Reagan, J.L. Intensity of anticoagulation and survival in patients hospitalized with COVID-19 pneumonia. Thromb. Res. 2020, 196, 375–378. [Google Scholar] [CrossRef]
- Jonmarker, S.; Hollenberg, J.; Dahlberg, M.; Stackelberg, O.; Litorell, J.; Everhov, A.H.; Jarnbert-Pettersson, H.; Soderberg, M.; Grip, J.; Schandl, A.; et al. Dosing of thromboprophylaxis and mortality in critically ill COVID-19 patients. Crit. Care 2020, 24, 653. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, G.; Falgarone, G.; Deutsch, D.; Derolez, S.; Lopez-Sublet, M.; Goudot, F.X.; Amari, K.; Uzunhan, Y.; Bouchaud, O.; Pamoukdjian, F. ADL-dependency, D-Dimers, LDH and absence of anticoagulation are independently associated with one-month mortality in older inpatients with COVID-19. Aging 2020, 12, 11306–11313. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.; Volk, S.; Vondracek, T.; Flanigan, J.; Chernaik, A. Empiric Therapeutic Anticoagulation and Mortality in Critically Ill Patients With Respiratory Failure From SARS-CoV-2: A Retrospective Cohort Study. J. Clin. Pharmacol. 2020, 60, 1411–1415. [Google Scholar] [CrossRef]
- Lynn, L.; Reyes, J.A.; Hawkins, K.; Panda, A.; Linville, L.; Aldhahri, W.; Kango, G.; Shah, S.; Ayanian, S.; Teufel, K. The effect of anticoagulation on clinical outcomes in novel Coronavirus (COVID-19) pneumonia in a U.S. cohort. Thromb. Res. 2021, 197, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Bolzetta, F.; Maselli, M.; Formilan, M.; Busonera, F.; Albanese, P.; Chiaromanni, F.; Romano, A.; Veronese, N. Prophylactic or therapeutic doses of heparins for COVID-19 infection? A retrospective study. Aging Clin. Exp. Res. 2021, 33, 213–217. [Google Scholar] [CrossRef]
- Canoglu, K.; Saylan, B. Therapeutic dosing of low-molecular-weight heparin may decrease mortality in patients with severe COVID-19 infection. Ann. Saudi Med. 2020, 40, 462–468. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Cauda, R.; Guaraldi, G.; Menicanti, L.; Mennuni, M.; et al. Heparin in COVID-19 Patients Is Associated with Reduced In-Hospital Mortality: The Multicenter Italian CORIST Study. Thromb. Haemost. 2021, 121, 1054–1065. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Syrigos, N.K.; Stergiou, G.S. Anticoagulation therapy in COVID-19: Is there a dose-dependent benefit? Thromb. Res. 2021, 199, 19–20. [Google Scholar] [CrossRef]
- Ciceri, F.; Beretta, L.; Scandroglio, A.M.; Colombo, S.; Landoni, G.; Ruggeri, A.; Peccatori, J.; D’Angelo, A.; De Cobelli, F.; Rovere-Querini, P.; et al. Microvascular COVID-19 lung vessels obstructive thromboinflammatory syndrome (MicroCLOTS): An atypical acute respiratory distress syndrome working hypothesis. Crit. Care Resusc. 2020, 22, 95–97. [Google Scholar] [CrossRef]
- Poulakou, G.; Dimakakos, E.; Kollias, A.; Kyriakoulis, K.G.; Rapti, V.; Trontzas, I.; Thanos, C.; Abdelrasoul, M.; Vantana, T.; Leontis, K.; et al. Beneficial Effects of Intermediate Dosage of Anticoagulation Treatment on the Prognosis of Hospitalized COVID-19 Patients: The ETHRA Study. In Vivo 2021, 35, 653–661. [Google Scholar] [CrossRef]
- Drago, F.; Gozzo, L.; Li, L.; Stella, A.; Cosmi, B. Use of Enoxaparin to Counteract COVID-19 Infection and Reduce Thromboembolic Venous Complications: A Review of the Current Evidence. Front. Pharmacol. 2020, 11, 579886. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Costanzo, S.; Di Castelnuovo, A.; de Gaetano, G.; Donati, M.B.; Iacoviello, L. Different Anticoagulant Regimens, Mortality, and Bleeding in Hospitalized Patients with COVID-19: A Systematic Review and an Updated Meta-Analysis. Semin. Thromb. Hemost. 2021, 47, 372–391. [Google Scholar] [CrossRef] [PubMed]
- Kamel, A.M.; Sobhy, M.; Magdy, N.; Sabry, N.; Farid, S. Anticoagulation outcomes in hospitalized COVID-19 patients: A systematic review and meta-analysis of case-control and cohort studies. Rev. Med. Virol. 2021, 31, e2180. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Design | N | ICU (%) | Males (%) | I/P or T/P (%) | Type of Anticoagulation |
|---|---|---|---|---|---|---|
| Intermediate versus prophylactic dose | ||||||
| Peperu et al. [30] | R | 173 | 62 | 56 | 50/50 | LMWH |
| Sadeghipour et al. [11] | R | 562 | 100 | 58 | 49/51 | LMWH/UFH |
| Jimenez-Soto et al. [29] | O | 244 | 0 | 66 | 55/45 | LMWH |
| Jonmarker et al. [35] | O | 115 | 100 | 82 | 42/58 | LMWH |
| Hsu et al. [34] | O | 393 | NR | 55 | 4/96 | LMWH/UFH/DOAC/VKA |
| Paolisso et al. [28] | O | 450 | 0 | 63 | 20/80 | LMWH |
| Stessel et al. [27] | O | 72 | 100 | 68 | 36/64 | LMWH |
| Therapeutic versus prophylactic dose | ||||||
| Lopes et al. [33] | R | 615 | 6 | 60 | 51/49 | LMWH/DOAC |
| Lemos et al. [12] | R | 20 | 100 | 80 | 50/50 | LMWH/UFH |
| Matli et al. [31] | O | 82 | 0 | 62 | 38/62 | LMWH/UFH/DOAC/Fondaparinux |
| Copur et al. [32] | O | 115 | 0 | 50 | 40/60 | LMWH |
| Jimenez-Soto et al. [29] | O | 186 | 0 | 67 | 41/59 | LMWH |
| Roomi et al. [26] | O | 176 | NR | NR | 19/81 | NR |
| Di Castelnuovo et al. [41] | O | 1577 | NR | NR | 30/70 | UFH |
| Motta et al. [25] | O | 374 | 17 | 59 | 20/80 | LMWH/UFH |
| Canoglu et al. [40] | O | 154 | NR | 62 | 36/64 | LMWH |
| Jonmarker et al. [35] | O | 104 | 100 | 87 | 36/64 | LMWH |
| Bolzetta et al. [39] | O | 81 | 0 | 60 | 30/70 | LMWH/UFH/Fondaparinux |
| Lynn et al. [38] | O | 402 | 27 | 54 | 38/62 | LMWH/UFH/DOAC |
| Ionescu et al. [24] | O | 3119 | 20 | 49 | 32/68 | LMWH/UFH/DOAC/VKA |
| Hsu et al. [34] | O | 425 | NR | 55 | 11/89 | LMWH/UFH/DOAC/VKA |
| Ferguson et al. [37] | O | 141 | 100 | 55 | 33/67 | LMWH/UFH |
| Secco et al. [23] | O | 112 | NR | 70 | 43/57 | LMWH/DOAC/VKA/Fondaparinux |
| Bousquet et al. [36] | O | 93 | 0 | NR | 34/66 | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kollias, A.; Kyriakoulis, K.G.; Trontzas, I.P.; Rapti, V.; Kyriakoulis, I.G.; Theochari, C.A.; Dimakakos, E.; Poulakou, G.; Syrigos, K. High versus Standard Intensity of Thromboprophylaxis in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5549. https://doi.org/10.3390/jcm10235549
Kollias A, Kyriakoulis KG, Trontzas IP, Rapti V, Kyriakoulis IG, Theochari CA, Dimakakos E, Poulakou G, Syrigos K. High versus Standard Intensity of Thromboprophylaxis in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(23):5549. https://doi.org/10.3390/jcm10235549
Chicago/Turabian StyleKollias, Anastasios, Konstantinos G. Kyriakoulis, Ioannis P. Trontzas, Vassiliki Rapti, Ioannis G. Kyriakoulis, Christina A. Theochari, Evangelos Dimakakos, Garyphallia Poulakou, and Konstantinos Syrigos. 2021. "High versus Standard Intensity of Thromboprophylaxis in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 23: 5549. https://doi.org/10.3390/jcm10235549