
68Ga-DOTATOC PET/CT Follow Up after Single or Hypofractionated Gamma Knife ICON Radiosurgery for Meningioma Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. 68Ga-DOTATOC PET/CT
2.2. Planning and Treatment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Achey, R.L.; Gittleman, H.; Schroer, J.; Khanna, V.; Kruchko, C.; Barnholtz-Sloan, J.S. Nonmalignant and Malignant Meningioma Incidence and Survival in the Elderly, 2005–2015, Using the Central Brain Tumor Registry of the United States. Neuro. Oncol. 2019, 21, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Almefty, R.; Haddad, G.; Al-Mefty, O. Meningiomas. In Youmans and Winn Neurological Surgery, 7th ed.; Winn, H.R., Youmans, J.R., Eds.; Elsevier: Philadelphia, PA, USA, 2016; pp. 1107–1131. [Google Scholar]
- Jordan, J.T.; Plotkin, S.R. Benign Intracranial Tumors. Neurol. Clin. 2018, 36, 501–516. [Google Scholar] [CrossRef]
- Rogers, L.; Barani, I.; Chamberlain, M.; Kaley, T.J.; McDermott, M.; Raizer, J.; Schiff, D.; Weber, D.C.; Wen, P.Y.; Vogelbaum, M.A. Meningiomas: Knowledge Base, Treatment Outcomes, and Uncertainties. A RANO Review. J. Neurosurg. 2015, 122, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Barone, F.; Alberio, N.; Iacopino, D.G.; Giammalva, G.R.; D’Arrigo, C.; Tagnese, W.; Graziano, F.; Cicero, S.; Maugeri, R. Brain Mapping as Helpful Tool in Brain Glioma Surgical Treatment-Toward the “Perfect Surgery”? Brain Sci. 2018, 8, 192. [Google Scholar] [CrossRef] [Green Version]
- International Commission of Radiation Units and Measurements. Prescribing, Recording, and Reporting Photon BeamTherapy; Report no. 50; ICRU: Bethesda, MD, USA, 1993. [Google Scholar]
- Moghaddasi, L.; Bezak, E.; Marcu, L.G. Current challenges in clinical target volume definition: Tumour margins and microscopic extensions. Acta Oncol. 2012, 51, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.S.; Tome, W.A.; Harari, P.M. Heterogeneity in head and neck IMRT target design and clinical practice. Radiother. Oncol. 2012, 103, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Raffa, G.; Picht, T.; Scibilia, A.; Rösler, J.; Rein, J.; Conti, A.; Ricciardo, G.; Cardali, S.M.; Vajkoczy, P.; Germanò, A. Surgical Treatment of Meningiomas Located in the Rolandic Area: The Role of Navigated Transcranial Magnetic Stimulation for Preoperative Planning, Surgical Strategy, and Prediction of Arachnoidal Cleavage and Motor Outcome. J. Neurosurg. 2019, 133, 107–118. [Google Scholar] [CrossRef]
- Unterrainer, M.; Ruf, V.; Ilhan, H.; Vettermann, F.J.; Cyran, C.C.; Niyazi, M.; Bartenstein, P.; Tonn, J.C.; Albert, N.L. 68Ga-DOTATOC PET/CT Differentiates Meningioma From Dural Metastases. Clin. Nucl. Med. 2019, 44, 412–413. [Google Scholar] [CrossRef] [PubMed]
- Galldiks, N.; Albert, N.L.; Sommerauer, M.; Grosu, A.L.; Ganswindt, U.; Law, I.; Preusser, M.; Le Rhun, E.; Vogelbaum, M.A.; Zadeh, G.; et al. PET imaging in patients with meningioma-report of the RANO/PET Group. Neuro. Oncol. 2017, 19, 1576–1587. [Google Scholar] [CrossRef]
- Rahman, A.; Ahmed, N.; Baniya, P.; Scalia, G.; Umana, G.E.; Chaurasia, B. Primary Sellar Neuroblastoma Mimicking Invasive Pituitary Adenoma: A Systematic Review. J. Neurosurg. Sci. 2020, 64, 377–382. [Google Scholar] [CrossRef]
- Purandare, N.C.; Puranik, A.; Shah, S.; Agrawal, A.; Gupta, T.; Moiyadi, A.; Shetty, P.; Shridhar, E.; Patil, V.; Rangarajan, V. Differentiating dural metastases from meningioma: Role of 68Ga DOTA-NOC PET/CT. Nucl. Med. Commun. 2020, 41, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Savage, N.M.; Alleyne, C.H.; Vender, J.R.; Figueroa, R.; Zhang, H.; Samuel, T.A.; Sharma, S. Dural-based metastatic carcinomas mimicking primary CNS neoplasia: Report of 7 cases emphasizing the role of timely surgery and accurate pathologic evaluation. Int. J. Clin. Exp. Pathol. 2011, 4, 530–540. [Google Scholar]
- Reubi, J.C.; Schaer, J.C.; Waser, B.; Mengod, G. Expression and localization of somatostatin receptor SSTR1, SSTR2, and SSTR3 messenger RNAs in primary human tumors using in situ hybridization. Cancer Res. 1994, 54, 3455–3459. [Google Scholar]
- Ge, Y.; Liu, D.; Zhang, Z.; Li, Y.; Lin, Y.; Wang, G.; Zong, Y.; Liu, E. Gamma Knife Radiosurgery for Intracranial Benign Meningiomas: Follow-up Outcome in 130 Patients. Neurosurg. Focus 2019, 46, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehler, B.; Paulsen, F.; Oksüz, M.O.; Hauser, T.-K.; Eschmann, S.M.; Bares, R.; Pfannenberg, C.; Bamberg, M.; Bartenstein, P.; Belka, C.; et al. [68Ga]-DOTATOC-PET/CT for Meningioma IMRT Treatment Planning. Radiat. Oncol. 2009, 4, 56. [Google Scholar] [CrossRef] [Green Version]
- Graf, R.; Nyuyki, F.; Steffen, I.G.; Michel, R.; Fahdt, D.; Wust, P.; Brenner, W.; Budach, V.; Wurm, R.; Plotkin, M. Contribution of 68Ga-DOTATOC PET/CT to Target Volume Delineation of Skull Base Meningiomas Treated with Stereotactic Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Milker-Zabel, S.; Zabel-du Bois, A.; Henze, M.; Huber, P.; Schulz-Ertner, D.; Hoess, A.; Haberkorn, U.; Debus, J. Improved Target Volume Definition for Fractionated Stereotactic Radiotherapy in Patients with Intracranial Meningiomas by Correlation of CT, MRI, and [68Ga]-DOTATOC-PET. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 222–227. [Google Scholar] [CrossRef]
- Stade, F.; Dittmar, J.-O.; Jäkel, O.; Kratochwil, C.; Haberkorn, U.; Debus, J.; Combs, S.E. Influence of 68Ga-DOTATOC on Sparing of Normal Tissue for Radiation Therapy of Skull Base Meningioma: Differential Impact of Photon and Proton Radiotherapy. Radiat. Oncol. 2018, 13, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acker, G.; Kluge, A.; Lukas, M.; Conti, A.; Pasemann, D.; Meinert, F.; Anh Nguyen, P.T.; Jelgersma, C.; Loebel, F.; Budach, V.; et al. Impact of 68Ga-DOTATOC PET/MRI on Robotic Radiosurgery Treatment Planning in Meningioma Patients: First Experiences in a Single Institution. Neurosurg. Focus 2019, 46, E9. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Wang, X.; Liu, F.; Chen, J. Gamma Knife Radiosurgery for Patients with Multiple Intracranial Meningiomas. World Neurosurg. 2019, 128, e495–e500. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Patel, A.D.; Kano, H.; Flickinger, J.C.; Lunsford, L.D. Long-Term Outcomes After Gamma Knife Radiosurgery for Meningiomas. Am. J. Clin. Oncol. 2016, 39, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.K.; Jung, H.H.; Chang, J.H.; Chang, J.W.; Park, Y.G.; Chang, W.S. Long-Term Results of Gamma Knife Radiosurgery for Intracranial Meningioma. Brain Tumor Res. Treat. 2015, 3, 103–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santacroce, A.; Walier, M.; Régis, J.; Liščák, R.; Motti, E.; Lindquist, C.; Kemeny, A.; Kitz, K.; Lippitz, B.; Martínez Álvarez, R.; et al. Long-Term Tumor Control of Benign Intracranial Meningiomas after Radiosurgery in a Series of 4565 Patients. Neurosurgery 2012, 70, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patient | Years | Sex | Location | Tumor Diameter (cm) | Tumor Volume (cm3) | Gy Gamma Knife | SUV Pre-Gamma Knife | PET Time from Gamma Knife (Months) | SUV Post-Gamma Knife | DeltaSUV | D_Marg |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 36 | male | right fronto-orbital | 3.679 | 208.476808 | 13 | 10.2 | 19 | 13.1 | 28% | 13.0 |
| 2 | 56 | female | left cerebellar | 1.310 | 9.41200765 | 14 | 3.5 | 18 | 2.6 | −26% | 14.0 |
| 3 | 63 | male | left petroclival | 4.593 | 405.655829 | 13 | 2.3 | 14 | 2.3 | 0% | 13.0 |
| 4 | 36 | female | right tentorial | 5.4 | 659.24928 | 12.5 | 53 | 11 | 35.7 | −33% | 12.5 |
| 5 | 33 | male | right parasagittal | 22.265 | 46210.0548 | 5 | 13 | 8 | 12.5 | −4% | |
| 6 | 47 | male | left parasagittal | 1.494 | 13.9611173 | 13.5 | 31.6 | 9 | 44.6 | 41% | 13.5 |
| 7 | 72 | female | left cerebellopontine angle | 5.514 | 701.889378 | 13 | 7.2 | 6 | 4.3 | −40% | 13.0 |
| 8 | 58 | female | olfactory groove | 6.046 | 925.279229 | 13 | 25.8 | 5 | 15.1 | −41% | 12.8 |
| 9 | 58 | female | left cavernous sinus | 0.931 | 3.37844947 | 12.5 | 11.5 | 1 | 10.6 | −8% | 12.8 |
| 10 | 70 | male | right clinoidal | 3.517 | 182.131678 | 13.5 | 24 | 3 | 24 | 0% | 13.5 |
| 11 | 50 | female | left sphenopetrocavernous | 19.8 | 32498.5478 | 4 | 20.8 | 15 | 18.4 | −12% | |
| 12 | 52 | male | right posterior petrous bone | 2 | 33.4933333 | 14 | 68.6 | 14.0 | |||
| 13 | 55 | male | right parasagittal | 10.078 | 4285.4008 | 15 | 7.1 | 15.0 | |||
| 14 | 80 | male | left parietal | 3.608 | 196.638237 | 16 | 9.8 | 16.0 | |||
| 15 | 80 | male | right tentorial | 3.712 | 214.137283 | 13.5 | 7.5 | 16.0 | |||
| 16 | 65 | female | left parieto-occipital | 14.1 | 11736.1519 | 13 | 9 | 13.0 | |||
| 16 | 52 | female | left cerebellar | 2.35 | 54.3340367 | 13 | 2.9 | 13.0 | |||
| 18 | 52 | female | right posterior petrous bone | 1.284 | 8.86264709 | 13 | 92 | 13.0 | |||
| 19 | 51 | female | right tentorial | 0.118 | 0.00687883 | 13 | 16.3 | 13.0 | |||
| 20 | 47 | male | left frontal | 3.684 | 209.327964 | 13 | 10.4 | 16.2 | 56% | 13.0 |
| Average Age | Minimum | Maximum | ||
|---|---|---|---|---|
| Female | 10 | 54.29 | 33 | 80 |
| Male | 10 | |||
| Total | 20 | |||
| Average SUV_pre | Minimum SUV_pre | Maxium SUV_pre | ||
| 21.325 | 2.3 | 92 | ||
| Average D_marg | Minimum D_marg | Maxium D_marg | ||
| 14.45 Gy | 12.5 Gy | 25 Gy | ||
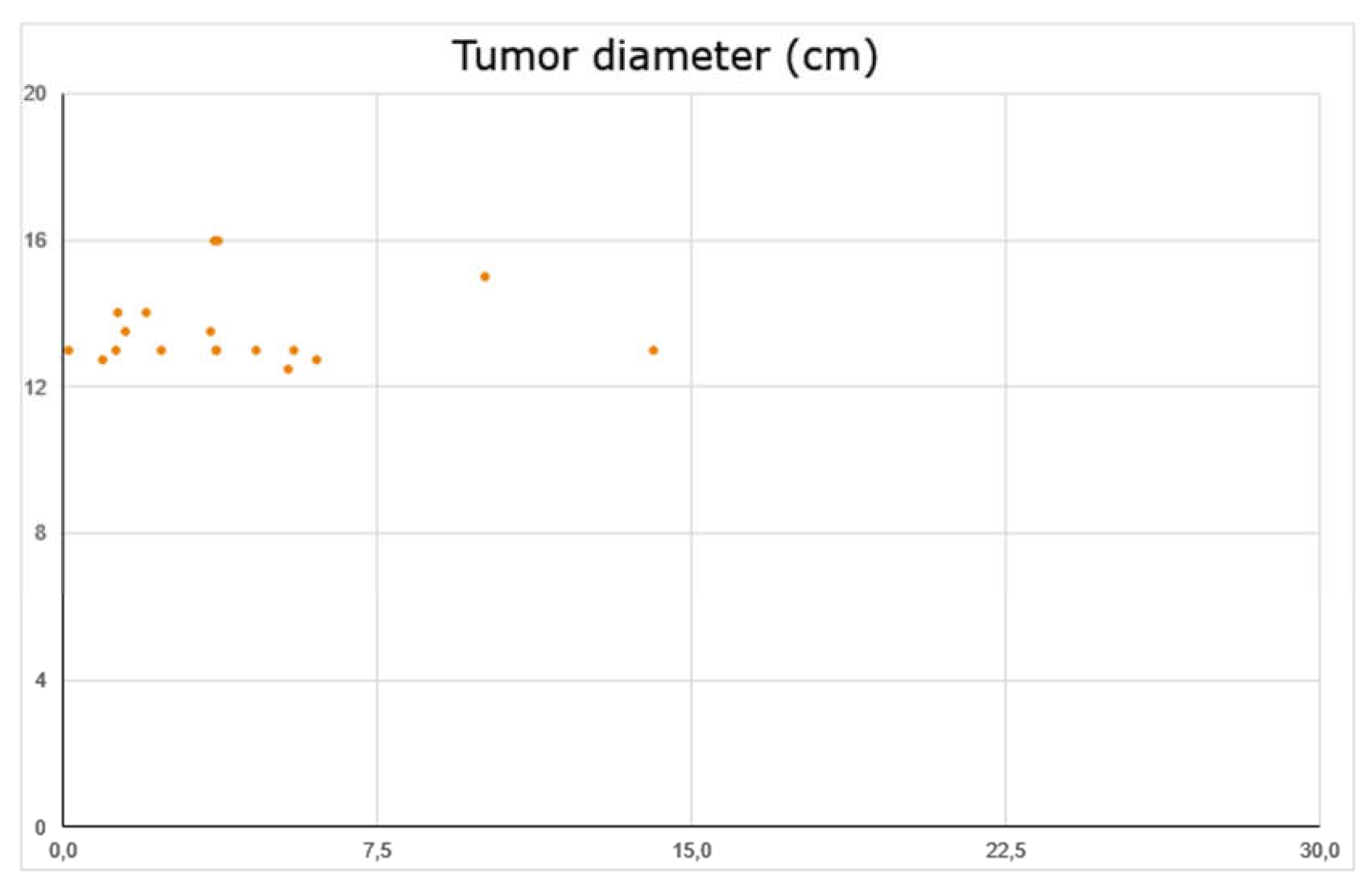
| Average Tumor diameter (cm3) | Minimum Tumor diameter (cm3) | Maxium Tumor diameter (cm3) | ||
| 5.78 | 0.118 | 22.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, F.; Inserra, F.; Scalia, G.; Ippolito, M.; Cosentino, S.; Crea, A.; Sabini, M.G.; Valastro, L.; Patti, I.V.; Mele, S.; et al. 68Ga-DOTATOC PET/CT Follow Up after Single or Hypofractionated Gamma Knife ICON Radiosurgery for Meningioma Patients. Brain Sci. 2021, 11, 375. https://doi.org/10.3390/brainsci11030375
Barone F, Inserra F, Scalia G, Ippolito M, Cosentino S, Crea A, Sabini MG, Valastro L, Patti IV, Mele S, et al. 68Ga-DOTATOC PET/CT Follow Up after Single or Hypofractionated Gamma Knife ICON Radiosurgery for Meningioma Patients. Brain Sciences. 2021; 11(3):375. https://doi.org/10.3390/brainsci11030375
Chicago/Turabian StyleBarone, Fabio, Francesco Inserra, Gianluca Scalia, Massimo Ippolito, Sebastiano Cosentino, Antonio Crea, Maria Gabriella Sabini, Lucia Valastro, Iolanda Valeria Patti, Stefania Mele, and et al. 2021. "68Ga-DOTATOC PET/CT Follow Up after Single or Hypofractionated Gamma Knife ICON Radiosurgery for Meningioma Patients" Brain Sciences 11, no. 3: 375. https://doi.org/10.3390/brainsci11030375