
Non-Invasive Physical Plasma Generated by a Medical Argon Plasma Device Induces the Expression of Regenerative Factors in Human Gingival Keratinocytes, Fibroblasts, and Tissue Biopsies

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. NIPP Application
2.3. Analysis of mRNA Expression
2.4. Analysis of Ki67 and MMP1 Protein Levels
2.5. Caspase-3/7 Assay
2.6. Staining of Tissue Biopsies
2.7. Statistical Analysis
3. Results
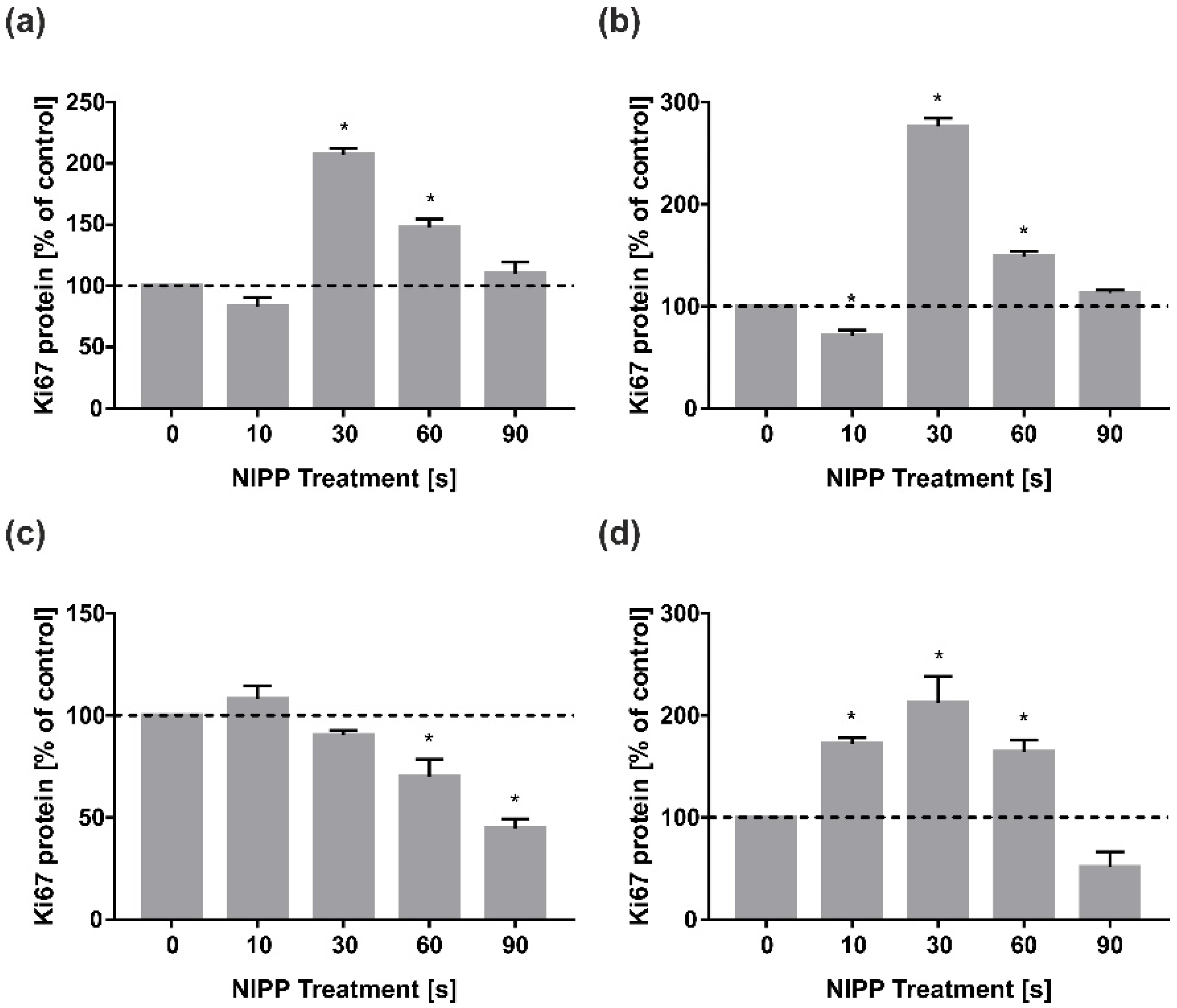
3.1. Analysis of Ki67 and PCNA
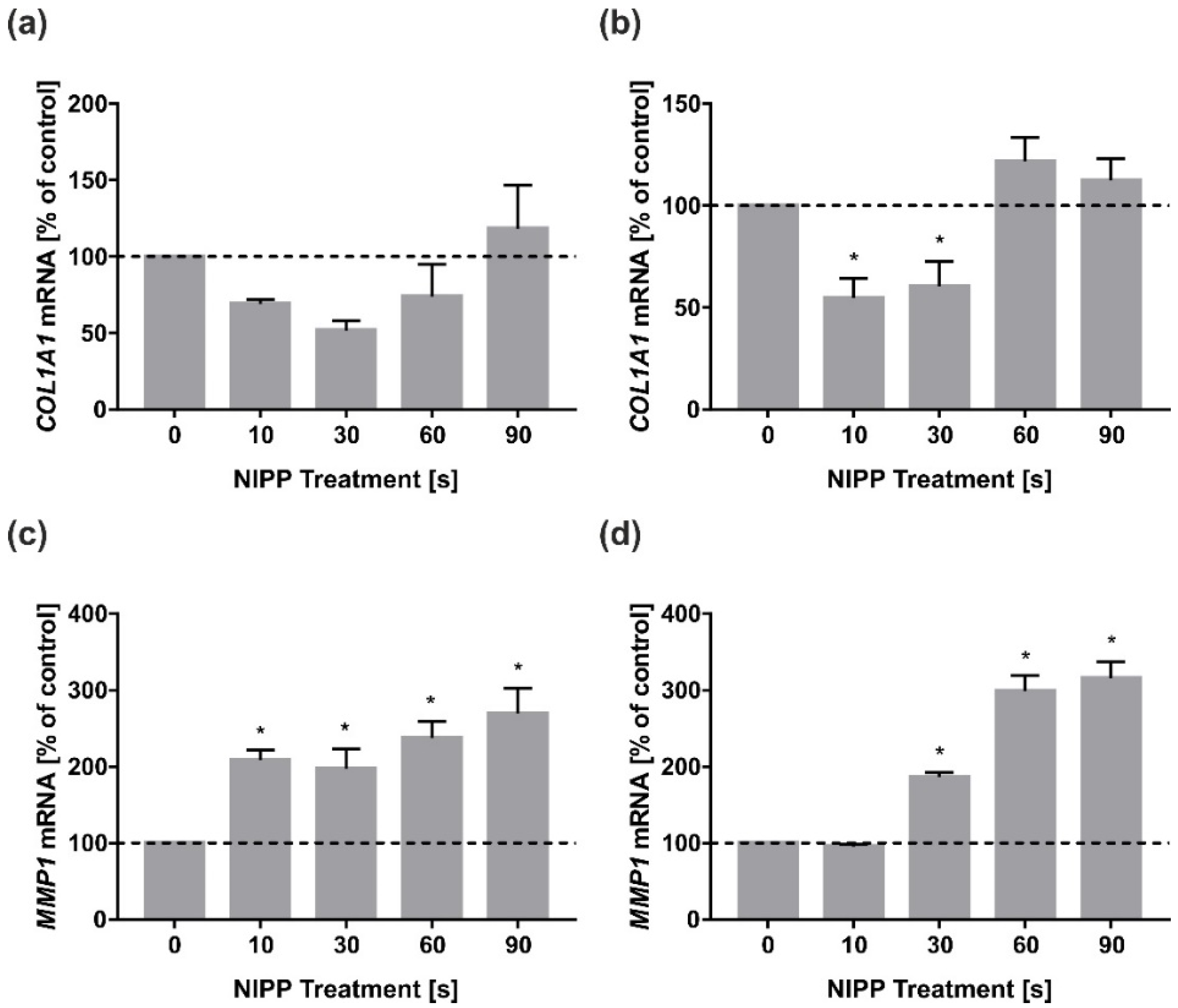
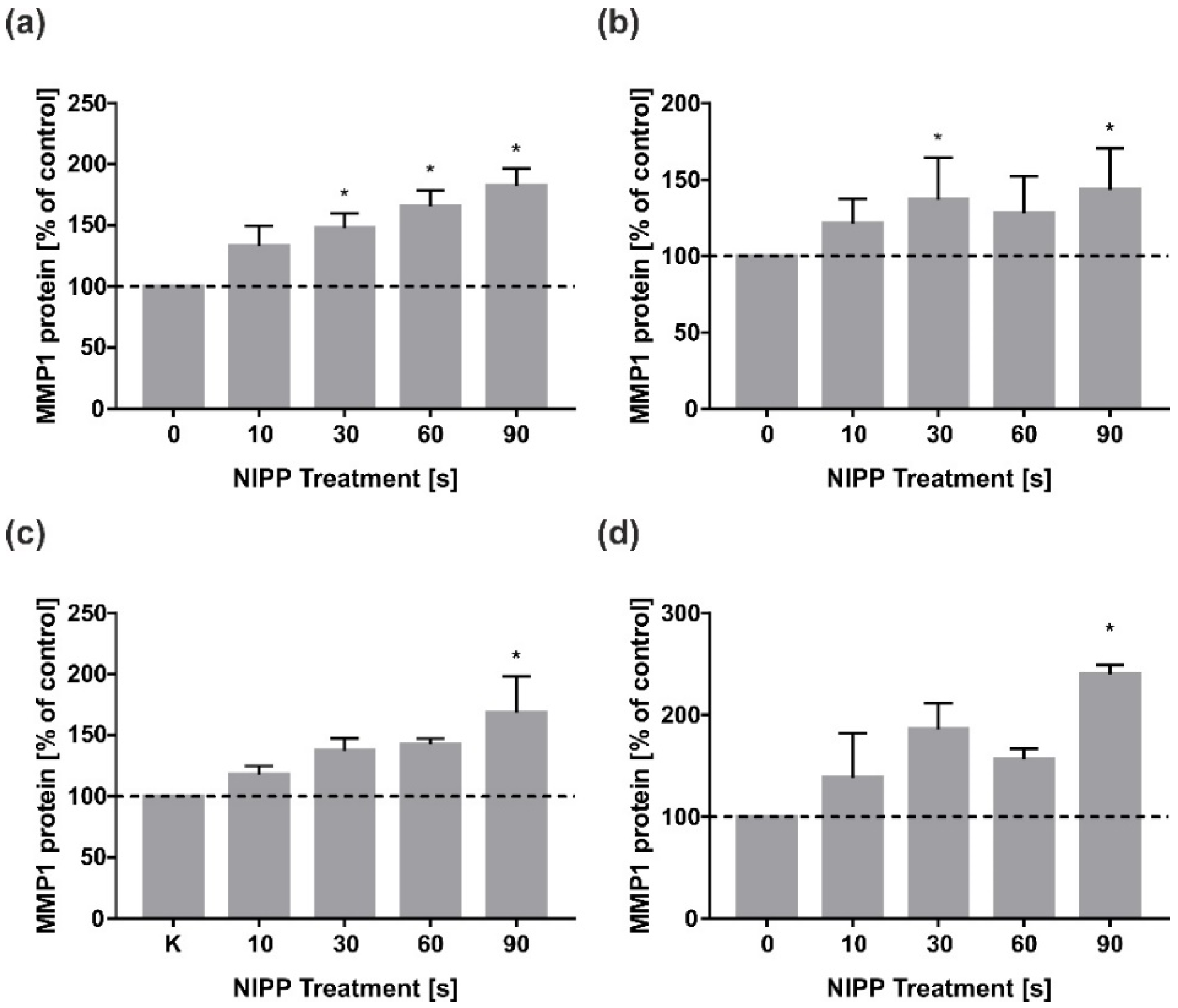
3.2. Analysis of COL1A1 and MMP1
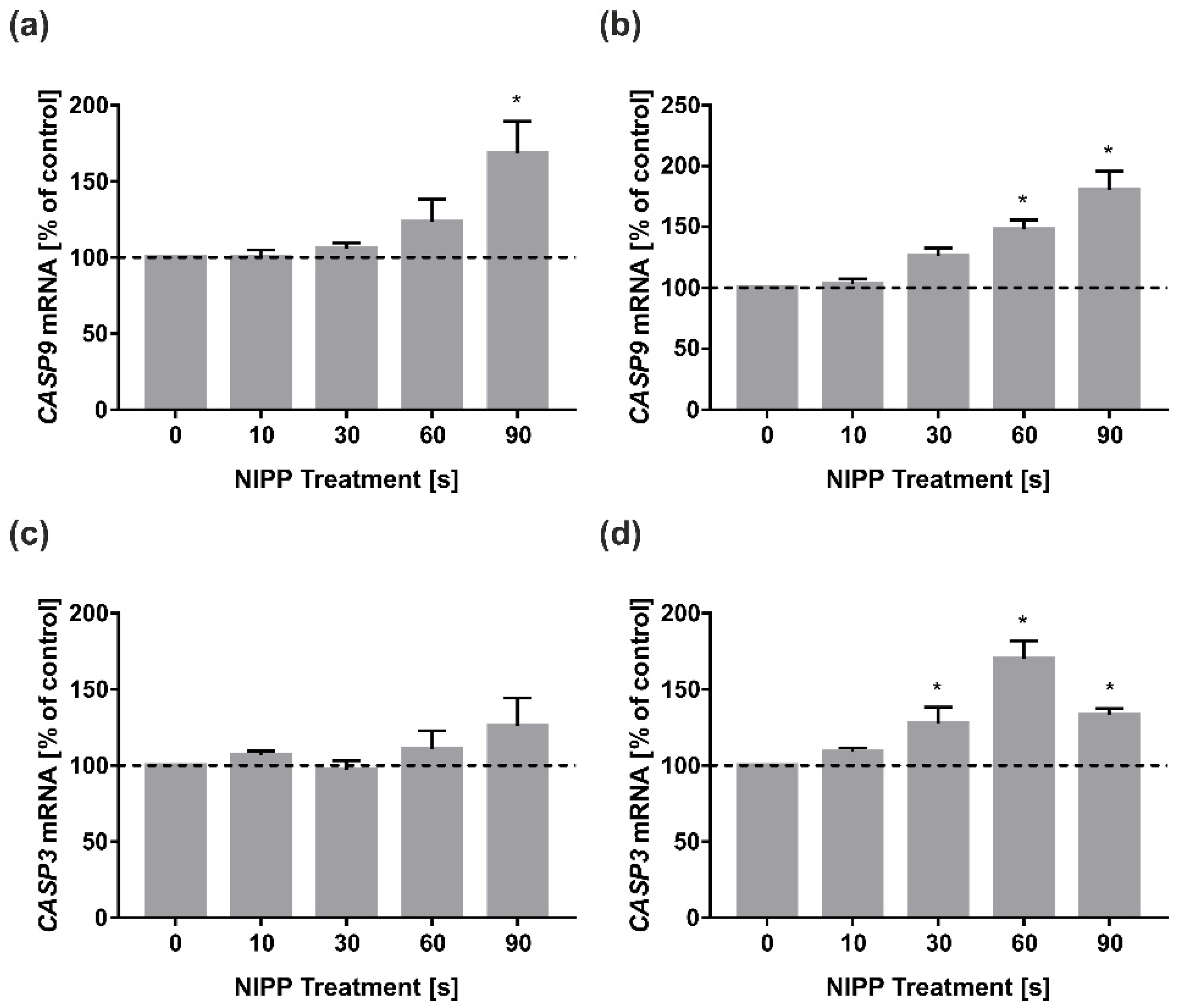
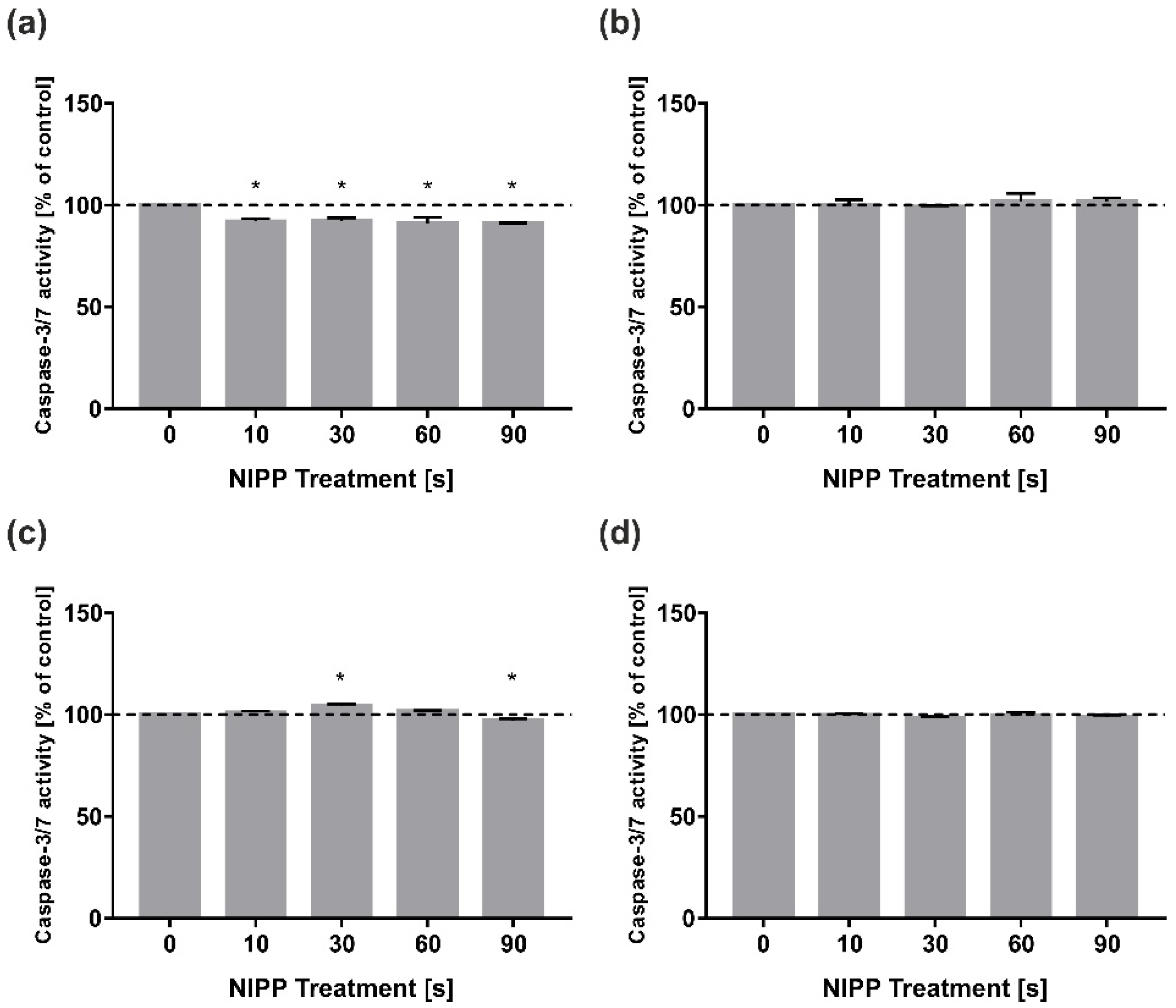
3.3. Examination of CASP9 and CASP3
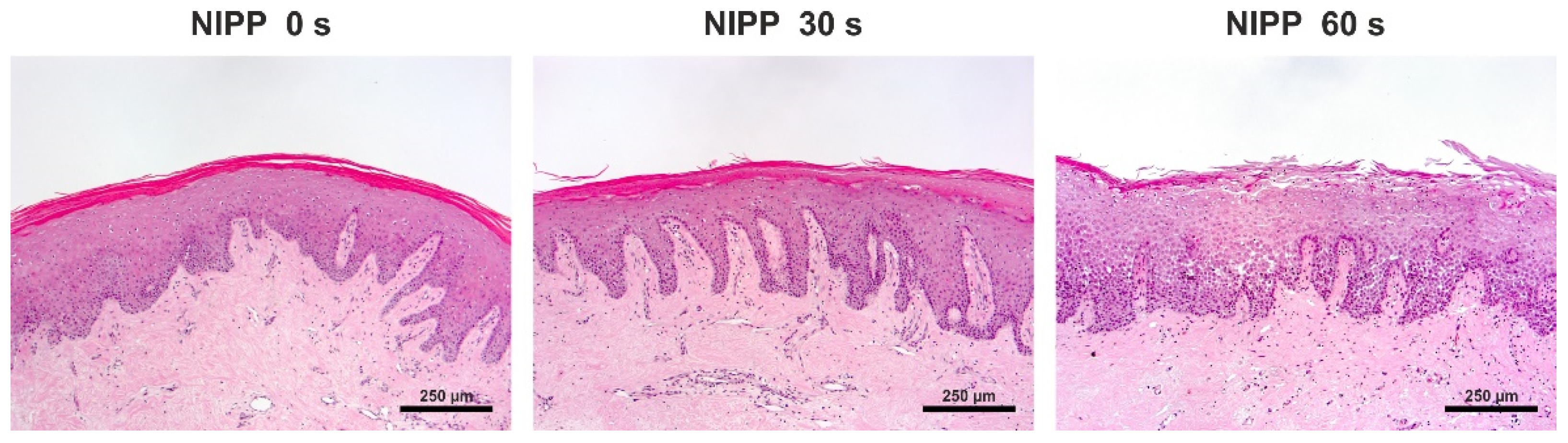
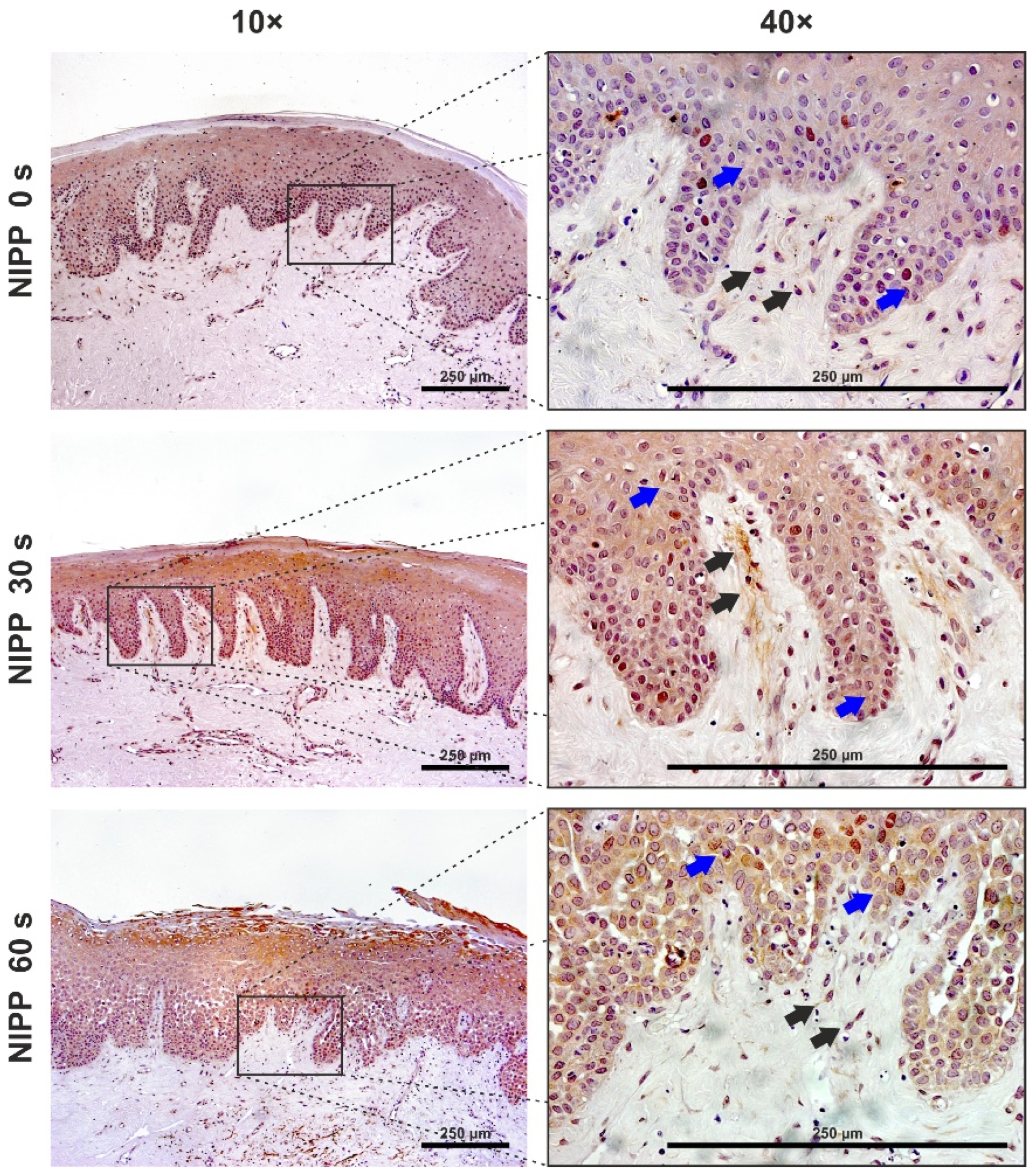
3.4. Examination of Tissue Biopsies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Methé, B.A.; Nelson, K.E.; Pop, M.; Creasy, H.H.; Giglio, M.G.; Huttenhower, C.; Gevers, D.; Petrosino, J.F.; Abubucker, S.; Badger, J.H.; et al. A Framework for Human Microbiome Research. Nature 2012, 486, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Dutzan, N.; Konkel, J.E.; Greenwell-Wild, T.; Moutsopoulos, N.M. Characterization of the Human Immune Cell Network at the Gingival Barrier. Mucosal Immunol. 2016, 9, 1163–1172. [Google Scholar] [CrossRef]
- Winning, T.A.; Townsend, G.C. Oral Mucosal Embryology and Histology. Clin. Dermatol. 2000, 18, 499–511. [Google Scholar] [CrossRef]
- Russo, B.; Brembilla, N.C.; Chizzolini, C. Interplay Between Keratinocytes and Fibroblasts: A Systematic Review Providing a New Angle for Understanding Skin Fibrotic Disorders. Front. Immunol. 2020, 11, 648. [Google Scholar] [CrossRef]
- Diegelmann, R.F.; Cohen, I.K.; McCoy, B.J. Growth Kinetics and Collagen Synthesis of Normal Skin, Normal Scar and Keloid Fibroblasts in Vitro. J. Cell. Physiol. 1979, 98, 341–346. [Google Scholar] [CrossRef]
- Hübner, G.; Brauchle, M.; Smola, H.; Madlener, M.; Fässler, R.; Werner, S. Differential Regulation of Pro-Inflammatory Cytokines during Wound Healing in Normal and Glucocorticoid-Treated Mice. Cytokine 1996, 8, 548–556. [Google Scholar] [CrossRef]
- McFarland-Mancini, M.M.; Funk, H.M.; Paluch, A.M.; Zhou, M.; Giridhar, P.V.; Mercer, C.A.; Kozma, S.C.; Drew, A.F. Differences in Wound Healing in Mice with Deficiency of IL-6 versus IL-6 Receptor. J. Immunol. 2010, 184, 7219–7228. [Google Scholar] [CrossRef] [Green Version]
- Takamiya, M.; Fujita, S.; Saigusa, K.; Aoki, Y. Simultaneous Detection of Eight Cytokines in Human Dermal Wounds with a Multiplex Bead-Based Immunoassay for Wound Age Estimation. Int. J. Legal Med. 2008, 122, 143–148. [Google Scholar] [CrossRef]
- Low, Q.E.H.; Drugea, I.A.; Duffner, L.A.; Quinn, D.G.; Cook, D.N.; Rollins, B.J.; Kovacs, E.J.; DiPietro, L.A. Wound Healing in MIP-1α−/− and MCP-1−/− Mice. Am. J. Pathol. 2001, 159, 457–463. [Google Scholar] [CrossRef]
- Futagami, A.; Ishizaki, M.; Fukuda, Y.; Kawana, S.; Yamanaka, N. Wound Healing Involves Induction of Cyclooxygenase-2 Expression in Rat Skin. Lab. Investig. 2002, 82, 1503–1513. [Google Scholar] [CrossRef] [Green Version]
- Beare, A.H.M.; O’Kane, S.; Krane, S.M.; Ferguson, M.W.J. Severely Impaired Wound Healing in the Collagenase-Resistant Mouse. J. Investig. Dermatol. 2003, 120, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Saffarian, S.; Collier, I.E.; Marmer, B.L.; Elson, E.L.; Goldberg, G. Interstitial Collagenase Is a Brownian Ratchet Driven by Proteolysis of Collagen. Science 2004, 306, 108–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlüter, C.; Duchrow, M.; Wohlenberg, C.; Becker, M.H.; Key, G.; Flad, H.D.; Gerdes, J. The Cell Proliferation-Associated Antigen of Antibody Ki-67: A Very Large, Ubiquitous Nuclear Protein with Numerous Repeated Elements, Representing a New Kind of Cell Cycle-Maintaining Proteins. J. Cell Biol. 1993, 123, 513–522. [Google Scholar] [CrossRef]
- Hergott, G.J.; Kalnins, V.I. Expression of Proliferating Cell Nuclear Antigen in Migrating Retinal Pigment Epithelial Cells during Wound Healing in Organ Culture. Exp. Cell Res. 1991, 195, 307–314. [Google Scholar] [CrossRef]
- Scholzen, T.; Gerdes, J. The Ki-67 Protein: From the Known and the Unknown. J. Cell. Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Bologna-Molina, R.; Mosqueda-Taylor, A.; Molina-Frechero, N.; Mori-Estevez, A.D.; Sánchez-Acuña, G. Comparison of the Value of PCNA and Ki-67 as Markers of Cell Proliferation in Ameloblastic Tumor. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e174–e179. [Google Scholar] [CrossRef] [PubMed]
- Braný, D.; Dvorská, D.; Halašová, E.; Škovierová, H. Cold Atmospheric Plasma: A Powerful Tool for Modern Medicine. Int. J. Mol. Sci. 2020, 21, 2932. [Google Scholar] [CrossRef] [Green Version]
- Kniha, K.; Möhlhenrich, S.C.; Bock, A.; Ayoub, N.; Modabber, A.; Hölzle, F.; Conrads, G.; Goloborodko, E. Evaluation of the Bactericidal Effect of Cold Atmospheric Pressure Plasma on Contaminated Human Bone: An in Vitro Study. Br. J. Oral Maxillofac. Surg. 2020, 58, 329–333. [Google Scholar] [CrossRef]
- Ma, Y.; Ha, C.S.; Hwang, S.W.; Lee, H.J.; Kim, G.C.; Lee, K.-W.; Song, K. Non-Thermal Atmospheric Pressure Plasma Preferentially Induces Apoptosis in P53-Mutated Cancer Cells by Activating ROS Stress-Response Pathways. PLoS ONE 2014, 9, e91947. [Google Scholar] [CrossRef]
- Stratmann, B.; Costea, T.-C.; Nolte, C.; Hiller, J.; Schmidt, J.; Reindel, J.; Masur, K.; Motz, W.; Timm, J.; Kerner, W.; et al. Effect of Cold Atmospheric Plasma Therapy vs. Standard Therapy Placebo on Wound Healing in Patients with Diabetic Foot Ulcers: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2010411. [Google Scholar] [CrossRef]
- Weiss, M.; Daeschlein, G.; Kramer, A.; Burchardt, M.; Brucker, S.; Wallwiener, D.; Stope, M.B. Virucide Properties of Cold Atmospheric Plasma for Future Clinical Applications. J. Med. Virol. 2017, 89, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Haralambiev, L.; Neuffer, O.; Nitsch, A.; Kross, N.C.; Bekeschus, S.; Hinz, P.; Mustea, A.; Ekkernkamp, A.; Gümbel, D.; Stope, M.B. Inhibition of Angiogenesis by Treatment with Cold Atmospheric Plasma as a Promising Therapeutic Approach in Oncology. Int. J. Mol. Sci. 2020, 21, 7098. [Google Scholar] [CrossRef] [PubMed]
- Haralambiev, L.; Wien, L.; Gelbrich, N.; Kramer, A.; Mustea, A.; Burchardt, M.; Ekkernkamp, A.; Stope, M.B.; Gümbel, D. Effects of Cold Atmospheric Plasma on the Expression of Chemokines, Growth Factors, TNF Superfamily Members, Interleukins, and Cytokines in Human Osteosarcoma Cells. Anticancer Res. 2019, 39, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Gan, L.; Zhang, S.; Poorun, D.; Liu, D.; Lu, X.; He, M.; Duan, X.; Chen, H. Medical Applications of Nonthermal Atmospheric Pressure Plasma in Dermatology. JDDG J. Dtsch. Dermatol. Ges. 2018, 16, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Heinlin, J.; Isbary, G.; Stolz, W.; Morfill, G.; Landthaler, M.; Shimizu, T.; Steffes, B.; Nosenko, T.; Zimmermann, J.; Karrer, S. Plasma Applications in Medicine with a Special Focus on Dermatology. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1–11. [Google Scholar] [CrossRef]
- Pekbağrıyanık, T.; Dadas, F.K.; Enhoş, Ş. Effects of Non-Thermal Atmospheric Pressure Plasma on Palatal Wound Healing of Free Gingival Grafts: A Randomized Controlled Clinical Trial. Clin. Oral Investig. 2021, 25, 6269–6278. [Google Scholar] [CrossRef]
- Kusakci-Seker, B.; Demirayak-Akdemir, M. The Effect of Non-Thermal Atmospheric Pressure Plasma Application on Wound Healing after Gingivectomy. Int. Wound J. 2020, 17, 1376–1383. [Google Scholar] [CrossRef]
- Eggers, B.; Wagenheim, A.-M.; Jung, S.; Kleinheinz, J.; Nokhbehsaim, M.; Kramer, F.-J.; Sielker, S. Effect of Cold Atmospheric Plasma (CAP) on Osteogenic Differentiation Potential of Human Osteoblasts. Int. J. Mol. Sci. 2022, 23, 2503. [Google Scholar] [CrossRef]
- Eggers, B.; Marciniak, J.; Memmert, S.; Kramer, F.J.; Deschner, J.; Nokhbehsaim, M. The Beneficial Effect of Cold Atmospheric Plasma on Parameters of Molecules and Cell Function Involved in Wound Healing in Human Osteoblast-like Cells in Vitro. Odontology 2020, 108, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Kleineidam, B.; Nokhbehsaim, M.; Deschner, J.; Wahl, G. Effect of Cold Plasma on Periodontal Wound Healing-an in Vitro Study. Clin. Oral Investig. 2019, 23, 1941–1950. [Google Scholar] [CrossRef]
- Delben, J.A.; Zago, C.E.; Tyhovych, N.; Duarte, S.; Vergani, C.E. Effect of Atmospheric-Pressure Cold Plasma on Pathogenic Oral Biofilms and In Vitro Reconstituted Oral Epithelium. PLoS ONE 2016, 11, e0155427. [Google Scholar] [CrossRef]
- Schmidt, A.; von Woedtke, T.; Vollmar, B.; Hasse, S.; Bekeschus, S. Nrf2 Signaling and Inflammation Are Key Events in Physical Plasma-Spurred Wound Healing. Theranostics 2019, 9, 1066–1084. [Google Scholar] [CrossRef] [PubMed]
- Lou, B.-S.; Hsieh, J.-H.; Chen, C.-M.; Hou, C.-W.; Wu, H.-Y.; Chou, P.-Y.; Lai, C.-H.; Lee, J.-W. Helium/Argon-Generated Cold Atmospheric Plasma Facilitates Cutaneous Wound Healing. Front. Bioeng. Biotechnol. 2020, 8, 683. [Google Scholar] [CrossRef] [PubMed]
- Shao, P.-L.; Liao, J.-D.; Wu, S.-C.; Chen, Y.-H.; Wong, T.-W. Microplasma Treatment versus Negative Pressure Therapy for Promoting Wound Healing in Diabetic Mice. Int. J. Mol. Sci. 2021, 22, 10266. [Google Scholar] [CrossRef] [PubMed]
- Eggers, B.; Marciniak, J.; Deschner, J.; Stope, M.B.; Mustea, A.; Kramer, F.-J.; Nokhbehsaim, M. Cold Atmospheric Plasma Promotes Regeneration-Associated Cell Functions of Murine Cementoblasts In Vitro. Int. J. Mol. Sci. 2021, 22, 5280. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.S.; Cho, Y.S.; Joo, S.Y.; Mun, C.H.; Seo, C.H.; Kim, J.-B. Wound Healing Potential of Low Temperature Plasma in Human Primary Epidermal Keratinocytes. Tissue Eng. Regen. Med. 2019, 16, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Eggers, B.; Stope, M.B.; Mustea, A.; Nokhbehsaim, M.; Heim, N.; Kramer, F.-J. Non-Invasive Physical Plasma Treatment after Tooth Extraction in a Patient on Antiresorptive Medication Promotes Tissue Regeneration. Appl. Sci. 2022, 12, 3490. [Google Scholar] [CrossRef]
- Park, J.; Lee, H.; Lee, H.J.; Kim, G.C.; Kim, S.-S.; Han, S.; Song, K. Non-Thermal Atmospheric Pressure Plasma Is an Excellent Tool to Activate Proliferation in Various Mesoderm-Derived Human Adult Stem Cells. Free Radic. Biol. Med. 2019, 134, 374–384. [Google Scholar] [CrossRef]
- Liu, J.-R.; Xu, G.-M.; Shi, X.-M.; Zhang, G.-J. Low Temperature Plasma Promoting Fibroblast Proliferation by Activating the NF-ΚB Pathway and Increasing CyclinD1 Expression. Sci. Rep. 2017, 7, 11698. [Google Scholar] [CrossRef] [Green Version]
- Soo, C.; Shaw, W.W.; Zhang, X.; Longaker, M.T.; Howard, E.W.; Ting, K. Differential Expression of Matrix Metalloproteinases and Their Tissue-Derived Inhibitors in Cutaneous Wound Repair. Plast. Reconstr. Surg. 2000, 105, 638–647. [Google Scholar] [CrossRef]
- Nuytinck, L.; Freund, M.; Lagae, L.; Pierard, G.E.; Hermanns-Le, T.; De Paepe, A. Classical Ehlers-Danlos Syndrome Caused by a Mutation in Type I Collagen. Am. J. Hum. Genet. 2000, 66, 1398–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayer, A.; Wijaya, B.; Möbus, L.; Rademacher, F.; Rodewald, M.; Tohidnezhad, M.; Pufe, T.; Drücke, D.; Gläser, R.; Harder, J. Platelet-Released Growth Factors and Platelet-Rich Fibrin Induce Expression of Factors Involved in Extracellular Matrix Organization in Human Keratinocytes. Int. J. Mol. Sci. 2020, 21, 4404. [Google Scholar] [CrossRef]
- Kim, H.-Y.; Agrahari, G.; Lee, M.J.; Tak, L.-J.; Ham, W.-K.; Kim, T.-Y. Low-Temperature Argon Plasma Regulates Skin Moisturizing and Melanogenesis-Regulating Markers through Yes-Associated Protein. Int. J. Mol. Sci. 2021, 22, 1895. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.-S.; Kim, Y.H.; Choi, E.H.; Kim, C.-K.; Kim, K.-N.; Kim, K.-M. Non-Thermal Atmospheric Pressure Plasma Increased MRNA Expression of Growth Factors in Human Gingival Fibroblasts. Clin. Oral Investig. 2016, 20, 1801–1808. [Google Scholar] [CrossRef] [PubMed]
- Nokhbehsaim, M.; Nogueira, A.V.B.; Damanaki, A.; Dalagiorgou, G.; Eick, S.; Adamopoulos, C.; Piperi, C.; Basdra, E.K.; Papavassiliou, A.G.; Deschner, J. Regulation of Matrix Metalloproteinase-1 by Filifactor Alocis in Human Gingival and Monocytic Cells. Clin. Oral Investig. 2020, 24, 1987–1995. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.B.; Park, G.S.; Park, S.S.; Jang, Y.J.; Kim, K.H.; Kim, K.J.; Park, E.J. Effect of Platelet-Rich Plasma on Proliferation and Migration in Human Dermal Fibroblasts. J. Cosmet. Dermatol. 2019, 18, 1105–1112. [Google Scholar] [CrossRef]
- Haralambiev, L.; Wien, L.; Gelbrich, N.; Lange, J.; Bakir, S.; Kramer, A.; Burchardt, M.; Ekkernkamp, A.; Gümbel, D.; Stope, M.B. Cold Atmospheric Plasma Inhibits the Growth of Osteosarcoma Cells by Inducing Apoptosis, Independent of the Device Used. Oncol. Lett. 2020, 19, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Almeida-Ferreira, C.; Silva-Teixeira, R.; Gonçalves, A.C.; Marto, C.M.; Sarmento-Ribeiro, A.B.; Caramelo, F.; Botelho, M.F.; Laranjo, M. Cold Atmospheric Plasma Apoptotic and Oxidative Effects on MCF7 and HCC1806 Human Breast Cancer Cells. Int. J. Mol. Sci. 2022, 23, 1698. [Google Scholar] [CrossRef]
- Gümbel, D.; Suchy, B.; Wien, L.; Gelbrich, N.; Napp, M.; Kramer, A.; Ekkernkamp, A.; Daeschlein, G.; Stope, M.B. Comparison of Cold Atmospheric Plasma Devices’ Efficacy on Osteosarcoma and Fibroblastic In Vitro Cell Models. Anticancer Res. 2017, 37, 5407–5414. [Google Scholar]
- Schmidt, A.; Bekeschus, S.; Jarick, K.; Hasse, S.; von Woedtke, T.; Wende, K. Cold Physical Plasma Modulates P53 and Mitogen-Activated Protein Kinase Signaling in Keratinocytes. Oxid. Med. Cell. Longev. 2019, 2019, 7017363. [Google Scholar] [CrossRef] [Green Version]
- Weiss, M.; Barz, J.; Ackermann, M.; Utz, R.; Ghoul, A.; Weltmann, K.-D.; Stope, M.B.; Wallwiener, D.; Schenke-Layland, K.; Oehr, C.; et al. Dose-Dependent Tissue-Level Characterization of a Medical Atmospheric Pressure Argon Plasma Jet. ACS Appl. Mater. Interfaces 2019, 11, 19841–19853. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, K.-N. Effects of a Nonthermal Atmospheric Pressure Plasma Jet on Human Gingival Fibroblasts for Biomedical Application. Biomed Res. Int. 2016, 2016, 2876916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jablonowski, L.; Kocher, T.; Schindler, A.; Müller, K.; Dombrowski, F.; von Woedtke, T.; Arnold, T.; Lehmann, A.; Rupf, S.; Evert, M.; et al. Side Effects by Oral Application of Atmospheric Pressure Plasma on the Mucosa in Mice. PLoS ONE 2019, 14, e0215099. [Google Scholar] [CrossRef] [Green Version]
- Evert, K.; Kocher, T.; Schindler, A.; Müller, M.; Müller, K.; Pink, C.; Holtfreter, B.; Schmidt, A.; Dombrowski, F.; Schubert, A.; et al. Repeated Exposure of the Oral Mucosa over 12 Months with Cold Plasma Is Not Carcinogenic in Mice. Sci. Rep. 2021, 11, 20672. [Google Scholar] [CrossRef]
- Jensen, J.-O.; Schulz, L.; Schleusser, S.; Matzkeit, N.; Stang, F.H.; Mailaender, P.; Kraemer, R.; Kleemann, M.; Deichmann, H.; Kisch, T. The Repetitive Application of Cold Atmospheric Plasma (CAP) Improves Microcirculation Parameters in Chronic Wounds. Microvasc. Res. 2021, 138, 104220. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Pan, J.; Ye, G.; Zhang, Q.; Wang, J.; Zhang, J.; Fang, J. In Vitro Studies of the Antimicrobial Effect of Non-Thermal Plasma-Activated Water as a Novel Mouthwash. Eur. J. Oral Sci. 2017, 125, 463–470. [Google Scholar] [CrossRef]
- Hoefeler, H.; Duran, I.; Hechmati, G.; Garzon Rodriguez, C.; Lüftner, D.; Ashcroft, J.; Bahl, A.; Atchison, C.; Wei, R.; Thomas, E.; et al. Health Resource Utilization Associated with Skeletal-Related Events in Patients with Bone Metastases: Results from a Multinational Retrospective—Prospective Observational Study—A Cohort from 4 European Countries. J. Bone Oncol. 2014, 3, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.; Simões, S.; Ascenso, A.; Reis, C.P. Therapeutic Advances in Wound Healing. J. Dermatol. Treat. 2022, 33, 2–22. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, H.-J.; Kim, H.K.; Hong, J.Y.; Cho, S.B. Effects of Argon and Nitrogen Plasma Pulses on the Skin and Skin Appendages in an in Vivo Animal Model. Skin Res. Technol. 2020, 26, 81–90. [Google Scholar] [CrossRef]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eggers, B.; Stope, M.B.; Marciniak, J.; Götz, W.; Mustea, A.; Deschner, J.; Nokhbehsaim, M.; Kramer, F.-J. Non-Invasive Physical Plasma Generated by a Medical Argon Plasma Device Induces the Expression of Regenerative Factors in Human Gingival Keratinocytes, Fibroblasts, and Tissue Biopsies. Biomedicines 2022, 10, 889. https://doi.org/10.3390/biomedicines10040889
Eggers B, Stope MB, Marciniak J, Götz W, Mustea A, Deschner J, Nokhbehsaim M, Kramer F-J. Non-Invasive Physical Plasma Generated by a Medical Argon Plasma Device Induces the Expression of Regenerative Factors in Human Gingival Keratinocytes, Fibroblasts, and Tissue Biopsies. Biomedicines. 2022; 10(4):889. https://doi.org/10.3390/biomedicines10040889
Chicago/Turabian StyleEggers, Benedikt, Matthias Bernhard Stope, Jana Marciniak, Werner Götz, Alexander Mustea, James Deschner, Marjan Nokhbehsaim, and Franz-Josef Kramer. 2022. "Non-Invasive Physical Plasma Generated by a Medical Argon Plasma Device Induces the Expression of Regenerative Factors in Human Gingival Keratinocytes, Fibroblasts, and Tissue Biopsies" Biomedicines 10, no. 4: 889. https://doi.org/10.3390/biomedicines10040889