
Abstract
Background
Esophagectomy with lymphadenectomy is the principal treatment for localized esophageal cancer. Conventional minimally invasive esophagectomy (C-MIE) in prone position has spread worldwide as it is less invasive. However, its efficacy remains controversial. Robot-assisted MIE (RAMIE) can have more advantages than C-MIE. Therefore, the current study aimed to validate whether RAMIE is associated with lower incidence of left recurrent laryngeal nerve (RLN) palsy compared with C-MIE in prone position.
Patients and Methods
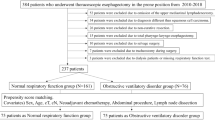
In total, 404 patients with esophageal carcinoma underwent MIE (353 C-MIEs and 51 RAMIEs) in prone position at Kobe University between 2010 and 2020. Then, propensity score matching was performed, and results showed that 51 patients should be included in each group. Thereafter, the perioperative outcomes between the two groups were compared.
Results
The RAMIE group had a significantly longer operative time than the C-MIE group (P < 0.0001). However, the number of lymph nodes resected along the left RLN was similar in both groups. Moreover, the incidence of left RLN palsy was significantly lower in the RAMIE group than in the C-MIE [Clavien–Dindo classification grade II; 0 (0%) versus 32 (9%), P = 0.022 in entire cohort, and 0 (0%) versus 5 (10%), P = 0.022 in matched cohort. Esophagectomy Complications Consensus Group definitions type I; 8 (16%) versus 101 (29%), P = 0.041 in entire cohort and 8 (16%) versus 18 (35%) in matched cohort, P = 0.023].
Conclusion
RAMIE is superior to C-MIE in prone position in decreasing the incidence of left RLN palsy.

Similar content being viewed by others


References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Smyth EC, Lagergren J, Fitzgerald RC, et al. Oesophageal cancer. Nat Rev Dis Primers. 2017;3:17048.
Altorki NK, Zhou XK, Stiles B, et al. Total number of resected lymph nodes predicts survival in esophageal cancer. Ann Surg. 2008;248:221–6.
Rizk NP, Ishwaran H, Rice TW, et al. Optimum lymphadenectomy for esophageal cancer. Ann Surg. 2010;251:46–50.
Palanivelu C, Prakash A, Senthilkumar R, et al. Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position-experience of 130 patients. J Am Coll Surg. 2006;203:7–16.
Cuschieri A, Shimi S, Banting S. Endoscopic oesophagectomy through a right thoracoscopic approach. J R Coll Surg Edinb. 1992;37:7–11.
Baba Y, Yoshida N, Shigaki H, et al. Prognostic impact of postoperative complications in 502 patients with surgically resected esophageal squamous cell carcinoma: a retrospective single-institution study. Ann Surg. 2016;264:305–11.
Oshikiri T, Takiguchi G, Hasegawa H, et al. Postoperative recurrent laryngeal nerve palsy is associated with pneumonia in minimally invasive esophagectomy for esophageal cancer. Surg Endosc. 2021;35:837–44.
Oshikiri T, Yasuda T, Harada H, et al. A new method (the “Bascule method”) for lymphadenectomy along the left recurrent laryngeal nerve during prone esophagectomy for esophageal cancer. Surg Endosc. 2015;29:2442–50.
Oshikiri T, Nakamura T, Hasegawa H, et al. Reliable surgical techniques for lymphadenectomy along the left recurrent laryngeal nerve during thoracoscopic esophagectomy in the prone position. Ann Surg Oncol. 2017;24:1018.
Yang Y, Zhang X, Li B, et al. Short- and mid-term outcomes of robotic versus thoraco-laparoscopic McKeown esophagectomy for squamous cell esophageal cancer: a propensity score-matched study. Dis Esophagus. 2020;33(6):doz080.
He H, Wu Q, Wang Z, et al. Short-term outcomes of robot-assisted minimally invasive esophagectomy for esophageal cancer: a propensity score matched analysis. J Cardiothorac Surg. 2018;13:52.
Deng HY, Luo J, Li SX, et al. Does robot-assisted minimally invasive esophagectomy really have the advantage of lymphadenectomy over video-assisted minimally invasive esophagectomy in treating esophageal squamous cell carcinoma? A propensity score-matched analysis based on short-term outcomes. Dis Esophagus. 2019;32(7):doy110.
Zhang Y, Han Y, Gan Q, et al. Early outcomes of robot-assisted versus thoracoscopic-assisted Ivor Lewis esophagectomy for esophageal cancer: a propensity score-matched study. Ann Surg Oncol. 2019;26:1284–91.
Chao YK, Hsieh MJ, Liu YH, Liu HP. Lymph node evaluation in robot-assisted versus video-assisted thoracoscopic esophagectomy for esophageal squamous cell carcinoma: a propensity-matched analysis. World J Surg. 2018;42:590–8.
Chen J, Liu Q, Zhang X, et al. Comparisons of short-term outcomes between robot-assisted and thoraco-laparoscopic esophagectomy with extended two-field lymph node dissection for resectable thoracic esophageal squamous cell carcinoma. J Thorac Dis. 2019;11:3874–80.
Oshikiri T, Takiguchi G, Urakawa N, et al. Novel “Modified Bascule method” for lymphadenectomy along the left recurrent laryngeal nerve during robot-assisted minimally invasive esophagectomy. Ann Surg Oncol. 2021. https://doi.org/10.1245/s10434-021-09738-w.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. 1983;70:41–55.
Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors. 8th edn. Oxford: Wiley; 2017.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Low DE, Alderson D, Cecconello I, et al. International consensus on standardization of data collection for complications associated with esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann Surg. 2015;262:286–94.
Weijs TJ, Seesing MF, van Rossum PS, et al. Internal and external validation of a multivariable model to define hospital-acquired pneumonia after esophagectomy. J Gastrointest Surg. 2016;20:680–7.
van der Sluis PC, van der Horst S, May AM, et al. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer: a randomized controlled trial. Ann Surg. 2019;269:621–30.
Jin D, Yao L, Yu J, et al. Robotic-assisted minimally invasive esophagectomy versus the conventional minimally invasive one: a meta-analysis and systematic review. Int J Med Robot. 2019;15(3):e1988.
Li XK, Xu Y, Zhou H, et al. Does robot-assisted minimally invasive oesophagectomy have superiority over thoraco-laparoscopic minimally invasive oesophagectomy in lymph node dissection? Dis Esophagus. 2021;34(2):doaa050.
Otsuka K, Murakami M, Goto S, et al. Minimally invasive esophagectomy and radical lymph node dissection without recurrent laryngeal nerve paralysis. Surg Endosc. 2020;34:2749–57.
Kim DJ, Park SY, Lee S, Kim HI, Hyung WJ. Feasibility of a robot-assisted thoracoscopic lymphadenectomy along the recurrent laryngeal nerves in radical esophagectomy for esophageal squamous carcinoma. Surg Endosc. 2014;28:1866–73.
Pelosi P, Croci M, Calappi E, et al. The prone positioning during general anesthesia minimally affects respiratory mechanics while improving functional residual capacity and increasing oxygen tension. Anesth Analg. 1995;80:955–60.
Otsubo D, Nakamura T, Yamamoto M, et al. Prone position in thoracoscopic esophagectomy improves postoperative oxygenation and reduces pulmonary complications. Surg Endosc. 2017;31:1136–41.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Oshikiri, T., Goto, H., Horikawa, M. et al. Incidence of Recurrent Laryngeal Nerve Palsy in Robot-Assisted Versus Conventional Minimally Invasive McKeown Esophagectomy in Prone Position: A Propensity Score-Matched Study. Ann Surg Oncol 28, 7249–7257 (2021). https://doi.org/10.1245/s10434-021-10123-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10123-w