
Abstract
Background
Our objective was to set up a more objective quantitative laparoscopy-based model in predicting the chances of optimal cytoreductive surgery in advanced ovarian cancer patients.
Methods
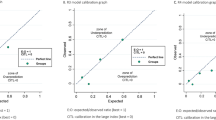
Sixty-four advanced ovarian cancer patients were submitted to both laparoscopy and standard longitudinal laparotomy sequentially, to define the chances of optimal debulking surgery (residual disease ≤1 cm). Three patients could not be evaluated by laparoscopy because of the presence of multiple and tenacious adherences. Sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy were calculated for each laparoscopic parameter. On the basis of the statistical probability of each factor to predict surgical outcome, seven laparoscopic features were selected for inclusion in the final model. Each parameter was assigned a numerical score based on the strength of statistical association, and a total predictive index value was tabulated for each patient. Receiver operating characteristic curve analysis was used to assess the ability of the model to predict surgical outcome.
Results
After debulking surgery, 41 (67.2%) of 61 patients were left with optimal residual disease. The presence of omental cake, peritoneal carcinosis, diaphragmatic carcinosis, mesenteric retraction, bowel and/or stomach infiltration, and liver metastases satisfied the basic inclusion criteria and were assigned a final predictive index value of 2. In the final model, a predictive index score ≥8 identified patients undergoing suboptimal surgery with a specificity of 100%. The positive predictive value was 100%, and the negative predictive value was 70%.
Conclusions
The reliability of laparoscopy in assessing the chance of optimal cytoreduction can be improved by using a simple scoring system.

Similar content being viewed by others


References
Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: a prospective study. Gynecol Oncol 1998; 69:103–8
Nelson BE, Rosenfield AT, Schwartz PE. Preoperative abdominopelvic computed tomographic prediction of optimal cytoreduction in epithelial ovarian carcinoma. J Clin Oncol 1993; 11:166–72
Meyer JI, Kennedy AW, Friedman R, Ayoub A, Zepp RC. Ovarian carcinoma: value of CT in predicting success of debulking surgery. Am J Roentgenol 1995; 165:875–8
Bristow RE, Duska LR, Lambrou NC, et al. A model for predicting surgical outcome in patient with advanced ovarian carcinoma using computed tomography. Cancer 2000; 89:1532–40
Fagotti A, Fanfani F, Ludovisi M, et al. Role of laparoscopy to assess the chance of optimal cytoreductive surgery in advanced ovarian cancer patients: a pilot study. Gynecol Oncol 2005; 96:729–35
Fanfani F, Ferrandina G, Corrado G, et al. Impact of interval debulking surgery on clinical outcome in primary unresectable FIGO stage IIIc ovarian cancer patients. Oncology 2003; 65:316–22
Eisenkop SM, Spirtos NM. What are the current surgical objectives, strategies, and technical capabilities of gynecologic oncologist treating advanced epithelial ovarian cancer ? Gynecol Oncol 2001; 82:489–97
Hanley JA, McNeil B. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982; 143:29–36
Vergote I, De Wever I, Tjalma W, Van Gramberen M, Decloedt J, Van Dam P. Neoadjuvant chemotherapy or primary debulking surgery in advanced ovarian carcinoma: a retrospective analysis of 285 patients. Gynecol Oncol 1998; 71:431–6
van der Burg MEL, van Lent M, Buyse M, et al. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. N Engl J Med 1995; 332:629–34
Ansquer Y, Leblanc E, Clough K, et al. Neoadjuvant chemotherapy for unresectable ovarian carcinoma: a French multicenter study. Cancer 2001; 1:2329–34
Mazzeo F, Berliere M, Kerger J, et al. Neoadjuvant chemotherapy followed by surgery and adjuvant chemotherapy in patients with primarily unresectable, advanced-stage ovarian cancer. Gynecol Oncol 2003; 90:163–9
Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20:1248–59
D’Ugo DM, Pende V, Persiani R, Rausei S, Picciocchi A. Laparoscopic staging of gastric cancer: an overview. J Am Coll Surg 2003; 196:965–74
Blackshaw GR, Barry JD, Edwards P, Allison MC, Thomas GV, Lewis WG. Laparoscopy significantly improves the perceived preoperative stage of gastric cancer. Gastric Cancer 2003; 6:225–9
Schneider A, Hertel H. Surgical and radiographic staging in patients with cervical cancer. Curr Opin Obstet Gynecol 2004; 16:11–8
Chung HH, Lee S, Sim JS, et al. Pretreatment laparoscopic surgical staging in locally advanced cervical cancer: preliminary results in Korea. Gynecol Oncol 2005; 95:468–75
Byrom J, Widjaja E, Redman CWE, Jones PW, Tebby S. Can pre-operative computed tomography predict resectability of ovarian carcinoma at primary laparotomy? Br J Obstet Gynecol 2002; 109:369–75
Qayyum A, Coakley FV, Westphalen AC, Hricak H, Okuno WT, Powell B. Role of CT and MR imaging in predicting optimal cytoreduction of newly diagnosed primary epithelial ovarian cancer. Gynecol Oncol 2005; 96:301–6
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fagotti, A., Ferrandina, G., Fanfani, F. et al. A Laparoscopy-Based Score To Predict Surgical Outcome in Patients With Advanced Ovarian Carcinoma: A Pilot Study. Ann Surg Oncol 13, 1156–1161 (2006). https://doi.org/10.1245/ASO.2006.08.021
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2006.08.021