
Abstract
Objective
To compare the safety and regression rates of conservative treatments for complex atypical hyperplasia (CAH) between pre- and postmenopausal women.
Methods
Historical cohort study of pre- and postmenopausal women with CAH managed conservatively at one center (Royal Women’s Hospital, Melbourne, Australia) between September 1999 to June 2012.
Results
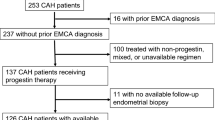
Of the 153 women with CAH, 92 (60%) underwent hysterectomy and the remaining 61 were managed conservatively with oral or intrauterine progestogen: 42 were premenopausal and 19 were postmenopausal. Within 12 months, 32 (76%) premenopausal women demonstrated regression of CAH and none developed endometrial cancer. In contrast, only 4 (21%) postmenopausal women showed disease regression and 4 (21%) progressed to endometrial cancer. Over a median of 24 months, 3 premenopausal women relapsed with CAH and 2 developed endometrial cancer. Four premenopausal women had successful pregnancies.
Conclusion
Conservative treatment with progestogen in premenopausal women with CAH leads to high regression rates within the first 12 months. In contrast, postmenopausal women have high rates of ongoing disease and cancer progression and conservative therapy should be avoided.
Similar content being viewed by others


References
Ayman E, Alfhaily F. Use of levonorgestrel-releasing intrauterine system in the prevention and treatment of endometrial hyperplasia. Obstet Gynaecol Surv. 2012;67(11):726–733.
Benshushan A. Endometrial adenocarcinoma in young patients: evaluation and fertility-preserving treatment. Eur J Obstet Gynecol Reprod Biol. 2004;117(2):132–137.
Cade TJ, Quinn MA, Rome RM, Neesham D. Progestogen treatment options for early endometrial cancer. BJOG. 2010;117(7):879–884.
Jadoul P, Donnez J. Conservative treatment may be beneficial for young women with atypical endometrial hyperplasia or endometrial adenocarcinoma. Fertil Steril. 2003;80(6):1315–1324.
Kaku T, Yoshikawa H, Tsuda H. Conservative therapy for adenocarcinoma and atypical endometrial hyperplasia of the endometrium in young women: central pathologic review and treatment outcome. Cancer Lett. 2001;167(1):39–48.
Travassoli FA. World Health Organisation Classification of Tumors: Pathology and Genetics of Tumors of the Breast and Female Genital Organs. Lyon, France: IARC Press; 2003.
Trimble CL, Kauderer J, Zaino R, et al. Concurrent endometrial carcinoma in women with a biopsy diagnosis of atypical endometrial hyperplasia; a gynaecologic oncology group study. Cancer. 2006;106(4):812–819.
Pennant S, Manek S, Kehoe S. Endometrial atypical hyperplasia and subsequent diagnosis of endometrial cancer: a retrospective audit and literature review. J Obstet Gynaecol. 2008;28(6):632–623.
Zaino RJ, Kauderer J, Trimble CL, et al. Reproducibility of the diagnosis of atypical endometrial hyperplasia: a gynecologic oncology group study. Cancer. 2006;106(4):804–811.
Clark TJ, Neelakantan D, Gupta JK. The management of endometrial hyperplasia: an evaluation of current practice. Eur J Obstet Gynecol Reprod Biol. 2006;125(2):259–264.
Randell IC, Kurman RJ. Progestin treatment of atypical hyperplasia and well-differentiated carcinoma of the endometrium in women under age 40. Obstet Gynecol. 1997:90(3):434–440.
Yamazawa K, Hirai M, Fujrto A, et al. Fertility-preserving treatment with progestin and pathological criteria to predict responses in young women with endometrial cancer. Hum Reprod. 2007;22(7):1953–158.
Orbo A, Arnes M, Hancke C, Vereide AB, Pettersen I, Larsen K. Treatment results of endometrial hyperplasia after prospective D-score classification: a follow up study comparing effect of LNG-IUD and oral progestins versus observation only. Gynecol Oncol. 2008;111(1):68–73.
Ushijima K, Yahata H, Yoshikawa H, et al. Multicentre phase II study of fertility-sparing treatment with medroxyprogesterone acetate for endometrial carcinoma and atypical hyperplasia in young women. J Clin Oncol. 2007;25(19):2798–2803.
Gallos ID, Yap J, Rajkhowa M, Luesley D, Coomarasamy A, Gupta JK. Regression, relapse, and live birth rates with fertilitysparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol. 2012;207(4):266.e1–e12.
Gallos ID, Shehmar M, Thangaratinam S, Papapostolou TK, Coomarasamy A, Gupta JK. Oral progestogens vs levonorgestrelreleasing intrauterine system for endometrial hyperplasia: a systematic review and meta-analysis. Am J Obstet Gynecol. 2010;203(6):547.e1–e10.
Gallos ID, Ganesan R, Gupta JK. Prediction of regression and relapse of endometrial hyperplasia with conservative therapy. Am J Obstet Gynecol. 2013;121(6):1165–1171.
Gallos ID, Krishan P, Shehmar M, Ganesan R, Gupta JK. Relapse of endometrial hyperplasia after conservative treatment: a cohort study with long term follow up. Hum Reprod. 2013;28(5):1231–1236.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Brownfoot, F.C., Hickey, M., Ang, W.C. et al. Complex Atypical Hyperplasia of the Endometrium: Differences in Outcome Following Conservative Management of Pre- and Postmenopausal Women. Reprod. Sci. 21, 1244–1248 (2014). https://doi.org/10.1177/1933719114522517
Published:
Issue Date:
DOI: https://doi.org/10.1177/1933719114522517