
Abstract
Purpose
The purpose of this work was to evaluate the results of high-dose radiation treatment using carbon ion therapy, alone or combined with intensity-modulated radiation treatment (IMRT), in patients with sacral chordoma.
Materials and methods
Between 2009 and 2012, 56 patients with sacral chordoma were treated in our center. The tumor was located above S3 in 33 patients and in S3 or below in 23 patients. In all, 41 patients received radiation therapy for the primary tumor, while 15 patients were treated for the recurrent tumor. Toxicity was measured using NCI CTCAE v.4.03. Local control (LC) and overall survival (OS) were evaluated with the Kaplan–Meier method.
Results
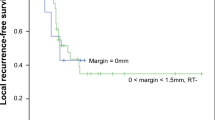
A total of 23 patients were irradiated with carbon ions in combination with photon IMRT, while 33 received carbon ion therapy only. Forty-three patients had a macroscopic tumor at treatment start with a median tumor size (GTV) of 244 ml (range 5–1188 ml). The median total dose was 66 Gy (range 60–74 Gy; RBE). After a median follow-up time of 25 months, the 2- and 3-year local control probability was 76 % and 53 %, respectively. The overall survival rate was 100 %. Treatment for primary tumor and male patients resulted in significant better local control. No higher toxicity occurred within the follow-up time.
Conclusion
High-dose photon/carbon ion beam radiation therapy is safe and, especially for primary sacral chordomas, highly effective. A randomized trial is required to evaluate the role of primary definitive hypofractionated particle therapy compared with surgery with or without adjuvant radiotherapy.
Zusammenfassung
Zielsetzung
Evaluierung der Ergebnisse nach hochdosierter Kohlenstoffionentherapie, allein oder in Kombination mit einer intensitätsmodulierten Photonenbestrahlung (IMRT), bei Patienten mit einem sakralen Chordom.
Material und Methoden
Zwischen 2009 und 2012 wurden 56 Patienten mit sakralen Chordomen in unserem Zentrum behandelt. Der Tumor war bei 33 Patienten oberhalb von S3 und bei 23 Patienten auf Höhe von S3 oder unterhalb davon lokalisiert. Insgesamt wurden 41 Patienten innerhalb der Primärtherapie und 15 Patienten innerhalb einer Rezidivtherapie behandelt. Die Erfassung der Toxizität erfolgte gemäß NCI CTCAE v.4.03. Lokale Kontrolle (LC) und Gesamtüberleben (OS) wurden mithilfe der Kaplan-Meier-Methode bestimmt.
Ergebnisse
Insgesamt 23 Patienten wurden mit Kohlenstoffionen in Kombination mit Photonen-IMRT bestrahlt, während 33 eine alleinige Kohlenstoffionentherapie erhielten. Zu Beginn der Therapie hatten 43 Patienten einen makroskopischen Tumor mit einer medianen Tumorgröße (GTV) von 244 ml (5–1188 ml). Die applizierte mediane Gesamtdosis betrug 66 Gy (60–74 Gy; RBE). Nach einer medianen Nachbeobachtungszeit von 25 Monaten lag die 2- und 3-Jahres-LC bei 76% bzw. 53%. Die OS-Rate betrug 100%. Die Behandlung innerhalb der Primärtherapie und männlichen Patienten zeigten eine signifikant bessere LC. Die Behandlung führte zu keiner höhergradigen Toxizität.
Schlussfolgherung
Eine hochdosierte Strahlentherapie mit Photonen bzw. Kohlenstoffionen ist sicher durchführbar und ist, vor allem innerhalb der Primärtherapie eines sakralen Chordoms, sehr effektiv. Eine randomisierte Studie ist erforderlich, um die Rolle der primären definitiven hypofraktionierten Partikeltherapie im Vergleich zu einer operativen Therapie mit oder ohne adjuvante Strahlentherapie zu evaluieren.





Similar content being viewed by others

References
Salisbury JR, Deverell MH, Cookson MJ et al (1993) Three-dimensional reconstruction of human embryonic notochords: clue to the pathogenesis of chordoma. J Pathol 171:59–62
Smoll NR, Gautschi OP, Radovanovic et al (2013) Incidence and relative survival of chordomas: the standardized mortality ratio and the impact of chordomas on a population. Cancer 119:2029–2037
Chen KW, Yang HL, Lu J et al (2010) Prognostic factors of sacral chordoma after surgical therapy: a study of 36 patients. Spinal Cord 48:166–171
Cheng EY, Ozerdemoglu RA, Transfeldt EE et al (1999) Lumbosacral chordoma. Prognostic factors and treatment. Spine (Phila Pa 1976) 24:1639–1645
Fuchs B, Dickey ID, Yaszemski MJ et al (2005) Operative management of sacral chordoma. J Bone Joint Surg Am 87:2211–2216
Osaka S, Kodoh O, Sugita H et al (2006) Clinical significance of a wide excision policy for sacrococcygeal chordoma. J Cancer Res Clin Oncol 132:213–218
Stener B, Gunterberg B (1978) High amputation of the sacrum for extirpation of tumors. Principles and technique. Spine (Phila Pa 1976) 3:351–366
Devin C, Chong PY, Holt GE et al (2006) Level-adjusted perioperative risk of sacral amputations. J Surg Oncol 94:203–211
Hsieh PC, Xu R, Sciubba DM et al (2009) Long-term clinical outcomes following en bloc resections for sacral chordomas and chondrosarcomas: a series of twenty consecutive patients. Spine (Phila Pa 1976) 34:2233–2239
Davidge KM, Eskicioglu C, Lipa J et al (2010) Qualitative assessment of patient experiences following sacrectomy. J Surg Oncol 101:447–450
Hulen CA, Temple HT, Fox WP et al (2006) Oncologic and functional outcome following sacrectomy for sacral chordoma. J Bone Joint Surg Am 88:1532–1539
York JE, Kaczaraj A, Abi-Said D et al (1999) Sacral chordoma: 40-year experience at a major cancer center. Neurosurgery 44:74–79; discussion 9–80
Lee SU, Park JW, Kim TH et al (2014) Effectiveness and safety of proton beam therapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Strahlenther Onkol 190:806–814
Demizu Y, Fujii O, Terashima K et al (2014) Particle therapy for mucosal melanoma of the head and neck. A single-institution retrospective comparison of proton and carbon ion therapy. Strahlenther Onkol 190:186–191
Mizumoto M, Okumura T, Ishikawa E et al (2013) Reirradiation for recurrent malignant brain tumor with radiotherapy or proton beam therapy. Technical considerations based on experience at a single institution. Strahlenther Onkol 189:656–663
Durante M, Loeffler JS (2010) Charged particles in radiation oncology. Nat Rev Clin Oncol 7:37–43
Uhl M, Mattke M, Welzel T et al (2014) High control rate in patients with chondrosarcoma of the skull base after carbon ion therapy: first report of long-term results. Cancer 120:1579–1585
Uhl M, Mattke M, Welzel T et al (2014) Highly effective treatment of skull base chordoma with carbon ion irradiation using a raster scan technique in 155 patients: first long-term results. Cancer 120:3410–3417
Uhl M, Edler L, Jensen AD et al (2014) Randomized phase II trial of hypofractionated proton versus carbon ion radiation therapy in patients with sacrococcygeal chordoma—the ISAC trial protocol. Radiat Oncol 9:100
Schulz-Ertner D, Nikoghosyan A, Didinger B et al (2005) Therapy strategies for locally advanced adenoid cystic carcinomas using modern radiation therapy techniques. Cancer 104:338–344
Uhl M, Welzel T, Oelmann J et al (2014) Active raster scanning with carbon ions: reirradiation in patients with recurrent skull base chordomas and chondrosarcomas. Strahlenther Onkol 190:686–691
Park L, Delaney TF, Liebsch NJ et al (2006) Sacral chordomas: impact of high-dose proton/photon-beam radiation therapy combined with or without surgery for primary versus recurrent tumor. Int J Radiat Oncol Biol Phys 65:1514–1521
Chen YL, Liebsch N, Kobayashi W et al (2013) Definitive high-dose photon/proton radiotherapy for unresected mobile spine and sacral chordomas. Spine (Phila Pa 1976) 38:E930–E936
Mima M, Demizu Y, Jin D et al (2014) Particle therapy using carbon ions or protons as a definitive therapy for patients with primary sacral chordoma. Br J Radiol 87:20130512
Imai R, Kamada T, Sugahara S et al (2011) Carbon ion radiotherapy for sacral chordoma. Br J Radiol 84:Spec No 1:S48–S54
DeLaney TF, Liebsch NJ, Pedlow FX et al (2009) Phase II study of high-dose photon/proton radiotherapy in the management of spine sarcomas. Int J Radiat Oncol Biol Phys 74:732–739
Yanagi T, Kamada T, Tsuji H et al (2010) Dose-volume histogram and dose-surface histogram analysis for skin reactions to carbon ion radiotherapy for bone and soft tissue sarcoma. Radiother Oncol 95:60–65
Staab A, Rutz HP, Ares C et al (2011) Spot-scanning-based proton therapy for extracranial chordoma. Int J Radiat Oncol Biol Phys 81:e489–e496
Zabel-du Bois A, Nikoghosyan A, Schwahofer A et al (2010) Intensity modulated radiotherapy in the management of sacral chordoma in primary versus recurrent disease. Radiother Oncol 97:408–412
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Debus states that he is CEO of Heidelberg Ion Therapy Center (HIT). M. Uhl, T. Welzel, A. Jensen, M. Ellerbrock, T. Haberer, O. Jäkel, and K. Herfarth state that there are no conflicts of interest.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 (in its most recently amended version). Informed consent was obtained from all patients included in the study
Rights and permissions
About this article

Cite this article
Uhl, M., Welzel, T., Jensen, A. et al. Carbon ion beam treatment in patients with primary and recurrent sacrococcygeal chordoma. Strahlenther Onkol 191, 597–603 (2015). https://doi.org/10.1007/s00066-015-0825-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-015-0825-3