

Abstract
Background/Aim: To report the frequency of crypts in asymmetric branching (CAB) in biopsies from all colorectal segments in patients with ulcerative colitis in remission (UCR). Patients and Methods: Biopsies in 100 UC patients were investigated: 50 with UCR and 50 with ongoing long-lasting UC (LLU; i.e., controls). Results: The frequency of CAB was significantly lower in UCR than in LLUC, both in the right colon and left colorectum. CAB frequency was not influenced by two important confounders: the age and sex of patients. Conclusion: CAB is a pathologic aberration of colorectal cryptogenesis evoked by chronic mucosal inflammation. When chronic inflammation waned in UCR, the production of CAB plummeted or ceased. Chronic inflammation and protracted disease-duration in LLUC increase the risk for colorectal dysplasia or carcinoma. Importantly, dysplastic CAB were recently detected in LLUC-associated dysplasia. Whether the abrogation of CAB is instrumental in reducing the neoplastic risk in UCR patients, deserves further investigation.
- Colon biopsies
- crypts
- asymmetric branching
- ulcerative colitis
- remission
In patients with ulcerative colitis (UC), colorectal endoscopic biopsies show, in addition to increased numbers of inflammatory cells, crypts with architectural distortions and branching crypts (1, 2). Crypt-branching in rectal biopsies from patients with UC was first mentioned by Morson in 1972 (3). Subsequently, Cheng et al. (4) found high percentages of branching crypts in patients with UC, claiming that crypt branching featured increased crypt replication. Since then, numerous surveys concerning the histologic description of UC have mentioned crypt branching, without further comments (5-8). More recently, The British Society of Gastroenterology defined crypt branching when “two or more branched crypts” were found “in a well-oriented biopsy” (9). Crypt branching is often included in the narrative of crypt distortion in UC (5-8, 10).
It is generally accepted that UC has no definitive cure (10). However, medication often ameliorates or resolves the mucosal inflammation, and patients experience a period of remission that may last for weeks or years (8). To assess the degree of mucosal inflammation in UC, several histologic grading systems have been proposed; in fact, nearly 30 histological scoring indices for UC were listed in the Cochrane Database (11). According to Lang-Schwarz et al. (2), “the ideal histological score should be able to assess not only disease activity but also restoration of chronic inflammation to normal”. Today, the Geboes grading system for UC is mostly used (12); it is based on structural (architectural change), chronic inflammatory infiltrate, lamina propria neutrophils and eosinophils, neutrophils in epithelium, crypt destruction, and erosions or ulcerations.
However, none of the aforementioned grading systems includes the histologic characteristics of branching crypts in UC. In previous publications, we described in detail, the histologic characteristics of crypt branching in UC (13-16). These studies, based on single colonic biopsies in patients with UC showed two histologic phenotypes of branching crypts: i) crypts in symmetric branching (CSB) and ii) crypts in asymmetric branching (CAB). Quantitative studies disclosed that the frequency of biopsies showing CAB was significantly higher than that showing CSB (15, 16). Since CAB do not evolve in the normal colon of adults without inflammatory diseases (17), the finding of CAB in adults with UC is a remarkable event. The findings suggested that the presence of CAB underlined a pathologic disturbance in the colorectal mucosa in adult patients with UC (18). A review of the literature revealed no study regarding the presence of CAB and CSB in patients with UC in remission (UCR) (1-12, 19).
The purpose of the present survey was to explore whether CAB and CSB persisted or disappeared following waned UC-inflammation, in patients with UCR. Cases with long-lasting UC (LLUC) served as controls.
Patients and Methods
Patient selection. From the files of the Department of Pathology, Klinikum Bayreuth, 100 endoscopic biopsies from different colorectal sites were selected: 50 biopsies were from patients with UCR and the remaining 50 were from patients with LLUC. To investigate the possible influence of sex on the frequency of CAB and CSB, 50 out of the 100 cases were males and the remining 50, females. The possible influence of age and the localization in the colorectum on the frequency of CAB and CSB were also recorded.
Cases were diagnosed at the Department of Pathology, Klinikum Bayreuth, Fredrich-Alexander University, Erlangen-Nuremberg University, Bayreuth, Germany. Following the endoscopic scheme for UC, a minimum of two endoscopic biopsies were obtained from various colorectal segments in UC (Table I). In this work, the right colon comprised cecum, colon ascendent, and colon transversum, and the left colorectum, colon descendent, sigmoid colon, and rectum. Crypt branching found in biopsies in all colorectal segments was quantified.
The number of biopsies-sites obtained in different colorectal segments in 100 patients with ulcerative colitis (UC): 50 with ulcerative colitis in remission (UCR) and 50 with long-lasting ulcerative colitis (LLUC).
Biopsies were cut in 4 μm thick sections, stained with hematoxylin and eosin (H&E), and subsequently scanned with a Hamamatsu Nanozoomer S360 digital scanner (Hamamatsu, Herrsching am Ammersee, Germany). Digitalized scanned sections were made available via web interface. Definitions of CAB and CSB in UC have been reported elsewhere (16).
Ethics. Ethical approval was obtained from the Ethics Committee of Friedrich-Alexander University, Erlangen-Nuremberg, Germany, for validation of the IBD-DCA score (ID number: 175_20 Bc).
Statistical analysis. The non-parametric Mann-Whitney U two-tailed test was applied to compare differences between groups. The Pearson’s correlation coefficient was used to evaluate the possible linear association between two variables. Statistical significance was defined as p<0.05.
Results
Frequency of CAB and CSB in UCR and in LLUC. In the 50 UCR cases, 123 branching crypts were found: 100 were CAB (mean 2.1, range=0-6) (Figure 1, upper panel) and 23 CSB (mean 0.46, rage=0-4). In the 50 LLUC cases, 208 branching crypts were found: 181 were CAB (mean 3.6, range=0-11) (Figure 1, lower panel), and 27 CSB (mean 0.54, range=0-4). Hence, CAB comprised the vast majority of the branching crypts in the 50 cases with UCR (81.9%) and of the branching crypts in the 50 cases with LLUC (87.0%). CAB, therefore, were chosen to test the influence of several possible confounders, such as age, sex, and localization of crypt branching in UCR and LLUC. The difference between CAB in UCR vs. LLUC was significant at p=0.00711.

{kind=link}
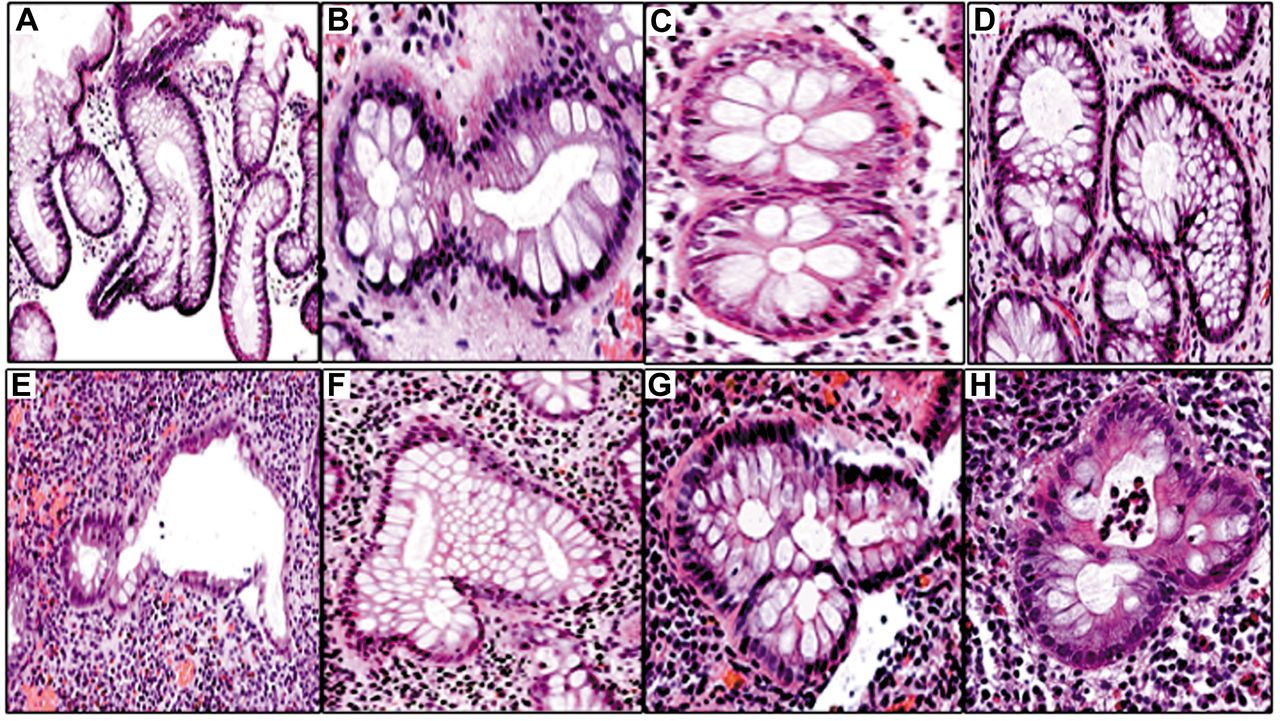
Upper panel. Examples of the spectrum of colon crypts in asymmetric branching (CAB) found in endoscopic biopsies from patients with ulcerative colitis in remission (UCR). Note the scarce round-cell infiltrate in the lamina propria (A: Well-oriented vertical crypt in asymmetric branching, H&E, original ×4). B, D: Cross-cut crypts in asymmetric branching. C: Cross-cut crypts in symmetric branching (H&E, B and C, original ×20, D ×10). Lower panel. E, F, G, H Cross-cut crypts in asymmetric branching showing two or more branching crypts in asymmetric branching found in biopsies from patients with long-lasting ulcerative colitis (LLUC). Note ongoing chronic inflammation in the lamina propria (H&E, E original ×10, F, G, H, original ×20).
Age. The mean age of the 50 patients with UCR was 51.3 years (range=24-82 years), and in the 50 patients with LLUC, it was 48.5 years (range=18-81 years). When the frequency of CAB in UCR and in LLUC was correlated with the age of the patients, no linear correlation was found; the result was not significant at p=0.610028.
Sex. In the 50 UCR male cases, a total of 126 CAB (mean 2.5 range=0-9) were found and in the 50 female cases, 155 CAB were registered (mean 3.1, range=0-11). When the frequency of CAB was correlated in males and females, the result was not significant at p=0.079847.
Localization of CAB in UCR and in LLUC. In UCR, 18 CAB (mean 0.78, range=0-8) were found in the right colon and 82 CAB (mean 3.03, range=0-8) were recorded in the left colorectum. The difference between the frequency of CAB in the right colon vs. the left colorectum in UCR, was significant at (p=0.00042) (Mann-Whitney U two-tailed test). In LLUC, 52 CAB (mean 4, range=0-9) were found in the right colon and 129 CAB (mean 5.2, range=1-11) were recorded in the left colorectum. The difference between the frequency of CAB in the right colon vs. the left colorectum in LLUC was significant (p=0.00042) (Mann-Whitney U two-tailed test).
The frequency of CAB was significantly lower in the right colon in UCR, than the frequency of CAB in the right colorectum in LLUC (p=0.01778, Mann-Whitney U two-tailed test). In similarity, the frequency of CAB was significantly lower in the left colorectum in UCR, than the frequency of CAB in the left colorectum in LLUC (p=0.00614, Mann-Whitney U two-tailed test).
Discussion
This study showed that CAB were significantly lower in UCR than in LLUC, suggesting that when the chronic inflammation in UC waned, the frequency of CAB recessed or was abrogated. Thirty-two biopsy-sites showed no CAB; of these, 23 (72%) were recorded in UCR and the remining 9 (28%) in LLUC. Thus, recession or abrogation of chronic inflammation in UCR seemed to have encouraged the “normalization” of crypt homeostasis. The cause for the absence of CAD in the 9 biopsy-sites with LLUC remains elusive.
The frequency of CAB in UCR was significantly lower, both in the right colon and left colorectum, than the frequency of CAB in LLUC in similar segments. However, the frequency of CAB was higher in the left colorectum than in the right colon, both in UCR and LLUC. The finding of CAB in the right colon in patients with UCR might imply either that the right colon in these patients was involved in the UC chronic inflammation before UC had entered the remission phase, or that CAB persisted following medical treatment.
Since the age and sex of the patients had no influence on the frequency of CAB in UCR and LLUC, the localization of the biopsy-site emerges as an important confounder variable that influenced the CAD frequency in different colorectal segments. Whether CAB in UCR eventually revert to crypts with normal configurations or persist as asymmetric branching crypts, is unclear. To answer this question, future investigations should probably include UCR-cases with long-lasting remission. The other question that deserves further investigation is why CAB plummeted in UCR. Is it because new CAB were not generated in UCR, or because CAB were generated, but at a slower pace than in LLUC? There was no indication that the failure to replicate more CAB in UCR was the result of crypt abrogation by apoptosis (20, 21). Since similar abnormal crypt branching is not found in the normal colorectal mucosa in adults (17), the presence CAB in the colonic mucosa in adult patients with UC substantiates the notion that these crypts are genuine pathologic aberrations of cryptogenesis. Fortunately, oral and local 5-ASA compounds and corticosteroids, or in more severe UC cases, tumour necrosis factor-α antibodies (infliximab) or immunomodulators (azathioprine, 6-mercaptopurine) (22), often ameliorate or abolish chronic inflammation resulting in a lower frequency of crypt branching, as shown in patients with UCR. However, in patients with poor response to medical treatment, the long-lasting chronic inflammation will probably continue to boost CAB production.
Chronic inflammation and protracted disease-duration in LLUC, increase the risk for colorectal dysplasia or carcinoma (22, 23). In this context, dysplastic CAB were recently detected in patients with LLUC-associate dysplasia (24).
In the present survey, we found that when chronic inflammation decreases in UCR, the production of CAB plummeted or ceased. Whether the abrogation of CAB is instrumental or contributes to reducing the neoplastic risk in UCR-patients, deserves to be further investigated. In this regard, no dysplastic crypts in asymmetric branching have been found in patients with UCR.
The study of CAB in endoscopic biopsies in patients with UCR offers several advantages: i) The frequency of CAB can easily be recorded at the time of routine diagnosis, in H&E-stained sections; ii) The frequency of CAB is not influenced by the age or sex in UC patients; iii) Immunostaining and molecular assays are not required for studies of the frequency and distribution of CAB in the colorectal mucosa in patients with UCR; iv) Possible variations in frequency of CAB in UCR can be registered in subsequent surveillance examination-biopsies in the same patient.
In summary, the frequency of CAB was significantly lower in patients with UCR than in patients with LLUC, strongly suggesting that in UCR patients, CAB recessed or were abrogated by the plummeting chronic mucosal inflammation. Routine endoscopic colorectal biopsies will prospectively be examined, as a method to monitor conceivable variations in CAB frequency in patients with UCR under surveillance.
Footnotes
Authors’ Contributions
Conception and design of the study: CAR Acquisition and analysis of data; MV, CLS, CAR. Drafting the manuscript and figures: CAR. Review and editing the manuscript: MV, CLS, CAR. Resources: MV, CLS, CAR. Supervision: CAR, MV.
Conflicts of Interest
The Authors declare no competing interests in relation to this study.
- Received June 19, 2022.
- Revision received July 8, 2022.
- Accepted July 12, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).