

Abstract
Background: For epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (NSCLC), administration of EGFR tyrosine kinase inhibitors (TKIs) is mandatory to prolong survival. To date, a comparison of second- and third-generation EGFR-TKIs has not been reported as far as we are aware. Patients and Methods: We retrospectively investigated the survival time of patients diagnosed with EGFR-mutated advanced or recurrent NSCLC who had received afatinib, a second-generation EGFR-TKI, or osimertinib, a third-generation EGFR-TKI, as the first-line treatment. Results: Among the 49 patients included in the study, 15 received afatinib and 34 received osimertinib. No significant differences in overall survival were observed between the two groups [afatinib vs. osimertinib=36 vs. 33 months (hazard ratio=2.917, 95% confidence interval=0.780-10.905; p=0.112)]. T790M mutation was detected in three of the patients in the afatinib group, and all three subsequently received osimertinib. The median overall survival of these three patients and of the 12 without the mutation were 63 and 36 months, respectively. Conclusion: There was no apparent difference in the effect on survival between second- and third-generation EGFR-TKIs, whereas the sequential administration of second- followed by third-generation EGFR-TKIs appeared to confer a better long-term prognosis.
- Epidermal growth factor receptor
- tyrosine kinase inhibitors
- non-small-cell lung cancer
Mutations in the epidermal growth factor receptor (EGFR) gene are important drivers of non-small-cell lung cancer (NSCLC). For EGFR mutation-positive NSCLC, administration of EGFR tyrosine kinase inhibitors (TKIs) remains crucial for prolonging survival. Currently approved EGFR-TKIs include first-generation gefitinib and erlotinib, second-generation afatinib and dacomitinib, and third-generation osimertinib.
Afatinib is an oral, irreversible blocker of the ERB-B2 receptor tyrosine kinase family of EGFR, EGFR2 (HER2⁄ERBB2), ERBB3, and ERBB4 signaling factors (1, 2). Afatinib demonstrated superior progression-free survival (PFS) in the LUX-Lung-7 trial, a comparative study with the first-generation EGFR-TKI gefitinib, and has been approved as first-line treatment for EGFR mutation-positive NSCLC (3). Although no statistical superiority was observed in terms of overall survival (OS), the median OS was longer following afatinib treatment (4). Subgroup analysis revealed that afatinib tended to afford better OS in patients with exon 19 deletion and patients with L858R mutation. Furthermore, both non-Asian and Asian patients tended to demonstrate better OS following afatinib therapy. Afatinib can be administered in any treatment line. Furthermore, the T790M EGFR mutation is a mechanism of resistance to afatinib (5), and in those cases, sequential administration of osimertinib may be expected to further prolong OS.
Osimertinib is a third-generation, irreversible, oral EGFR-TKI that selectively inhibits tumors with TKI-sensitizing and T790M resistance-associated EGFR mutations (6, 7). Osimertinib reportedly afforded superior PFS in the FLAURA trial, a comparative study of first-generation EGFR-TKIs gefitinib and erlotinib, and is currently recognized as first-line treatment as well as afatinib (8). Additionally, osimertinib outperformed first-generation EGFR-TKIs in terms of OS; however, subgroup analysis revealed no clear superiority in Asian and L858R EGFR mutational subgroups (9). Osimertinib is often used as the first-line treatment but cannot be administered after administration of first- or second-generation EGFR-TKIs unless the T790M mutation is detected. The mechanisms of resistance to osimertinib are diverse, including activation of collateral pathways such as secondary mutations in the EGFR gene, amplification of the MET gene, and transformation into other histological types, such as small-cell carcinoma and squamous cell carcinoma (10). Therefore, if resistance to osimertinib is detected, cytotoxic anticancer agents are usually administered.
Both afatinib and osimertinib demonstrated superior PFS compared with first-generation EGFR-TKIs in patients with EGFR mutation-positive NSCLC. Osimertinib, which is mildly toxic and elicits prolonged PFS, is often used as the first-line treatment. However, a direct comparison of efficacy and safety between afatinib and osimertinib has not been conducted to date, and such a study may be necessary in making informed clinical decisions, especially for Asians, as well as other patients with L858R mutation. Herein, we retrospectively evaluated the efficacy and safety of administering afatinib and osimertinib.
Patients and Methods
Patient selection. The present study included patients diagnosed with EGFR-mutated advanced or recurrent NSCLC who had received afatinib or osimertinib as first-line treatment at Osaka Medical and Pharmaceutical University Hospital between January 2014 and December 2019. Data analysis was conducted at the end of December 2020. We conducted a retrospective review of patient medical records after obtaining institutional approval from the review board of our hospital (approval number 2020-179). The study was carried out according to routine clinical practice, with no interventions undertaken for the purpose of this study; therefore, written informed consent was not required. Baseline patient characteristics at treatment initiation were collected from medical records. Data collected included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), smoking status, histology, clinical stage, presence of central nervous system metastasis, and type of EGFR mutation. Data regarding treatment were also collected, including the EGFR-TKI regimen used, tumor responses, and adverse events.
Treatment. Afatinib was initiated at 40 mg/day, and osimertinib was initiated at 80 mg/day. When adverse events were observed, the dose was reduced or the drug was withdrawn as appropriate; whenever unacceptable effects persisted, treatment was discontinued.
Efficacy and toxicity evaluation. PFS was defined as the date from the start of medication to the date of confirmation of exacerbation, the date of discontinuation of medication for some reason, or the date of death. OS was defined as the date from the start of medication to the date of last survival confirmation or death. The objective tumor response to treatment was determined based on the Response Evaluation Criteria for Solid Tumors version 1.1 (11). Toxicity data were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0 (12).
Statistical analysis. Differences in patient characteristics were analyzed using the Mann–Whitney U-test and chi-square test. PFS and OS were calculated using the Kaplan–Meier method. The Cox proportional hazard model was used to investigate the association between patient characteristics at treatment initiation and survival. All statistical analyses were performed using SPSS version 25 (IBM SPSS, Armonk, NY, USA). A two-sided value of p<0.05, was considered to indicate a statistically significant difference.
Results
Patients. Between January 2014 to December 2019, 49 patients were treated with afatinib or osimertinib as first-line treatment at our hospital. Among these patients, 15 received afatinib treatment and 34 received osimertinib treatment. The baseline characteristics of the 49 patients included in the analysis are shown in Table I.
Baseline patient characteristics.
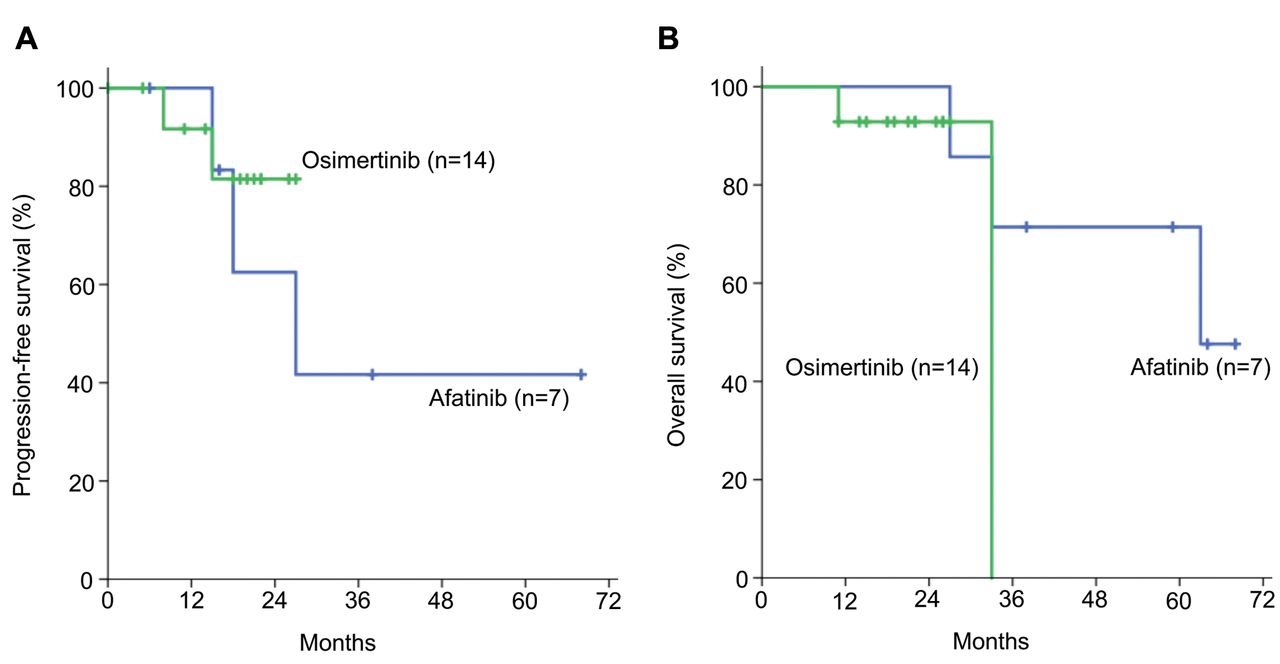
Efficacy. Kaplan–Meier curves for PFS and OS are shown in Figure 1. The median PFS was 23.0 months [95% confidence interval (CI)=14.2-31.8 months] under therapy with afatinib and was not estimable under osimertinib treatment [hazard ratio (HR)=0.932, 95% CI=0.379-2.287; p=0.877] (Figure 1A). The median OS was 36 (95% CI=2.9-69.1) months for the afatinib group and 33 months (95% CI=not estimable) for the osimertinib group (HR=2.917, 95% CI=0.780-10.905; p=0.112) (Figure 1B). No statistically significant differences in PFS and OS were observed between the two groups.

Progression-free (PFS) and overall (OS) survival for the whole patient cohort A: Kaplan–Meier estimates of the duration of PFS. Data for patients who had not experienced progression or had not died at the time of the analysis were censored when their last assessment was evaluated. B: Kaplan–Meier estimates of the duration of OS. Data for any patients who were not known to have died at the time of the analysis were censored at the last recorded date that the patient was known to be alive. Tick marks indicate censored data. No statistically significant difference in PFS and OS were observed between the two groups.
The best outcomes determined according to Response Evaluation Criteria for Solid Tumors guidelines were as follows for afatinib and osimertinib, respectively: one and no complete response, 10 and 23 partial responses (PR; 66.7% and 67.6%), four and 11 with stable disease (SD; 26.7% and 32.4%), and none with progressive disease (PD). The objective response rate was 73.3% and 67.6% for afatinib and osimertinib, respectively, and the disease control rate was 100%.
In patients with EGFR exon 19 deletion, the median PFS was 27 (95% CI=8.2-45.8) months for afatinib and not estimable for those treated with osimertinib (HR=0.500, 95% CI=0.078-3.207, p=0.465) (Figure 2A). The median OS was 63 months (95% CI=not estimable) in the afatinib group and 33 months (95% CI=not estimable) in the osimertinib group (HR=3.054, 95% CI=0.349-26.715; p=0.313) (Figure 2B). In patients with the EGFR L858R mutation, the median PFS was 8.0 (95% CI=0.0-16.0) months with afatinib and 13 (95% CI=7.6-18.4) months with osimertinib (HR=0.620, 95% CI=0.133-2.899, p=0.543) (Figure 3A). The median OS was 34 months (95% CI=0.0-68.4) with afatinib and 17 (95% CI=12.2-21.8) months with osimertinib (HR=2.958, 95% CI=0.359-24.385, p=0.314) (Figure 3B). In the analysis for each mutation type, no statistically significant differences in PFS and OS were observed between the two groups.
Progression-free (PFS) and overall (OS) survival in patients with epidermal growth factor receptor (EGFR) exon 19 deletion. A: Kaplan– Meier estimates of the duration of PFS in patients with an EGFR exon 19 deletion mutation. Patients who had survived and had no disease progression at the time of analysis were censored at the time of their last evaluable assessment. B: Kaplan–Meier estimates of the duration of OS in patients with EGFR exon 19 deletion. Patients who were not known to have died at the time of the analysis were censored at the last recorded date that the patient was known to be alive. Tick marks indicate censored data. No statistically significant difference in PFS and OS were observed between the two groups.

Progression-free (PFS) and overall (OS) survival in patients with epidermal growth factor receptor (EGFR) L858R mutation. A: Kaplan– Meier estimates of the duration of PFS in patients with EGFR L858R mutation. Patients who had survived and had no disease progression at the time of analysis were censored at the time of their last evaluable assessment. B: Kaplan–Meier estimates of the duration of OS in patients with EGFR L858R mutation. Patients who were not known to have died at the time of the analysis were censored at the last recorded date that the patient was known to be alive. Tick marks indicate censored data. No statistically significant difference in PFS and OS was observed between the two groups.
In the present study, four patients in the afatinib group and three patients in the osimertinib group had uncommon EGFR mutations. Statistical analysis was not possible owing to the small number of cases; however, a specific therapeutic efficacy was observed (Table II).
Therapy efficacy in patients with NSCLC harboring uncommon EGFR mutations.
Toxicity. All patients reported at least one adverse event (Table III). Frequent adverse events included diarrhea (n=15, 100%), oral mucositis (n=9, 60.0%), paronychia (n=9, 60.0%), rash (n=12, 80.0%) in the afatinib-treated group, and rash (n=21, 61.8%) in the osimertinib-treated group. Four patients (30.8%) receiving afatinib and nine patients (26.5%) receiving osimertinib reported adverse events of grade 3 or more. In total, 12 patients (80.0%) treated with afatinib and 20 patients (58.8%) treated with osimertinib underwent dose reduction due to adverse events, with three patients (20.0%) and two patients (5.9%), respectively, discontinuing treatment owing to adverse events. No treatment-related deaths were observed in either group.
Adverse events experienced by patients in this study.
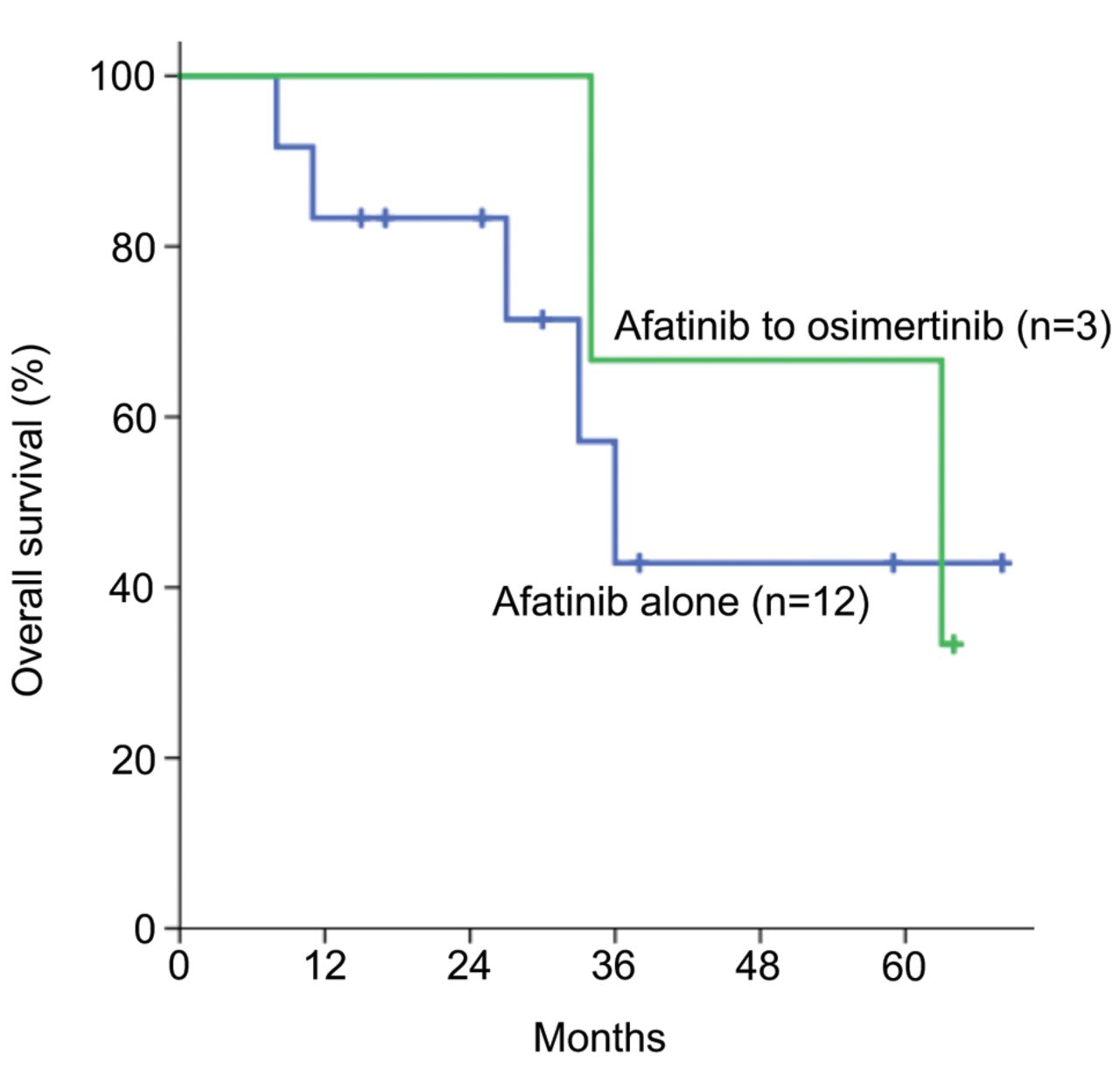
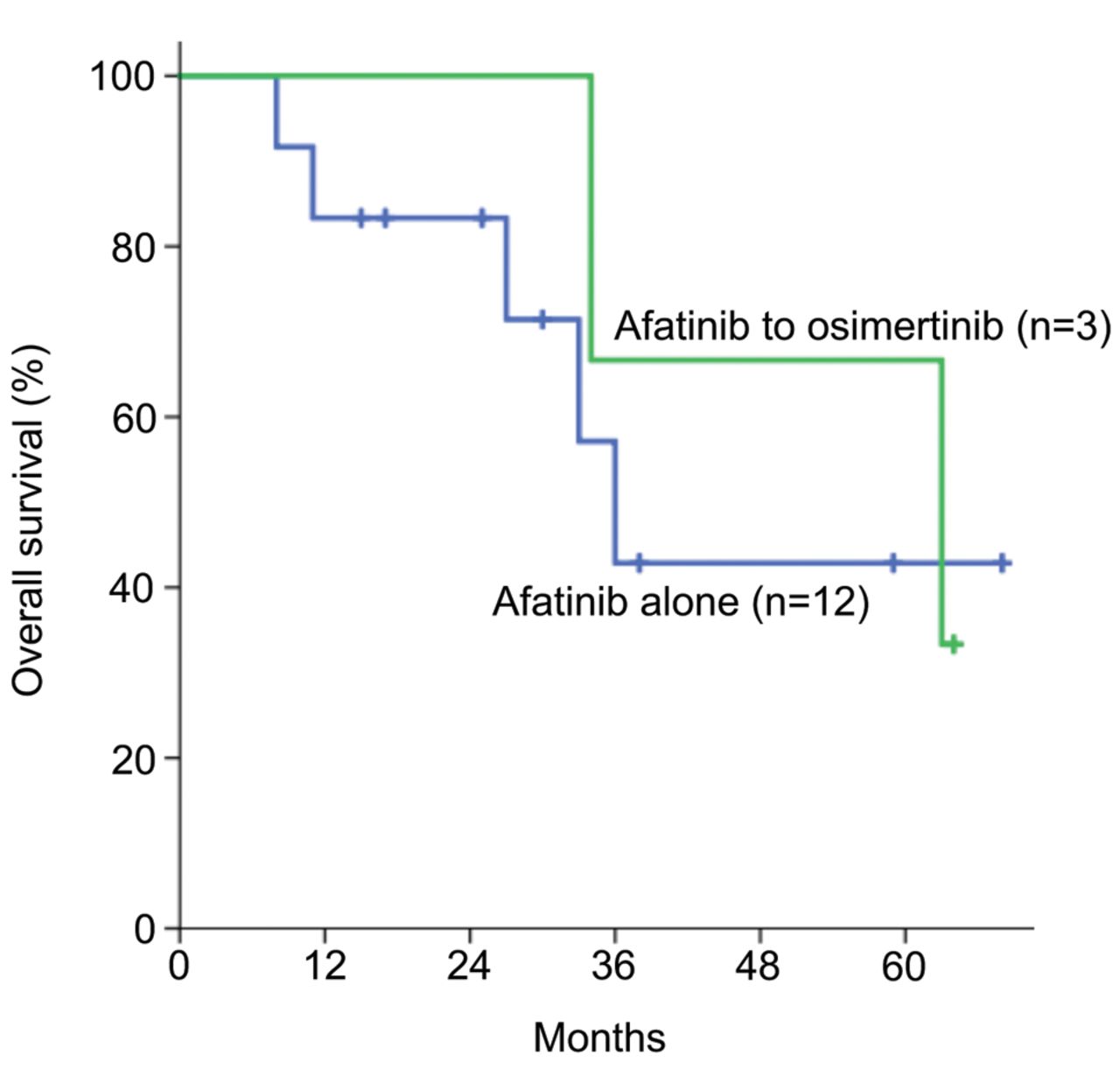
Subsequent treatment. Overall, four out of the 15 patients treated with afatinib continued treatment. Re-biopsy was performed in 10 out of 11 patients who discontinued afatinib treatment, and the T790M mutation was detected in three (two with exon 19 deletion and one with L858R). The samples selected for re-biopsy included three from primary tumor, two from lymph nodes, one from cerebrospinal fluid, one from pericardial fluid, and three from plasma. The T790M mutation was detected in one sample each of primary tumor, lymph node and plasma, and all three patients received osimertinib treatment. The median PFS for these three patients sequentially administered osimertinib was 30 months (range=17-49 months). The median OS for the three patients with the T790M mutation was 63 (95% CI=16.6-109.4) months, whereas for the 12 patients who did not have a T790M mutation, it was 36 (95% CI=28.6-43.4) months (HR=1.454, 95% CI=0.260-8.112, p=0.670) (Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of groups receiving sequential treatment with afatinib followed by osimertinib and those that did not by Kaplan–Meier estimates of the duration of overall survival. Patients who were not known to have died at the time of the analysis were censored at the last recorded date that the patient was known to be alive. Patients who were treated with afatinib and subsequently received osimertinib therapy survived for a prolonged period.
Of the 15 patients treated with afatinib, five received an EGFR-TKI rechallenge after afatinib treatment, and the best outcomes were PR in two, SD in one, and PD in two. Among the 34 patients treated with osimertinib, seven received an EGFR-TKI rechallenge after osimertinib treatment, and the best outcomes were PR in two, SD in three, and PD in two.
Discussion
Both second- and third-generation EGFR-TKIs present the opportunity for superior survival compared to first-generation EGFR-TKIs; however, in the FLAURA trial, superiority in OS of osimertinib over first-generation EGFR-TKIs was not observed in Asian patients. Accordingly, a comparison of second- and third-generation EGFR-TKIs in Asian patients is important. To date, there have been no reports of retrospective and prospective studies on this topic. To our knowledge, this is the first report comparing second- and third-generation EGFR-TKIs.
In the present study, no significant difference was observed between the second- and third-generation EGFR-TKIs in terms of both PFS and OS. Second-generation EGFR-TKIs seemed to be marginally better in terms of response rate, while third-generation EGFR-TKIs appeared to provide better safety.
In this study, we compared second- and third-generation EGFR-TKIs in patients with exon 19 deletion and L858R mutation. The results showed no significant difference in either PFS or OS, even in the analysis of exon 19 deletion and L858R mutation. Several reports have discussed the molecular biological differences between exon 19 deletion and the L858R mutation. With regard to the molecular structure, exon 19 deletion means that EGFR lacks 3-8 bases from the loop of the ATP-binding site, while the L858R mutation is distant from the ATP-binding site (13). In addition, exon 19 deletion can activate downstream signals without requiring dimer formation; however, activation of the L858R mutation requires dimerization (14, 15). Given these molecular biological differences, individual EGFR-TKIs distinctly affect tumors with exon 19 deletion and L858R mutation. A meta-analysis of phase III trials for EGFR-mutated NSCLC revealed that patients with L858R mutation had a significantly shorter PFS than those with exon 19 deletion (16).
In the present study, despite including uncommon mutations, the number of respective cases were small, and statistical analysis could not be performed; however, a specific therapeutic efficacy was observed with both second- and third-generation EGFR-TKIs, with no difference between the two groups. In terms of uncommon mutations, there have been some reports regarding both second- and third-generation EGFR-TKIs, with specific efficacy reported in both cases (17-20).
As EGFR-TKI rechallenge is covered by health insurance in Japan, a rechallenge was attempted in both groups in the present study. Although the number of cases was small and statistical analysis could not be performed, both groups reported some effects, with no differences in the effects of EGFR-TKI rechallenge between groups. Numerous cases of EGFR-TKI rechallenge following resistance to EGFR-TKIs have been reported, with most of the records documenting resistance to first-generation EGFR-TKI (21-26). Although the mechanism of resistance to second-generation EGFR-TKIs has been investigated, few studies have assessed the effects of EGFR-TKI rechallenge following resistance to second-generation EGFR-TKIs (27). Research efforts to determine the resistance mechanism of third-generation EGFR-TKIs are ongoing (28); however, only a few cases of EGFR-TKI rechallenge after resistance to third-generation EGFR-TKIs have been reported (29, 30).
In the present study, the T790M mutation was detected in three out of the 11 patients who had discontinued afatinib treatment and were then administered osimertinib. In the FLAURA trial, T790M mutation was detected in 31% of the 277 who had been assigned to the comparator group, which then progressed from standard treatment to osimertinib therapy (9). In the REMEDY trial, which investigated the status of genetic testing and treatment of NSCLC that progressed during EGFR-TKI treatment, the T790M mutation was detected in only 25.8% of the total cases (31). In the present study, the T790M mutation detection rate was similar to that previously reported. In the cases in which T790M mutation was not detected, the median OS did not differ from that of the entire afatinib-treated group, which was comparable with the median OS of the osimertinib-treated group. Conversely, the median OS of patients with T790M mutation was 63 months, which was an excellent result. The Gio-Tag trial, which evaluated the efficacy of sequential afatinib and osimertinib administration, reported an OS of 41.3 months and found that sequential treatment with afatinib followed by osimertinib administration may prolong OS (32).
This study has several limitations, as it was a retrospective study with a small number of cases. Moreover, the patient backgrounds differed between the two groups (with the osimertinib group being statistically significantly more elderly, and tending to have more cases with poor PS) and long-term follow-up was not performed.
In conclusion, there was no apparent difference in the effect of second- and third-generation EGFR-TKIs but it may be presumed that sequential administration of second- to third-generation EGFR-TKIs may have a benefit in long-term prognosis. Currently, third-generation EGFR-TKIs, which are mildly toxic and prolong PFS, are often used as the first-line treatment. However, given that the effects of second-generation EGFR-TKIs are not inferior to those of third-generation EGFR-TKIs, even if sequential administration is not possible, treatment with second-generation EGFR-TKIs may be deemed the first-line treatment option in anticipation of sequential administration of second- to third-generation EGFR-TKIs. However, it remains unclear which cases can benefit from sequential administration. Head-to-head prospective trials need to be undertaken to provide accurate data, and we hope that further research can clarify factors for selecting suitable patients for sequential treatment with second- to third-generation EGFR-TKIs.
Acknowledgements
We greatly appreciate the patients who participated in this study and thank their families for their cooperation. This work was supported by an OMPU internal research grant.
Footnotes
Authors’ Contributions
Sho Mitsuya: Visualization, investigation, writing original draft. Kenjiro Tsuruoka: Conceptualization, methodology, visualization, writing review & editing. Kiyoe Kanaoka: Validation. Tomoya Funamoto: Validation. Hiroyuki Tsuji: Validation. Ninso Matsunaga: Validation. Takahiko Nakamura: Validation. Yosuke Tamura: Validation. Masafumi Imanishi: Validation. Soichiro Ikeda: Supervision. Yasuhito Fujisaka: Supervision. Isao Goto: Supervision. Akihisa Imagawa: Supervision, funding acquisition.
Conflicts of Interest
The Authors declare no potential conflicts of interest relevant to this study. Dr. Imagawa received a clinical commission/joint research grant from Astra Zeneca for another study.
- Received June 14, 2021.
- Revision received July 31, 2021.
- Accepted August 30, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.