

Abstract
Background/Aim: Expanded indications for patients with preoperatively suspected prostate cancer (PC) undergoing theranostic robotic-assisted laparoscopic radical prostatectomy (T-RARP) are reported. We aimed to build a nomogram of T-RARP to predict final pathologically proven PC. This study reviewed data of 153 patients that underwent T-RARP for suspected PC performed by the same surgeon. Patients and Methods: Patients' preoperative demographic and clinical characteristics included age, prostate-specific antigen (PSA) level, PSA density (PSAD), history of acute urinary retention (AUR), abnormal digital rectal examination (DRE) of the prostate, and Prostate Imaging Reporting and Data System (PI-RADS) classification at 3-T multiparametric magnetic resonance imaging (MRI). Logistic regression with backward elimination was used to select potential risk factors. Results: Based on Harrell's guidelines, we chose seven variables for our final model: Age, DRE corresponding with MRI, AUR, PSAD, prostate-specific antigen velocity (PSAV), PI-RADS, and biopsy pathology. A nomogram for prediction of adenocarcinoma was developed. The original C-index for the nomogram was 0.80 (95% confidence interval=0.74-0.89). The cut-off of the nomogram score for predicting PC was 50 (sensitivity=55.4%; specificity=91.9%). The receiver operating characteristic curve of the model analysis showed an area under the curve of 0.801. Conclusion: A nomogram was produced using age, DRE-corresponding MRI, AUR, PSAD, PSAV, PI-RADS, and biopsy pathology. A preoperative nomogram prediction of prostate adenocarcinoma can help the patient and his family understand the possibility of PC and assist them in their decision-making.
- Laparoscopy
- nomogram
- suspected prostate cancer
- radical prostatectomy
- robotics
The da Vinci robotic surgery system offers a platform for technical improvement and refinements, especially in robotic-assisted radical prostatectomy (RARP) (1). Patients undergoing RARP for prostate cancer (PC) have been shown to have few perioperative complications, rapid functional recovery and lasting long-term oncological control (2, 3). Ten-year actuarial cancer-specific survival rates have reached 98.8% (3). Our robotic team has been mentored by Professor Ashutosh K. Tewari and Professor Vipul R. Patel since 2005. Complication rates decreased significantly to 4% after 600 cases of RARP (4). In a report on 230 patients that underwent RARP with bilateral neurovascular preservation, the continence rate was 98.3% and potency was 86.1% (5). The negative surgical margin rate was 77.0% overall, and in the patient cohort with a low, intermediate, and high risk it was 53.3%, 34.9%, and 11.8% (5). The long-term oncological outcome showed that the 8-year biochemical recurrence-free survival rate among low-risk patients was 95.5% (6). Expanded indications for 55 patients with preoperatively suspicious PC that underwent prophylactic RARP have been reported (7). That study was the first to report that no biopsy-proven PC patients underwent prophylactic RARP with bilateral neurovascular bundle preservation, and that it is safe when performed by experienced surgeons (7). RARP improves urinary function and quality of life postoperatively (7). Prophylactic RARP has been redefined as theranostic robot-assisted radical prostatectomy (T-RARP) because the PC can be both diagnosed and treated using this procedure. The numbers of patients with suspected PC using T-RARP are increasing and a nomogram is needed to predict the incidence of PC preoperatively. Using a nomogram, patients can more easily decide whether to undergo RARP or robotic-assisted simple prostatectomy, or follow-up only. This study aimed to report on the development of a nomogram for the prediction of PC in patients who underwent T-RARP for suspected PC, using 153 cases.
Comparison of preoperative and postoperative pathology in robotic-assisted radical prostatectomy (n=153).
Patients and Methods
We retrospectively reviewed data of a single-surgeon experience with 1,500 patients who underwent RARP at Taichung Veterans General Hospital and Tungs' Taichung Metro Harbor Hospital, Taichung, Taiwan, ROC, between Dec. 2005 and Aug. 2017. Preoperatively, 153 patients with suspicious PC were enrolled in this study. Patients were stratified by final pathology reports of T-RARP specimens into three groups: PC; abnormal [atypical small acinar proliferation (ASAP) or prostate intraepithelial neoplasia (PIN)]; and benign (nodular hyperplasia or inflammation).
The Institutional Review Board of our hospital reviewed and approved the study protocol (IRB number: CE 17196B). We performed the first T-RARP in February 2012. All patients understood RARP complications, and the incidence of urinary incontinence and impotence. Moreover, they were aware that the final pathology after RARP might reveal benign lesions.
Clinical parameters, including age, body mass index (BMI), American Society of Anesthesiologists (ASA) anesthetic/surgical risks class, prostate specific antigen (PSA) levels, prostate volume, PSA density (PSAD), PSA velocity (PSAV), history of acute urinary retention (AUR), pathology of biopsy, abnormal digital-rectal exam (DRE) of prostate, suspicious prostate lesion on 3-T multiparametric magnetic resonance imaging (mpMRI), family history of PC and whether patients were medical personnel, were collected preoperatively. MRI interpretation with Prostate Imaging Reporting and Data System (PI-RADS) classification version 2 was adopted (8). DRE corresponding to MRI as a predictive factor was analyzed with correspondence defined as a prostate nodule of more than 1.5 cm on DRE and MRI showing the prostate lesion with interpretation of a PI-RADS score of 5.
The procedure undertaken for all cases was RARP with neurovascular bundle preservation, as previously described (9, 10). Operative parameters were recorded for each surgery. All specimens were fixed as systematic stepwise sections of the prostate, and were interpreted by a pathologist (10).
All continuous data are expressed as the mean±SD. All statistical calculations were carried out using SPSS 12.0 for Windows (SPSS, Inc., Chicago, IL, USA). Statistical analysis was performed using the Kruskal–Wallis test, Mann–Whitney U-test, chi-squared test and multiple logistic regression, as appropriate. A p-value of less than 0.05 was considered statistically significant. Multiple logistic regression for predictive parameters of PC before RARP was calculated.
Logistic regression with backward elimination was used to select potential risk factors (11). Based on Harrell's guidelines (12, 13) seven variables were chose for our final model: AGE, DRE corresponding with MRI, AUR, PSAD, PSAV, PI RADS, and biopsy pathology. The 95% confidence interval of Harrell's concordance index (C-index) was obtained from 1,000 bootstrap resampling. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) and R (R Core Team 2017).
Results
Table I shows a comparison of preoperative and postoperative pathologies in T-RARP. Eighty-six patients underwent transrectal ultrasound (TRUS)-guided prostate needle biopsy 1-4 times. A final postoperative pathology of adenocarcinoma was found in 34 (39.5%) patients, ASAP or PIN in 34 (39.5%) and a benign lesion in 18 (21%). ASAP or PIN was noted in 13 patients preoperatively, and final pathology revealed adenocarcinoma in seven, ASAP or PIN in five, and benign lesions in one. In 67 cases without prostate biopsy, at the patient's request, the final pathology proved to be adenocarcinoma in 35 (52.2%), ASAP or PIN in 13 (19.4%), and benign lesions in 19 (28.4%). The postoperative results were: PC in 69 (45.1%); abnormal (ASAP or PIN) in 47 (30.7%) and benign in 37 (24.2%).
Preoperative clinical characteristics, operation parameters and complication rate of robotic-assisted radical prostatectomy for suspicious prostate cancer.
With regard to preoperative clinical characteristics of RARP for suspected PC, patient age in the PC group was significantly older than that in the other two groups (p=0.033). Prostate volume was significantly larger in the abnormal and benign groups than in the PC group (p=0.027). The incidence of PSAV>0.75 ng/ml/year was significantly higher (75.5%) in the PC group than in the abnormal and benign groups (36.2% and 48.6%) (p<0.001). The incidence of abnormal DRE was significantly higher (53.6%) in the PC group than in the other groups (29.8% and 29.7%, respectively) (p<0.001). The incidence of PI-RADS score 4-5 by MRI was also higher in the PC group than in the abnormal and benign groups (79.3%, 45.2% and 40%, respectively), and the differences were significant (p<0.001). There was a DRE corresponding to MRI in 10 patients only, and all 10 patients were proven to have prostate adenocarcinoma (Table II).
Operation parameters and complication rates of RARP are shown in Table II. The console time was less than 2 hours and no patients required blood transfusion. The complication rate was 3.9% (6/153), of Clavien–Dindo grade I in five cases: ileus in three, bowel injury with intraoperative repair in one, and bladder injury with intraoperative repair in one case during surgery. On postoperative day 3, a patient suffered from a Clavien–Dindo grade IV complication of myocardia ischemia; he recovered well after medical treatment.
The final pathological characteristics of PC in 69 patients included the following: Tumor volume was ≤1 ml in 23 (33%) patients and <0.5 ml in eight (11.6%). The positive surgical margin rate was 23.1% and angiolymphatic invasion was 8.7%. Clinically nonsignificant PC amounted to 10.1% (seven out of 69 patients) (Table III).
Pathological characteristics of prostate cancer after robotic-assisted radical prostatectomy (n=69).
There were five preoperative predictive parameters that had a mean odds ratio for PC group versus the benign group ranging from 2.73 to 11.21, and a p-value from <0.001 to 0.043. These five factors were PSAD, PSAV, AUR, DRE and MRI PI-RADS score (Table IV).
Figure 1 presents the nomogram for the prediction of PC in patients undergoing T-RARP for suspected PC We provided three examples for calculation of the nomogram score in Table V. The original C-index for the nomogram was 0.80 with 95% confidence interval=0.74-0.89. The average C-index of the 1,000 bootstrap resamples was 0.81. We set a cut-off nomogram score of 50 after calculating the score to be 50.019 at the largest Youden value of 0.4725. The sensitivity was 55.4% and specificity was 91.9%. The receiver operating characteristic curve of the model analysis showed the area under the curve was 0.801 (Figure 2).
Discussion
This study is the first to report a nomogram for the prediction of PC from among 153 patients undergoing T-RARP for suspected PC. The procedures were performed by a single experienced surgeon without surgical bias. A nomogram to predict adenocarcinoma was developed using seven parameters. The cut-off of the nomogram score for predicting PC was 50, with sensitivity of 55.4% and specificity of 91.9%.
This procedure was previously known as prophylactic RARP (7). Now, we have defined it as theranostic RARP, a diagnostic and therapeutic procedure for patients with suspected PC. In this current series, we found that 45.1% of suspected cases actually had PC. We needed to build a nomogram for prediction of patients with PC among those undergoing T-RARP for suspected PC. High specificity is necessary so that RARP is not used in cases with a low probability of PC. For patients with a nomogram score of more than 50, RARP is suggested. Observation/close follow-up or simple prostatectomy is suggested for patients with a nomogram score of less than 50.
In 2004, Brausi et al. reported radical prostatectomy in 25 patients with ASAP (14). All patients were proven to have adenocarcinoma, they therefore concluded that immediate radical prostatectomy is not overtreatment (14). Similarly, radical prostatectomy is sometimes considered in patients with high-grade PIN (15). Transperineal template saturation biopsy was performed every 5-mm in another study. The PC detection rates were 53% (9/17), 89% (8/9), and 83% (10/12) in patients with high-grade PIN and in those who had two or more cores of high-grade PIN or ASAP, respectively (16). In our series, 13 cases of ASAP or PIN were found in the TRUS biopsy preoperatively, and the final pathology at RARP revealed adenocarcinoma in 61.5%, ASAP/PIN in 30.8% and benign disease in 7.7%. Using our nomogram with these 13 cases, a nomogram score >50 was noted in seven of eight patients with PC. One patient with a nomogram score of 30.25 had pT2a PC, with Gleason score 6, and 1% of tumor (volume 1 ml). One of five non-PC patients had a nomogram score of 52.7, and the final pathology was high-grade PIN. Among these 13 cases of ASAP or PIN in the TRUS biopsy, using a nomogram score cutoff of 50, sensitivity was 87.5% and specificity was 80%.
Two important clinical trials for PC screening, the Prostate Cancer Prevention Trial (PCPT) and the European Randomized Study of Screening for Prostate Cancer (ERSPC) (17), use nomograms and risk calculators. Their online risk calculators are used to indicate individual risk of biopsy positivity, and are available(18, 19). Determining the risk of a positive biopsy using the PCPT calculator relies on family history, PSA, DRE, and prior biopsy (20). The ERSPC risk calculator includes age, family history, PSA, DRE, prostate volume and previous negative biopsy, and can estimate individual 4-year PC risk. Their standard diagnosis for PC relies on the TRUS prostate biopsy pathology. Sometimes, the TRUS prostate biopsy may miss a small tumor or prostate tumor in the anterior lobe. For our cohort, we used the final pathology of the T-RARP specimen, since it is more reliable and there is no verification bias.
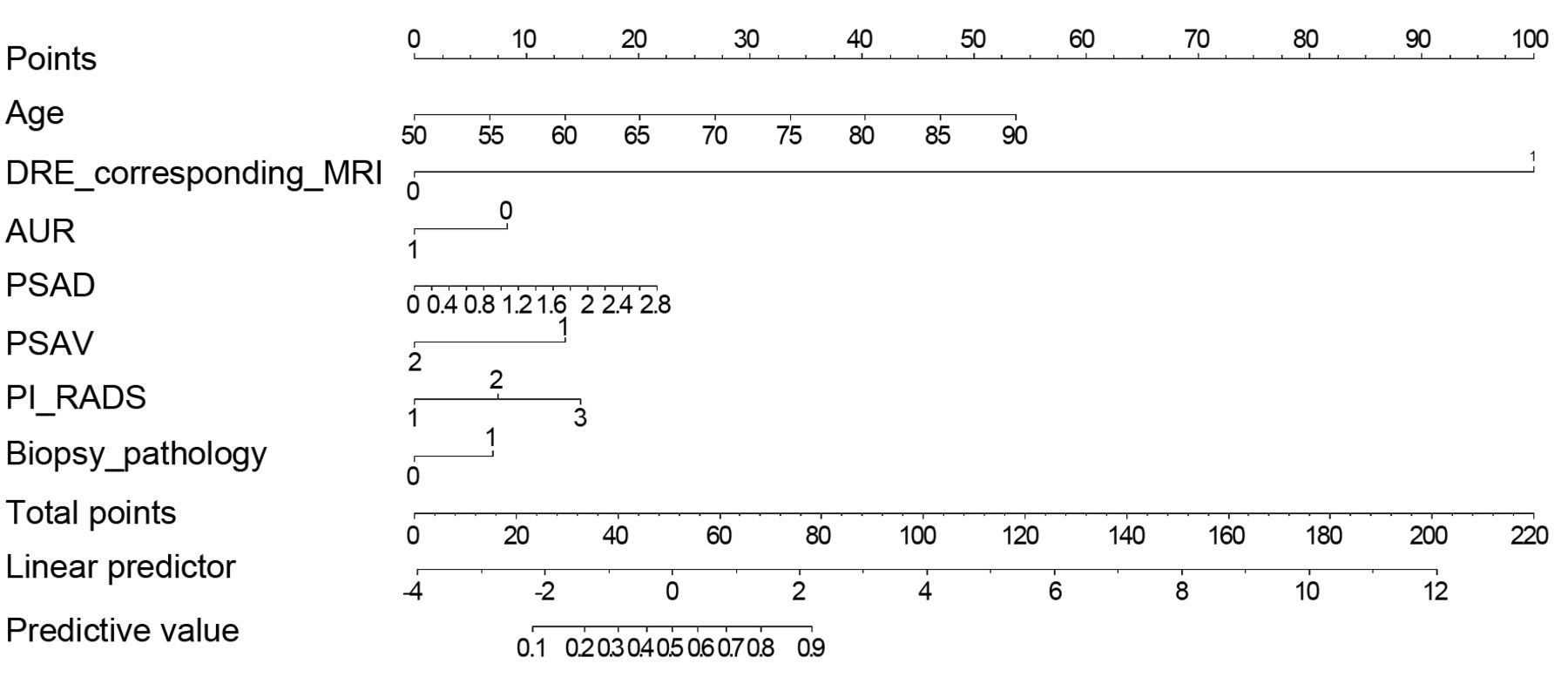
Nomogram predicting prostate cancer among men undergoing theranostic robotic-assisted laparoscopic radical prostatectomy for suspicion of prostate cancer. ASAP: Atypical small acinar proliferation; AUR: acute urinary retention, DRE: digital rectal examination; BMI: body mass index; MRI: magnetic resonance image; PIN: prostate intraepithelial neoplasia; PI-RADS: Prostate Imaging Reporting and Data System; PSA: prostate-specific antigen; PSAD: PSA/prostate volume by trans-rectal sonography; PSAV: PSA velocity.
Parameters predictive of prostate cancer before robotic-assisted radical prostatectomy: Odds ratio for prostate cancer versus benign disease.
Our predictor incorporated PI-RADS scores 4 and 5 on MRI, which would contribute to the risk of PC. A previous study reported that the tumor incidence in a systematic 12-core biopsy adding cognitive fusion-targeted biopsy on mpMRI was 88% and 94% in those with PI-RADS V2.0 scores 4 and 5, respectively (21). In our hospital, we do not perform mpMRI targeted biopsy (22). Furthermore, DRE corresponding to MRI is a definitive predictor of PC. The definition of DRE corresponding to MRI is a firm prostate nodule more than 1.5 cm in size on DRE and MRI showing the prostate lesion with interpretation with a PI-RADS V.2.0 score of 5. In our cohort, all of the 10 cases of DRE corresponding to MRI had PC. The kernel of the DRE was a more than 1.5-cm firm nodule, which was compatible with focally pronounced hypointensity on apparent diffusion coefficient MRI and pronounced hyperintensity on high b-value diffusion weighted imaging MRI, and was ≥1.5 cm in its largest dimension on axial images, which was a PI-RADS V2.0 scores of 5. In 2015, a study reported two cases of radical prostatectomy without prostate biopsy in PI-RADS score 5 lesions on 3T mpMRI, and DRE revealed a prostate nodule (23). They concluded that with a high pre-test probability of PC (rising and elevated PSA, malignant nodule on DRE and a corresponding PIRADS score 5 lesion on mpMRI-P), it may be appropriate to proceed to radical prostatectomy without a prostate biopsy (23). The majority of patients with renal tumor underwent radical nephrectomy or partial nephrectomy as a theranostic procedure without preoperative renal biopsy (24). In the robotic era and with experienced surgeons, preoperative prostate biopsy for patients with highly suspicious PC is a debatable issue.
Three cases as examples for calculation of the nomogram score.
Our clinical study has two unique advantages. Firstly, it reflects real-world practice with patients with highly suspicious PC and a negative prostate biopsy. The use of T-RARP should be reconsidered for patients with DRE corresponding to MRI and biopsy with ASAP/high-grade PIN. If patients have a family history of PC, suffer from lower urinary tract symptoms and experience sepsis after TRUS biopsy, they are likely to be concerned about sepsis and very anxious about suspected PC. Our nomogram is a good tool to help them make an appropriate decision.
Bilateral prophylactic mastectomy is a model of breast cancer risk reduction, especially for breast cancer gene mutation carriers (25, 26). Bilateral prophylactic mastectomy is a major operation with minor risks, and 84% of patients are satisfied with their decision to go ahead with the procedure (27). We agree with the advice from Coelho et al. that the surgeon must provide comprehensive education and counseling to ensure that theranostic surgery is performed under suitable conditions and within the patient's expectations (27). However, the risk of developing PC with gene mutation has not yet been defined. Therefore, our patients were asked to consider their decision after patient group education and discussion across the board.

{kind=link}
{kind=link}
Receiver operating characteristics curve for predicting prostate cancer. The cut-off nomogram score for predicting prostate cancer was 50. Sensitivity was 55.4% and specificity was 91.9%.
RARP performed by a very experienced surgeon and in a high-volume institute can minimize the complication rate to about 3% (4, 28, 29); this is extremely close to a gold standard (1). We suggest that T-RARP performed by experienced surgeons is a reasonable option for patients with suspicion of PC.
RARP for patients with suspected PC is not a new robotic procedure but it is a broadened indication. T-RARP includes its own medico-legal issues, and a second opinion is needed for patients and their family. This is clinical practice among high-volume surgeons and in a few countries. The existence of medico-legal issues is ubiquitous. Even with transurethral resection of the prostate, the mortality rate is 2.5% in Taiwan (30). Perioperative complications and mortality were 6.5% and 0.4% respectively after transurethral resection of the prostate in 4794 cases in the American College of Surgeons National Surgical-Quality Improvement Program database (28). T-RARP can only explain to the patient the probability of PC, not ensure that there is PC. The previous level of sexual function cannot be guaranteed after T-RARP.
T-RARP with bilateral neurovascular bundle preservation is a viable option for suspicion of PC when performed by an experienced surgeon; it is a diagnostic and therapeutic procedure. A nomogram for prediction of PC in patients preoperatively provides the patient and his family the information needed to make a better decision.
Acknowledgements
The Authors wish to thank five mentors for helping to establish the robotic urology program: Hemal AK, Wake Forest University (Winston-Salem, NC, USA); Kawachi MH, City of Hope, National Medical Center (Duarte, CA, USA); Tewari AK and Badani KK, Icahn School of Medicine at Mount Sinai (New York, NY, USA); and Patel VR, Global Robotics Institute, Florida Hospital (Orlando, FL, USA).
Footnotes
Authors' Contributions
YC Ou, MC Tung: Protocol/project development; YC Ou, MC Tung, LH Huang, WC Weng, CY Hsu, YS Lin, TY Tsao: Data collection or management; YC Ou, MC Tung, KH Chang, IJ Tsai: Data analysis; YC Ou, MC Tung: Article writing/editing.
Conflicts of Interest
All Authors state that they have no conflicts of interest.
- Received March 27, 2020.
- Revision received April 10, 2020.
- Accepted April 16, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved