

Abstract
Primary ovarian carcinoids are very rare tumors that belong to the germ cell family of ovarian malignancies. They account for less than 1% of all carcinoid tumors and for less than 0.1% of all ovarian neoplasms. Recurrences are even rarer, with only few cases reported in the literature. Strumal carcinoid has recently been recognized as an extremely rare distinct entity. We report on a patient with bilateral mature cystic teratoma with millimetric foci of ovarian strumal carcinoid who developed lymph node para aortic metastasis after 30 years from primary diagnosis. Our case is thus far the second report of a metastatic strumal carcinoid and the first one in which strumal carcinoid occurred bilaterally and was also metastatic.
- Strumal carcinoid
- ovary
- lymph node metastasis
- neuroendocrine tumor
- primary ovarian carcinoid
- bilateral mature cystic teratoma
- IOTA simple rules
- malignant strumal carcinoid
Case Presentation
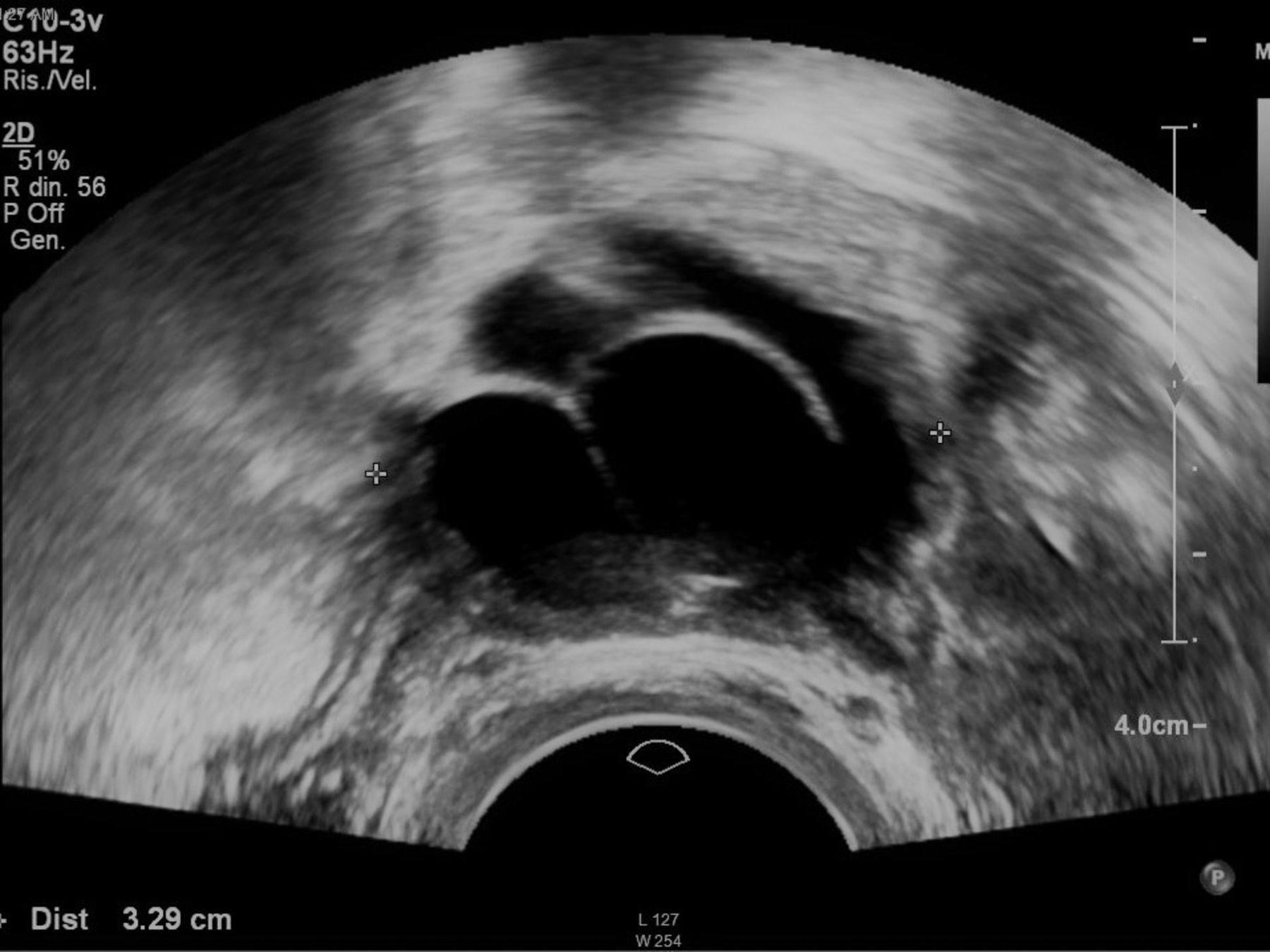
A 61-year-old G1P1 woman (BMI 22 kg/m2) was diagnosed with an incidental right adnexal mass and was then referred to our center. In 1988 she underwent surgery to remove a left ovarian cyst, that was 1-cm mature cystic teratoma with a node of ovarian strumal carcinoid on the definitive pathologic report, contralateral ovary biopsy was normal. In 1995 she underwent left adnexectomy for ipsilateral recurrence of a 3 millimeter struma ovarii. Her past medical history was relevant for cerebral aneurism, arterial hypertension and venous insufficiency. Menopause occurred at 52 and she never used hormone replacement therapy. Her grandmother and aunt were both diagnosed with endometrial cancer. At present she denied any symptoms and pelvic examination was unremarkable. Pelvic ultrasound showed an anechoic right ovarian multilocular (three locules) solid cyst (3.3×3.2×2.4 cm), with scarce vascularization in the septae (color score 2). A single non-vascularized papillary projection of 3.4×7.3 mm was identified. Uterus had regular echotexture with thin endometrial lining. IOTA Adnex Risk Model retrieved a malignancy risk of 19.8% (Figures 1, 2 and 3). Routine investigations were all within normal ranges. Tumor markers (CA125, CA19.9, CEA) and other values were normal (chromogranine A, LDH 211, 5-HIAA, fT3). A CT-scan confirmed the 3.4 cm right adnexal mass, plus two enlarged left para aortic lymph nodes of 2.2 cm each, suspected to be adenopathic. No carcinomatosis nor ascites were described. FDG-PET scan showed focal, moderate metabolic activity in the left para aortic region (SUV max 3.7) only. Laparotomy was planned and we found a 4 cm right ovarian cyst with intact capsule and regular margins and some bulky left para aortic lymph nodes. Peritoneal washing, right oophorectomy and removal of bulky lymph nodes were performed without intra-operative cyst spillage. According to frozen section the cyst was a teratoma with struma ovarii and bulky lymph nodes were metastatic for neuroendocrine tumor. No residual disease was present at the end of surgery. According to the pathology report, ovarian teratoma measured 7×4×3 cm and had a smooth surface and intact capsule. On cut sections, a well-circumscribed, yellowish, solid nodule with mucinous cystic spaces was identified. Ten para-aortic nodes were identified, the bigger was 2 cm in size. Tissue samples were embedded in paraffin blocks, sectioned at 4-μm thickness, and stained with Hematoxylin–Eosin. Microscopically, the nodule contained two cell populations intimately associated: the first consisted of medium size thyroid follicle-like structure with low cuboidal cells, rotund nuclei and central colloid material (struma ovarii), the second (the carcinoid cell component) was made of polygonal cells in a trabecular arrangement, with round nuclei, coarse chromatin in a “salt and pepper” pattern and acidophilic cytoplasm. Fibrous stroma with low mitotic rate and multilocular mucinous cystadenoma cells were present. The tumor was limited to the ovarian parenchyma, without involving the capsule (Figure 4A). In one out of ten lymph nodes massive metastases from neuroendocrine well differentiated tumor were found (Figure 4A). The neuroendocrine tumor cells were immunopositive for synaptophysin (Figure 4B), CD56 and Neuron Specific Enolase and negative for thyroglobulin (Figure 4C) and chromogranin, with focal positivity for CDX2. Ki67 index was <2%. The strumal components were positive for thyroglobulin (Figure 4C). On definitive histological analysis the lesion was monoderm cystic teratoma of the ovary with area of struma ovarii, including focus of well differentiated neuroendocrine tumor, and there was a single lymph node metastasis. Cytology of peritoneal washing was negative. After tumor board we offered the patient a 68Ga-PET about three months after surgery and periodic follow up with tumor markers, ultrasound and CT.

Right ovarian multilocular solid cyst.
Review of the literature
Ovarian carcinoids represent 0,1% of all ovarian neoplasms and strumal carcinoids account for 21.9% (1). Our patient was diagnosed with bilateral mature cystic teratoma with millimetric ovarian strumal carcinoid: as far as we know, all previously reported strumal carcinoids were unilateral. Our case is so far the second of a metastatic strumal carcinoid and the first one in which strumal carcinoid occurred bilaterally and was metastatic. Moreover, strumal carcinoids are almost always benign (2-4) and among the malignant cases in only two of them the neuroendocrine element metastasized: in all other cases, in fact, the metastasizing element was stromal. Armes reported on a pregnant patient with ovarian torsion and metastases of a strumal carcinoid with malignant struma ovarii, but with the thyroid follicular carcinoma component metastasized (5). In our patient the regional recurrence occurred with incredibly long latency, about 30 years after the primary diagnosis, showing low malignancy. In the literature the tumor is often complicated by carcinoid syndrome as a result of bioactive polypeptides produced by the tumor; flushing, diarrhea and bronchoconstriction are often the first signs of the disease. In our patient, however, the diagnosis was incidentally made. The carcinoid element was millimetrical within a much bigger cystic teratoma. What is also remarkable is that the preoperative PET scan showed focal, moderate metabolic activity in the left para aortic region (SUV max 3.7), but the Ki67 index was only <2%: usually strumal carcinoids show metabolic activity only when the proliferative index is high. We intend to analyze the receptor status for octreotide on the tumor and in case of positivity we may consider to use somatostatin analog therapy if disease becomes symptomatic. In conclusion, we think that due to the borderline malignant potential and very slow growth of these tumors a long follow-up is recommended. Due to the rarity of the disease and the lack of precise guidelines there is need for a multidisciplinary diagnostic and therapeutic approach.
Papillary projection.
Primary gynecologic carcinoids are rare tumors that develop from neuroendocrine tissues and are typically well- to moderately differentiated. Ovarian carcinoids account for less than 0,1% of all ovarian neoplasms and are invariably unilateral (1).; they are classified into groups according to histological features: insular, trabecular, strumal and mucinous. Struma ovarii is a rare monodermal ovarian teratoma which contains at least 50% of thyroid tissue: its prevalence among all ovarian tumors is 0.3-1% (6) and 2% among mature cystic teratomas (7). Malignant mature cystic teratoma transformation has been reported in 5-10% of cases, while metastasis can develop in about 5-23% of malignant mature cystic teratomas (8). If the mass is big patients may suffer from abdominal pain or constipation, but strumal carcinoids are sometimes just incidental findings. The median age at diagnosis is 55 and ultrasound is generally the way it is diagnosed: the IOTA group proposed the Assessment of Different NEoplasias in the adneXa (ADNEX) model, the first risk model to differentiate between benign, borderline and invasive ovarian cancer. In a recent study, Van Calster et al. examined the correlation between the final histology (9) and ADNEX Model prediction and in our patient Adnex Model retrieved a malignancy risk of 19.8%, which is higher than the cut-off risk for malignancy (10%). CT and MRI are standard techniques performed to evaluate the extent of the disease. The need to distinguish between primary and metastatic ovarian carcinoid is crucial, since it changes drastically the management and prognosis. Management of carcinoid tumors of the ovary comprises tumor resection with negative margins (most commonly salpingo-oophorectomy, with or without hysterectomy, but there are reports of cystectomy alone (1); fertility sparing surgery may have a role in young patients (10) and octreotide is supposed to be given during surgery to avoid the “carcinoid-crisis” immediately after removing the tumor. There is no evidence for adjuvant therapy of any sort, either hormonal, chemotherapy, or radiation therapy for such tumors (11). Octreotide scan should be considered for somatostatin analog therapy if residual carcinoid tumor or recurrence is present. Octreotide negative tumors or tumors presenting atypical features can be treated with chemotherapy (12). A case of aggressive atypical carcinoid was recently treated with the mTOR inhibitor everolimus (13). The most common sites of metastasis of carcinoid tumors are regional lymph nodes, liver, bones and lung. NCCN panel recommends that patients with recurrent or unresectable carcinoid tumor without carcinoid syndrome should be observed until the disease becomes symptomatic. A case series of 50 strumal carcinoids published in 1980 included only one patient who died of the disease (2). Women who present with stage I have excellent survival, while for more advanced disease the prognosis is poor (14). Blood and urine markers may be helpful for monitoring well differentiated functioning carcinoid tumors. 24 h urinary 5-HIAA is very specific but has low sensitivity, while chromogranin A is very sensitive for patients with diffuse metastases.

Strumal carcinoid: small thyroid follicles with colloid-like material mixed with carcinoid structures (A). Immunohistochemistry showed positive expression of synaptofysin in both carcinoid and strumal components (B) with negative expression of thyroglobulin in the carcinoid area and positive expression in the strumal component (C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lymph node metastasis from a well differentiated neuroendocrine tumor (Hematoxylin and Eosin staining) (A). Immunohistochemistry showed positive expression of synaptofysin (B) and negative expression of thyroglobulin (D). Proliferation index (Ki67) was lower than 2% (C).
Conclusion
To our knowledge, this is the second report of a metastatic strumal carcinoid and the first arising from metachronous bilateral mature cystic teratoma. Strumal carcinoids pose a significant clinical and histological challenge because of the tumor heterogeneity and lack of standardized guidelines for treatment and follow-up. There is a need for multi-disciplinary diagnostic and therapeutic approaches and due to the borderline malignant potential and the very slow growing nature of these tumors recurrences can occur after a long interval and a long follow-up period is required.
Footnotes
Authors' Contributions
Borghese: Protocol/project development, manuscript writing/editing; Razzore: Medical endocrinological management, protocol/project development; Ferrero: Protocol/project development, manuscript writing/editing; Daniele: Histological diagnosis, manuscript writing/editing; Mariani: Diagnostic ultrasound imaging, manuscript writing/editing;Sgro: Protocol/project development; De Rosa: Histological diagnosis, manuscript writing/editing; Biglia: Protocol/project development
Conflicts of Interest
The Authors declare that they have no conflicts of interest regarding this study.
- Received May 24, 2019.
- Revision received June 15, 2019.
- Accepted June 18, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved