

Abstract
Aim: To investigate hyoid bone position and cross-sectional area (CSA) of pharyngeal airway space (PAS) for assessing postoperative airway change after oral cancer surgery with concurrent neck dissection (ND). Patients and Methods: Fifty-two patients who underwent oral cancer surgery with concurrent ND were retrospectively evaluated by grouping based on ND type and reconstruction. Computed tomographic data were analyzed three-dimensionally before and after surgery. Results: The hyoid bone position differed significantly between preoperative and postoperative images in the anteroposterior and supero-inferior directions (p<0.05). CSA was increased after ND (p<0.05). The hyoid bone was positioned more superiorly in ND and fibular free-flap reconstruction groups compared to other groups (p<0.05). CSA of the PAS increased as the hyoid bone moved forward (p<0.05). Conclusion: The hyoid bone moves forward and upward after oral cancer surgery with concurrent ND, which increases the CSA of the PAS. These results provide the useful insight into managing a patient's airway after oral cancer surgery with ND.
- Oral cancer
- pharyngeal airway
- hyoid bone position
- neck dissection
The hyoid bone is essential for various physiological functions, including speech, breathing, and swallowing; therefore, changes in hyoid bone position can affect oral functioning. In addition, it plays a key role in helping maintain patency of the pharyngeal airway space (PAS) (1, 2). Many types of oral and maxillofacial surgery may affect the position of the hyoid bone; however, oral cancer can directly affect the position and movement of the hyoid bone. The typical surgical procedure for oral cancer consists of resection of the primary lesion, neck dissection (ND), and reconstruction. The hyoid bone in patients tends to be displaced after these procedures (3). The change in the position of the hyoid bone after surgery is thought to be the major factor contributing to difficulties in maintaining and stabilizing the PAS (4-6). Therefore, measurement of the position of the hyoid bone after surgery may contribute to the evaluation of airway maintenance related to the quality of life of patients with oral cancer (7, 8).
Most previous studies have used two-dimensional (2D) radiographs; however, these measurements are not always reproducible because they are affected by both head and mandible posture. Changes in the head posture and the inclination of the mandible influence the position of the hyoid bone (9). Careful attention is required in order to successfully reproduce the position of the head to obtain successive radiographs and reproduce hyoid position measurements, which is cumbersome, time-consuming, and difficult (10). Moreover, comparing hyoid bone position changes before and after surgery presents issues with reproducibility.
The development of three-dimensional (3D) imaging and reconstruction with computerized tomography (CT) has enabled the production of more accurate analyses of head and neck anatomical structure. The exact superimposition of the maxillofacial skeleton using an analysis program enables the simultaneous comparison of preoperative and postoperative results. Therefore, CT and 3D reconstructive imaging are now widely used in diagnosis, treatment planning, surgical guidance, evaluation of results, and follow-up studies of various maxillofacial treatments. Nevertheless, to the best of our knowledge, no studies have investigated hyoid bone position and compared postoperative and preoperative hyoid bone position using 3D analysis via superimposition on the cervical vertebrae.
Definition of landmarks.

Reference plane. The sagittal reference plane (SRP) was defined as the plane passing through the odontoid process tip and dividing the body of C2-C3 in half, and passing through the spinous process tip posteriorly. The coronal reference plane (CRP) was defined as the plane perpendicular to the SRP, and passing through the most anterior point of the C2-C3 joint space and the most anterior point of C3-C4 joint space. The horizontal reference plane (HRP) was defined as the plane perpendicular to the SRP and CRP, passing through the most anterior point of the C2-C3 joint.
The aim of the present study was to (i) investigate the position of the hyoid bone and the CSA of the PAS and compare postoperative and preoperative hyoid bone positions; and ii) assess the correlation between hyoid bone position and different surgical modalities after ND in patients with oral cancer using 3D analysis.
Patients and Methods
Study design and participants. This study was a retrospective, case–control study. We included patients with oral cancer who had undergone excision or the main mass and concurrent ND at our affiliated hospital from March 2013 to December 2016. Conventional facial CT was completed immediately before surgery and 6 months postoperatively. patients with congenital or muscular disease or any disease that affects the position of the mandible and spine were excluded. No patients had a history of facial trauma after cancer surgery. The Institutional Review Board of the Kyungpook National University Hospital approved this study, and all patients provided informed consent to data use (KNUH_2019-01-008).
CT image reconstruction. To obtain 3D structural information on the maxillofacial, hyoid, and cervical spine, conventional facial CT images were obtained under the following parameters: Field of view, 19 cm, 120 kVp, and 15 mA, with a continuous slice thickness of 0.4 mm. Facial CT images were converted to Digital Imaging and Communications in Medicine data files as raw data, reconstructed into the multiplanar reformation images, and investigated with reference points on the 3D image analysis software (OnDemand3D; Cybermed, Irvine, CA, USA). The definitions of the landmarks are described in Table I. Postoperative CT data were selected from the follow-up CT scans obtained at least 6 months after the operation.
Superimposition and reference plane. To investigate the hyoid bone position and compare preoperative and postoperative positions, 3D reformatted images were superimposed via setting a volume of interest on the second, third, and fourth cervical vertebrae (C2-C3-C4). In a virtual 3D coordinate system, three reference planes were designated. Firstly, the sagittal reference plane (SRP) was defined as a plane passing the odontoid process tip and dividing the bodies of C2-C3 in half, and passing through spinous process tip posteriorly. Secondly, the coronal reference plane (CRP) was defined as the plane perpendicular to the MSR plane, passing through the most anterior point of the C2-C3 joint space and the most anterior point of the C3-C4 joint space. Thirdly, the horizontal reference plane (HRP) was defined as a plane perpendicular to the SRP and CRP, passing through the most anterior point of the C2-C3 joint (Figure 1).
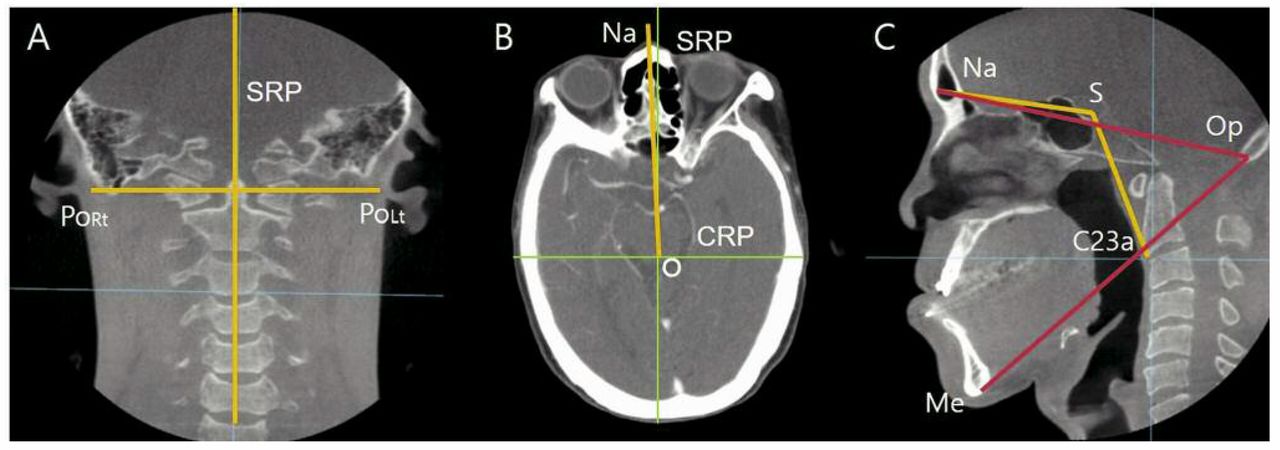
Standardization. A: Head tilting was checked with cranial base angle between the sagittal reference plane (SRP) and the line between the right porion (PoRt) and left porion (PoLt). B: Head rotation was evaluated with the angle between CRP and the line of nasion (Na) to the meeting point of SRP and coronal reference plane (O-point). C: Head flexion (yellow line) was checked with the angle consisting of the Na, sella (S) and the most anterior point of the C2-C3 joint space (C23a). Jaw opening (red line) was checked with the angle of Na and opisthion (Op) and menton (Me).
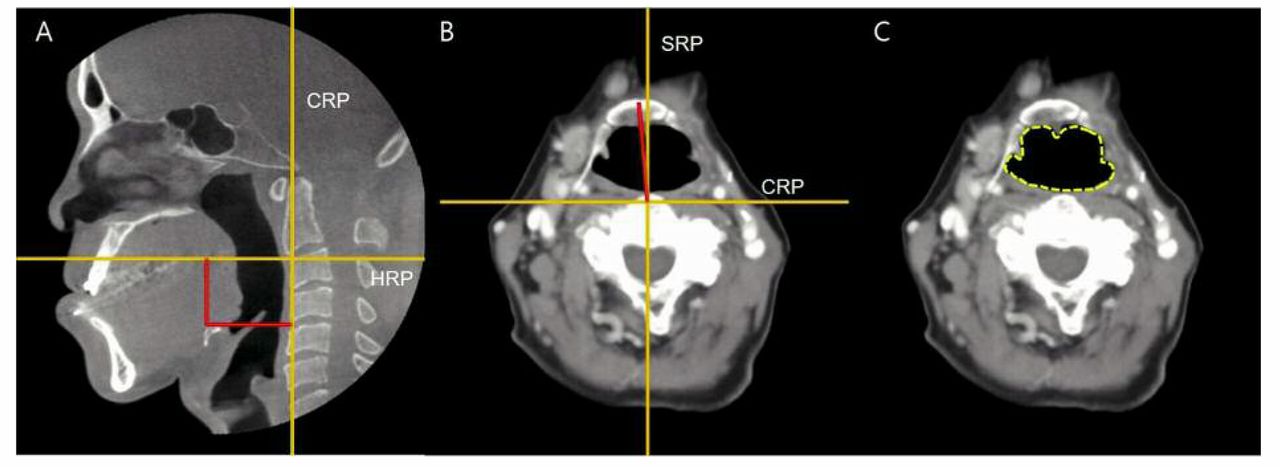
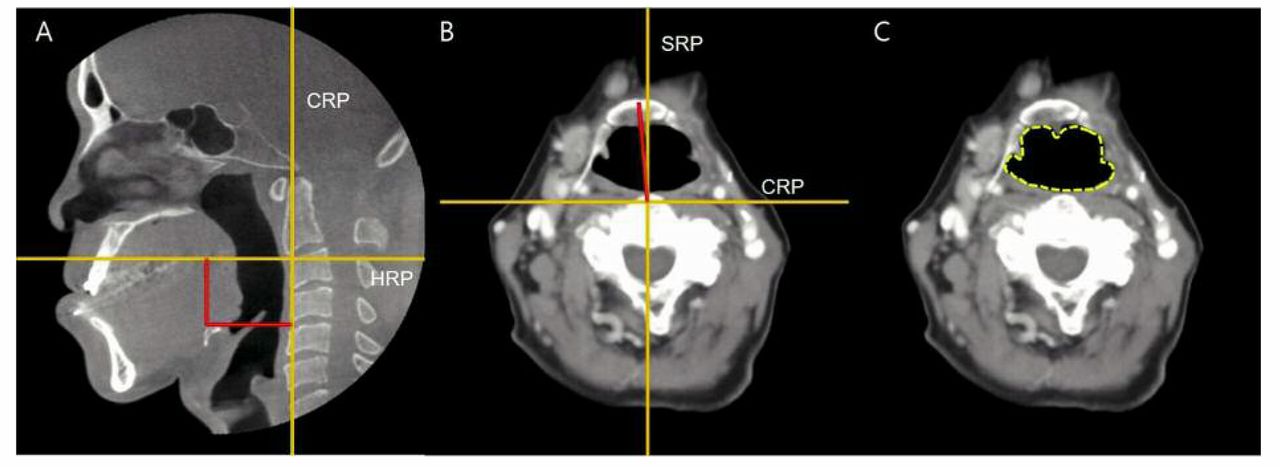
Linear and angular measurement and cross-sectional area. A: linear measurement to evaluate antero-posterior and vertical position of the hyoid bone. B: Angular measurement to evaluate rotation of the hyoid bone. C: Cross-sectional area was checked by the Smart Pen function.
Standardization. To minimize the differences in error due to changes in patient head posturing before and after surgery, head tilting, head rotation, head flexion, and jaw opening (Figure 2) were evaluated. Head tilting was measured using the cranial base angle between the SRP and line between the right and left porion. Head rotation was checked using the angle between the CRP and line of the nasion to the O-point. Head flexion was assessed using the angle that consisted of the nasion, sella and the most anterior point of the C2-C3 joint space (C23a). In order to assess jaw opening, the angles of the nasion, opisthion, and menton were evaluated. Patients who had large changes in their postoperative positions were excluded.
Measurement. Two linear and one angular measurement were used to evaluate the position of the hyoid bone. The perpendicular distance from the HRP to the most anterosuperior point of the hyoid bone in the sagittal plane view was used to measure the anteroposterior position of the hyoid bone. The perpendicular distance from the HRP to the most anterosuperior point of the hyoid bone in the sagittal plane view was used to measure the vertical position of the hyoid bone. Angular measurements were completed using the angle of the most anterior point of the hyoid bone with SRP in the horizontal plane view. The distance and angle were measured using the Cephalometric Analysis Tool in the 3D analysis software. The cross-sectional area (CSA) of the pharyngeal airway at the level of the epiglottis was measured by using the Smart Pen analysis tool in the 3D analysis software (Figure 3).
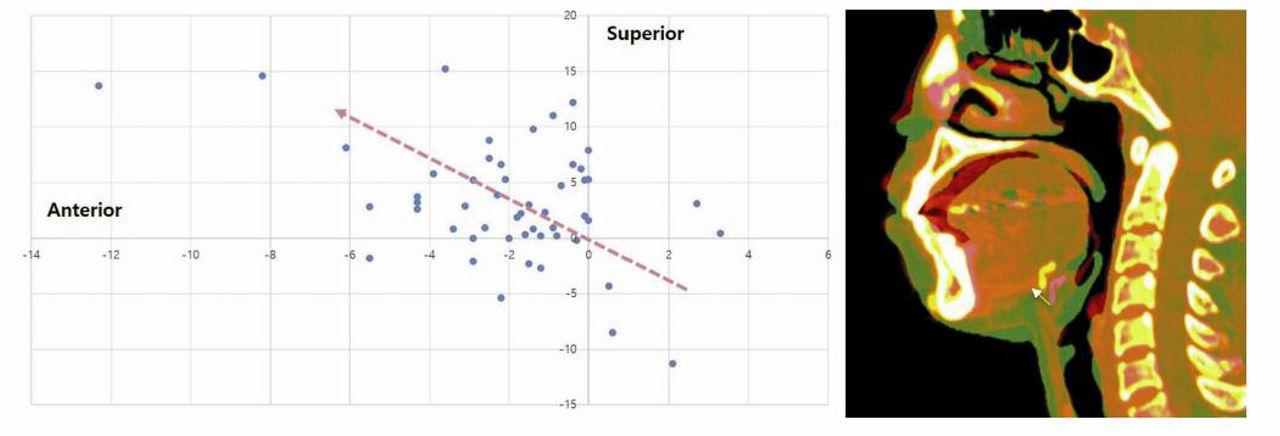
Change in hyoid bone position. The most anterosuperior point of hyoid bone moved significantly anteriorly and superiorly (white arrow) from the original position after oral cancer surgery.

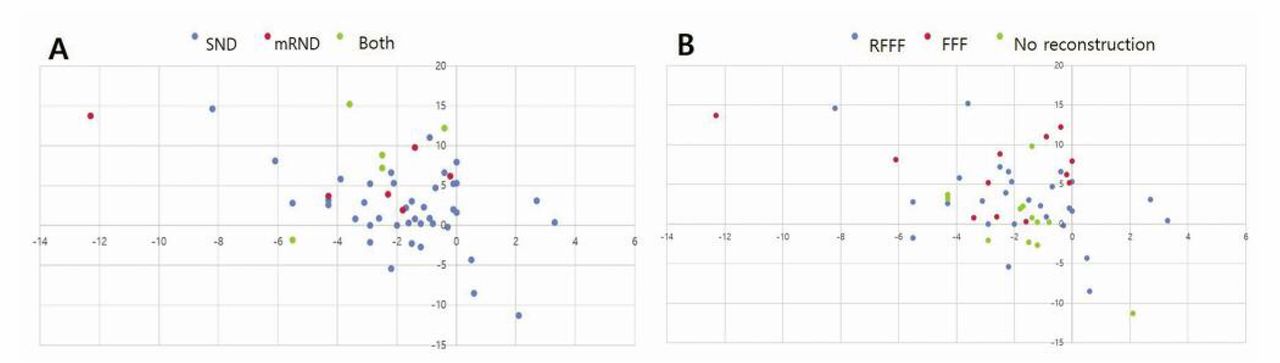
Change in hyoid bone position related to neck dissection type (A) and reconstruction type (B). SND: Selective neck dissection; mRND: modified radical neck dissection; both: both types of neck dissection; FFF: fibular free-flap; RFFF: radial forearm free-flap.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
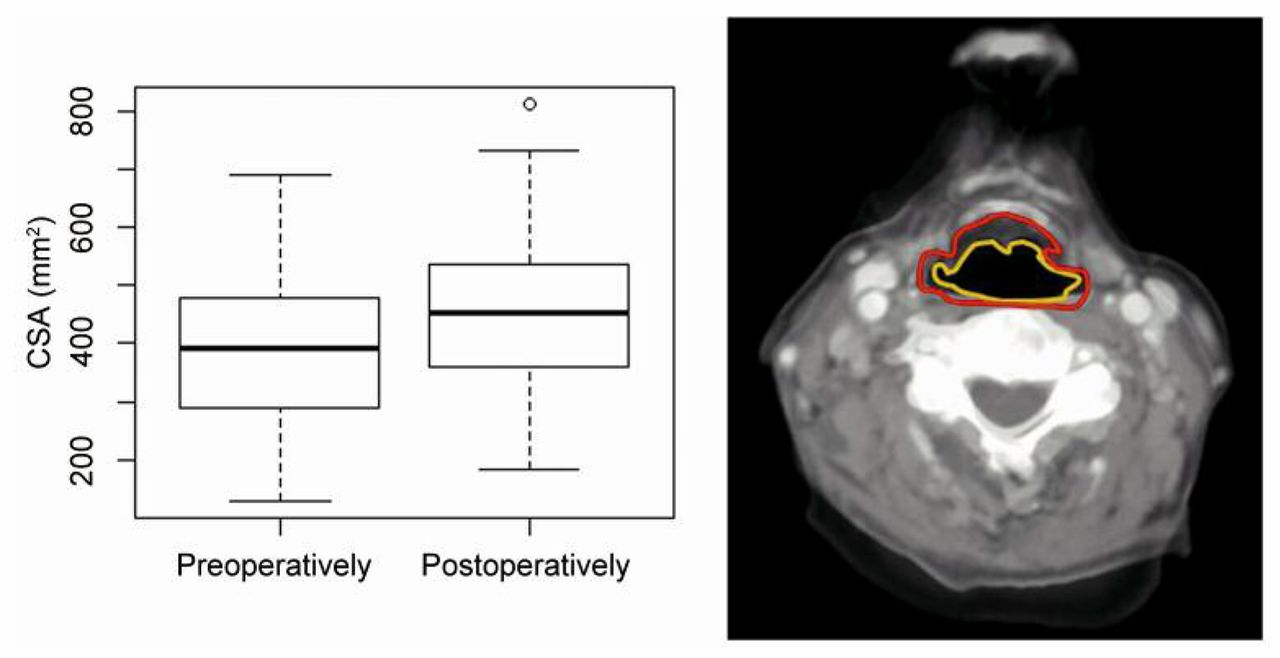
A: Boxplot of the cross-sectional area (CSA) at the level of the epiglottis of the pharyngeal airway pre- and postoperatively (p<0.005). B: Analysis of computed tomographic image. The yellow line indicates the preoperative area, and the red line indicates the postoperative area.
Error measurement. To evaluate measurement errors, the measurements from the original and repeated examination, performed 1 week after obtaining 3D CT images from seven patients, were compared by the same observer (S.T.L.). The error of the method was calculated as Se=√(∑d2/2n), where d was the difference between the double measurements and n the number of paired double measurements (11). The method errors in the linear measurements were 0.43-0.63 mm and were 0.48-0.79° in the angular measurements, which were not statistically significant.
Statistical analyses. The statistical analyzing program R version 3.3.3 (the R Foundation for Statistical Computing) was used to compare data. The paired t-test was used to compare pre-operative and postoperative measurements. Pearson's correlation and Kruskal–Wallis tests were used to analyze differences in hyoid bone position and CSA between factors.
Results
This study included 51 patients (28 male, 23 female) who satisfied the inclusion criteria and standardization. The mean age was 62.5 years (range=42-82 years). Details of the clinical characteristics of the patients are described in Table II.
In selective ND, the lymph nodes at level I, II and III were removed. In modified radical ND, lymph nodes at level I, II, III, IV and V were removed. Both ND procedures consisted of modified radical ND on one side of the primary lesion and selective ND on the opposite side. Fibular free-flap reconstruction was conducted when the main surgery was mandibulectomy.
Comparison of hyoid bone position before and after surgery. The hyoid bone tended to move anteriorly and superiorly after oral cancer surgery with ND (Figure 4). There was a significant difference in anteroposterior (AP) position and vertical position change (Table III). The ND procedure significantly influenced the AP and vertical position change. Furthermore, reconstruction significantly influenced the vertical position change in the hyoid bone (Table IV, Figure 5).
Comparison of CSA before and after oral cancer surgery. The CSA of the PAS at the level of the epiglottis tended to widen after oral cancer surgery (p<0.05) (Figure 6).
Correlations between hyoid bone position and CSA. The CSA of the PAS at the level of epiglottis increased as the hyoid bone moved forward (p<0.05). There was no significant correlation with vertical movement (Table V).
Clinical characteristics of patients. In selective neck dissection, lymph node levels I-III were removed. In modified radical neck dissection, lymph node levels I-V were removed. Both neck dissection consisted of modified radical dissection on the side of primary lesion and selective dissection on the opposite side. Fibular free flap was used when the main surgery was mandibulectomy.
Comparison between pre- and postoperative extent of hyoid bone displacement and cross-sectional area.
Correlations between hyoid bone position and CSA and body mass index (BMI). There was a significant correlation between the AP movement of the hyoid bone and BMI (p<0.05): when the BMI was lower, the hyoid bone moved forward more. There was no significant correlation between vertical movement and CSA (Table VI).
Discussion
Surgeries in the oral and maxillofacial field may affect the hyoid bone directly or indirectly because of its relationship with the surrounding musculature, including the extrapharyngeal, omohyoid, and digastric muscles. Advanced oral cancer typically metastasizes to the cervical lymph nodes. Therefore, oral cancer surgery is often conducted with ND, and requires reconstruction immediately. Inevitably, oral cancer surgery may affect the position of the hyoid bone. Furthermore, one of the major concerns after oral cancer surgery is airway management. Postoperative swelling in the surgical site is the main cause of upper airway obstruction. However, changes in the hyoid bone position can cause upper airway narrowing. Changes in the hyoid bone position induce displacement of the epiglottis, which can then constrict the upper airway (10, 12). Hyoid bone position is significantly correlated with PAS dimensions (13, 14).
Comparison of hyoid bone displacement and cross-sectional area according to different surgical modalities of neck dissection and reconstruction.
Many studies have investigated the correlation between hyoid bone position and CSA of the PAS; however, most used data from orthognathic surgery (8, 10, 13, 14). Therefore, it is difficult to assess the effect of oral cancer surgery on the position of the hyoid bone. In addition, most studies assess dynamic movement impairments of the hyoid bone with swallowing after radiotherapy. However, studies assessing changes in the static position of the hyoid bone after oral cancer surgery are rare (15). There are limitations to these studies; various factors can affect the function of the hyoid bone in oral cancer surgery, but they have not been considered. Therefore, we investigated the changes in hyoid bone positioning and various surgical factors affecting the position of the hyoid bone.
Most studies assessing changes in hyoid bone position in orthognathic surgery used the reference plane in the cranial base or maxilla. However, we set the reference plane on the cervical vertebra, especially C2, C3, and C4, to minimize errors in measurement in the pharyngeal region. The joints of C2-C3 and C3-C4 have a small average flexion-extension range and are more stable compared with other cervical vertebra. The AP and vertical positions of the hyoid bone were related to positions of the head, jaw, and C1-C4. Furthermore, the position of the hyoid in relation to the cervical column exhibits less variability than that to the maxilla and mandible (16, 17). There are various factors that influence the hyoid bone position, such as body height, age, sex, etiology of dysphagia, and bolus characteristics. The recommended measurements for hyoid displacement are currently being investigated with anatomically normalized units (in terms of percentage of the distance between cervical vertebra C2 and C4) that neutralize factor confounding measures in millimeters (18).
Comparison between the change in hyoid bone position and cross-sectional area at the level of the epiglottis.
Comparison between body mass index (BMI) and change in hyoid bone position and cross-sectional area at the level of the epiglottis.
In the present study, we found that the hyoid bone moved anteriorly and superiorly after oral cancer surgery with ND, and the CSA of the PAS increased when the hyoid bone moved forward, as shown in previous studies in orthognathic surgery. However, we analyzed various influencing factors that might change the position of the hyoid bone and correlated these with the CSA of the PAS in patients undergoing oral cancer surgery. We measured the CSA at the level of the epiglottis (the most inferior level of the vallecular) because this level is the most affected by the position of the hyoid bone, and the other sites of the oropharyngeal airway are often altered with the position of the posterior tongue.
Changes were observed in the hyoid bone position and CSA in this study because the soft tissue and areolar tissue surrounding the PAS are enclosed by bony structures, such as the mandible and cervical spine, which might be removed during ND, and postoperative scar contraction would then lead to the contraction of adjacent structures of the hyoid bone (19). Future studies should assess whether the increased CSA leads to changes in the anterosuperior position in the hyoid bone or changes in hyoid bone position lead to increased CSA. We analyzed ND, which was classified into three groups: Selective ND, modified radical ND, and radical ND. We observed changes in hyoid bone position after selective ND and modified radical ND; however, this did not reach significance. The hyoid bone position in the group that underwent radical ND showed more upward movement than did the other groups. These changes may be due to excessive soft-tissue removal from the submental and submandibular space, more than that performed in other types of ND (20, 21).
The type of reconstruction affected the change in vertical position of the hyoid bone after surgery. There are three types of reconstruction: No reconstruction, fibular free-flap, and radial forearm free-flap. Patients who underwent the fibular free-flap showed increased upward movement of the hyoid bone compared with the other reconstruction groups. The site of the primary cancer mass also affected the vertical position change in the hyoid bone after surgery. In cases where the main mass was on the lower gingiva, the hyoid bone tended to move further upward when compared with other groups. Most patients who underwent mandibulectomy, and had a lesion in the lower gingival, underwent fibular free-flap reconstruction. Therefore, they seemed to exhibit similar results.
It is important to consider that when the hyoid bone moves upwards, the PAS becomes shorter. A longer upper airway in patients could be beneficial for preventing airway obstruction by increasing the longitudinal tension of the PAS. However, shortening the PAS increases the chance that the PAS will collapse. Therefore, if there is no structural increase in the airway due to other influencing factors, it may be difficult to manage the airway. More research should consider airway management when moving the hyoid bone upward (22, 23).
The hyoid bone position of patients with a low BMI showed further movement forward than in those with a high BMI. This indicates that patients with a high BMI appear to have a higher fat content in the posterior tongue and anterolateral PAS than those with lower BMI (24, 25). In addition, there was no difference in the CSA of the PAS or movement forward of the hyoid bone between groups with different BMI.
In conclusion, our data revealed that movement of the hyoid bone after oral cancer surgery is associated with different influencing factors, such as type of ND, reconstruction type, primary lesion site, and BMI. The hyoid bone tends to move forward and upward after oral cancer surgery with concurrent ND, which increases the CSA of PAS. We have shown that oral cancer surgery with ND does not adversely affect a patient's airway and have provided data to aid patient airway management.
Acknowledgements
This research was supported by Kyungpook National University Research Fund, 2018.
Footnotes
Authors' Contributions
STL and JYP drafted the article. JYP, JWK and STL carried out operations. STL and JWK contributed to the statistical analysis of the report. STL and JYP critically revised the article. All Authors read and approved the final article.
Conflicts of Interest
The Authors of this article have no conflicts of interest to declare.
- Received February 27, 2019.
- Revision received March 14, 2019.
- Accepted March 20, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved