

Abstract
Background: Patients with adenocarcinoma of the lung are routinely screened for anaplastic lymphoma kinase (ALK) rearrangement because they can be treated by ALK-specific targeted therapy. The clinical and molecular characteristics of large-cell neuroendocrine carcinoma (LCNEC) associated with ALK rearrangement are still unclear. Herein, we assessed the ALK status in a series of patients with LCNEC by testing methods commonly used for adenocarcinoma. Materials and Methods: ALK expression was first examined by immunohistochemistry. For a positively stained tumor, molecular analyses were then conducted. The ALK fusion partner found in a patient with ALK rearrangement was further identified by direct DNA sequencing. Patient clinicopathological features were also analyzed, focusing on the ALK rearrangement-positive case. Results: Immunohistochemistry of seven patients identified strong ALK expression in one case of stage IV LCNEC. Molecular analysis identified a novel rearranged gene resulting from the fusion of kinesin family member 5B (KIF5B) exon 17 to ALK exon 20. The patient was treated with ALK-specific inhibitors, crizotinib and later, alectinib, and has remained alive for more than 24 months without disease progression. Three of the remaining six patients without ALK rearrangement had stage IV cancer and received cytotoxic chemotherapies. Their average overall survival was 5.4 months. Conclusion: To our knowledge, this is the first report of a KIF5B–ALK fusion gene in LCNEC. The patient was successfully treated with ALK inhibitors, suggesting that sensitivity to ALK inhibitor may define a specific LCNEC subtype. We propose that screening for ALK rearrangement in patients with LCNEC may assist in selecting potential candidates for targeted therapy.
- Large-cell neuroendocrine carcinoma
- anaplastic lymphoma kinase
- kinesin family member 5B
- crizotinib
- alectinib
- immunohistochemistry
A large number of gene mutations have been discovered to drive the malignant transformation and cell proliferation of a range of human cancer types, including pulmonary cancer. Screening for these molecular aberrations is a crucial component of cancer therapy, not only for accurate diagnosis, but also for treatment optimization. Anaplastic lymphoma kinase (ALK) gene rearrangement, in which fusion of ALK and a second gene creates a novel driver oncogene, occurs in ~5% of pulmonary carcinomas and is a biomarker for targeted therapy (1-3). In 2011, crizotinib became the first ALK inhibitor to be approved by the United States Food and Drug Administration for the treatment of ALK-rearranged non-small-cell lung cancer (4-6). Since then, several additional ALK inhibitors, including alectinib, have been developed and used as alternative or first-line options for patients with disease resistant to platinum doublet chemotherapy (7, 8). Screening for potential genetic aberrations is now essential for accurate diagnosis of frequently mutated cancers such as lung adenocarcinoma. Molecular testing for ALK gene rearrangement by immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and reverse transcription-polymerase chain reaction (RT-PCR) has been widely used in many facilities to complement morphological analysis and facilitate diagnosis (9-11).
According to the current World Health Organization classification, large-cell neuroendocrine carcinoma (LCNEC) is one of three subtypes of pulmonary tumors that share common neuroendocrine morphological features. The other two are small-cell lung cancer and carcinoid tumors (12). Despite this common classification, clinical and epidemiological features, and molecular profiling vary among the three subtypes, requiring different treatment strategies. Similar to small-cell lung cancer, LCNEC has a poorer prognosis than carcinoid tumors (12, 13). Genomic abnormalities are most frequently observed in LCNEC, followed by carcinoid and small-cell lung cancer (14). Nevertheless, because of their low prevalence, the molecular characteristics and treatment implications of LCNEC are still unclear. Therefore, practical diagnostic and therapeutic approaches need to be developed for this refractory disease. To date, several studies have investigated the ALK rearrangement status of LCNEC (15-17); however, only a few cases have been reported (14, 18, 19), and little is known on the clinical and molecular characteristics of LCNEC with ALK rearrangement. Considering that a number of effective targeted therapies are now available, it is beneficial to identify potential genetic alterations in LCNEC to ensure that patients receive the most appropriate treatments. Herein, we investigated the ALK status and clinicopathological features of a series of seven patients with LCNEC.
Clinical features of the patients of this study.
Materials and Methods
Patients and tumor samples. We investigated seven patients diagnosed with LCNEC at Kindai University Nara Hospital between 2010 and 2016. No patient had received neoadjuvant treatment before their first visit. Histological typing was performed according to the 2015 World Health Organization histological classification (12). The clinical stage was evaluated according to the seventh TNM classification (20). Clinical data were collected from medical records. Survival time was measured from the date of operation or biopsy until the time of death. The study protocol was approved by our Institutional Ethics Committee (approval number 17-14). Informed consent was obtained from all patients.
IHC and FISH. All specimens submitted for histopathological diagnosis were stored as formalin-fixed, paraffin-embedded tissues after surgery. A commercially available intercalated antibody-enhanced polymer method was used for ALK IHC (Nichirei Biosciences Inc., Tokyo, Japan). The percentage of positively stained cells and staining intensity (0 negative, 1+ weak, 2+ moderate, and 3+ strong; relative to positive controls) were recorded according to the manufacturer's protocol. When a neoplastic cell was at least weakly positively stained, it was considered as positive for ALK expression. For ALK-positive tumor, ALK rearrangement was confirmed by interphase FISH with ALK break-apart (2p23) probes (Abbott Molecular, Libertyville, IL, USA), according to the manufacturer's instructions.
Identification of the genomic breakpoint. Total RNA was purified from paraffin-embedded tissue sections using a miRNeasy formalin-fixed paraffin-embedded kit (Qiagen, Hilden, Germany). First-strand cDNA was synthesized from 1 μg total RNA using PrimeScript RT Master Mix (Perfect Real Time) and Ex Taq (TaKaRa, Shiga, Japan). The PCR conditions were 35-45 cycles of 95°C for 30 s and 55-63°C for 30 s. The PCR primers for 5’-ALK fusion partner genes were as follows: Echinoderm microtubule-associated protein-like 4 (EML4): EML4-1F: 5’-TGATGTTTTGAGGCGTCTTG, EML4-6F: 5’-GTCGGCCAATTACCATGTTC, EML4-13F: 5’-CACACCTGGGAAAGGACCTA, EML4-14F: 5’-AAGCTCATGATGGCAGTGTG, EML4-17F: 5’-ACAGTGGTGGCCATAGGAAC, EML4-22R: 5’-TGCTTTGGAGCAGGGATACT; kinesin light chain 1 (KLC1): KLC1-8F5’-CCAGAACCAGGGCAAGTATG; and TRK-fused gene (TFG): TFG-4F: 5’-ACCTGGAGAACCAGGAC CTT; kinesin family member 5B (KIF5B): B-16F: 5’-AGCAGCATG TCAGCTTCGTA; 3’-ALK: ALK-R: 5’-TGCCAGCAAAGCAG TAGTTG.
To verify the fusion point between ALK and the fusion partner, direct cDNA sequencing was performed using an ABI PRISM 3130 genetic analyzer (Applied Biosystems, Foster City, CA, USA).
Results
Patient characteristics. Table I summarizes the clinical features of the studied patients. The median age was 73 years (range=63-84 years), and six out of the seven patients were men. Four patients had stage IV tumor at the initial visit. All tumors were located peripherally. The median tumor size was 33 mm (range=12-100 mm).
All tumors showed typical pathological findings of LCNEC and exhibited a typical staining pattern for at least one of the neuroendocrine markers (chromogranin A, synaptophysin, and CD56). Some high-grade neuroendocrine tumors displayed combined histology of adenocarcinoma, which may have carried genetic changes characteristic of adenocarcinoma (16). In this study, none of the seven samples stained positive for markers of adenocarcinoma, such as thyroid transcription factor 1 (TTF-1) and napsin A. We performed IHC for ALK expression in all samples and detected positive staining in one sample. There were no clear morphological differences between the ALK-positive sample and ALK-negative samples. The serum level of pro-gastrin-releasing peptide was elevated in one ALK-negative case. Neuron-specific enolase was elevated in the other two ALK-negative cases. In the ALK-positive case, these tumor markers were not elevated.

A: Thyroid tumor in the left lobe (yellow arrowhead) and lymph node metastases (red arrowheads) in a neck computed tomographic (CT) scan at initial presentation. B: An ill-defined small nodule was visible in the right lung apex in a chest CT scan. C: The same lesion shown in (B) remained stable on treatment with anaplastic lymphoma kinase inhibitor. D and E: Disappearance of 18F-fluorodeoxyglucose uptake in the vertebral metastasis was achieved after 8 months of crizotinib treatment.
Three patients with ALK-negative stage I or II disease underwent surgical resection as the initial treatment. They all survived for more than 1 year (Table I); the average overall survival of these patients was 37.9 months. The remaining four patients had stage IV LCNEC. Of these patients, the three ALK-negative patients were treated with cytotoxic chemotherapies, but none of them survived for more than a year (average overall survival=5.4 months). The patient with stage IV ALK-positive LCNEC was treated with crizotinib as the first-line therapy. The clinicopathological features of this patient are described in detail in the next section.
Identification of an LCNEC case with KIF5B–ALK gene fusion. A 73-year-old man presented with swelling of the anterior neck. Ultrasound and computed tomography (CT) revealed a thyroid tumor in the left lobe and metastases of the left cervical lymph nodes (Figure 1A) and third thoracic vertebra. A small spiculated nodular lesion was also found in the apex of the right lung (Figure 1B). A smear of a fine-needle aspiration biopsy from the thyroid tumor was submitted as being highly suspicious of malignant thyroid disease. Cytomorphological features of this tumor were classified as the definite malignant category. Its differential diagnosis included metastatic carcinomas from other sites in addition to thyroid follicular cell-and parafollicular cell-derived carcinomas, although serum levels of calcitonin and carcinoembryonic antigen were not elevated. The patient underwent a total thyroidectomy and left neck dissection. Pathological findings showed a trabecular and cribriform pattern without mucin production (Figure 2A). The nuclei were large and contained vesicular chromatin and prominent nucleoli. Immunohistochemical analysis showed positive staining for non-specific neuroendocrine markers such as chromogranin A (Figure 2C) and synaptophysin (Figure 2D), and negative staining for TTF-1 (Figure 2E), thyroglobulin, calcitonin, napsin A (Figure 2F), and p63. The Ki-67 staining index was ~50%. Negative staining for TTF-1 and thyroglobulin ruled out thyroid follicular cell-derived carcinoma and negative staining for calcitonin also ruled out parafollicular cell, or medullary carcinoma. Accordingly, diagnosis of metastatic neuroendocrine carcinoma originating from other anatomical sites was rendered. An additional transbronchial biopsy of the pulmonary lesion revealed a poorly differentiated solid tumor with lobular and palisading patterns and neuroendocrine morphology such as rosette formation and nuclear molding (Figure 2G). Neither mucin production nor keratinization were present. Neoplastic cells in the lung biopsy were positive for chromogranin A (Figure 2I) and synaptophysin (Figure 2J), and negative for TTF-1 (Figure 2K), napsin A (Figure 2L), p40, and p63. Staining of the thyroid and lung biopsy samples for ALK (mouse monoclonal antibody clone 5A4) revealed strong and moderate expression, respectively (Figure 2B and H). The tumor cells contained large intracytoplasmic foci with perinuclear halos. For further molecular analyses, we used thyroid tissue. FISH analysis identified a split signal of ALK. RT-PCR analysis identified a KIF5B–ALK fusion gene, whereas other potential fusion partners, including EML4, KLC1 and TFG, were not detected. The KIF5B–ALK fusion was confirmed by direct sequencing to be an in-frame fusion of the two mRNAs (Figure 3). Mutation of the epidermal growth factor receptor (EGFR) was not detected in the bronchial brushing specimen and extirpated thyroid tumor. We also tested for rearranged c-ros oncogene 1 (ROS1) in the thyroid specimen, but it was not found. Whole-body positron-emission tomography/computed tomography (PET/CT) examination was performed after thyroid surgery. It revealed a known solitary pulmonary nodule and thoracic vertebral metastasis (Figure 1D). However, there was no evidence of distant metastasis in other sites including abdominal, pelvic, and brain regions. The patient was therefore diagnosed with stage IVB LCNEC in the lung with ALK rearrangement.

Analysis of a metastatic thyroid tumor (A-F) and primary lung tumor (G-L) in a patient with large-cell neuroendocrine carcinoma with anaplastic lymphoma kinase (ALK) rearrangement. Sections stained with hematoxylin and eosin (A and G), for ALK (B and H), chromogranin A (C and I), synaptophysin (D and J), thyroid transcription factor 1 (TTF-1) (E and K), and napsin A (F and L), respectively, are shown.

Identification of a novel variant of kinesin family member 5B (KIF5B)–anaplastic lymphoma kinase (ALK). A: Arrow indicates the chromosomal breakpoint. B: Reverse transcription-polymerase chain reaction amplification of the fusion point. A PCR product of 277 bp corresponding to KIF5B–ALK was specifically amplified from tumor cells. MM: DNA size standards (100-bp ladder); P: patient-derived cDNA. C: Schematic representation of the KIF5B–ALK fusion protein. Nucleotide sequencing of the PCR products revealed that exon 17 of KIF5B was fused to exon 20 of ALK.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
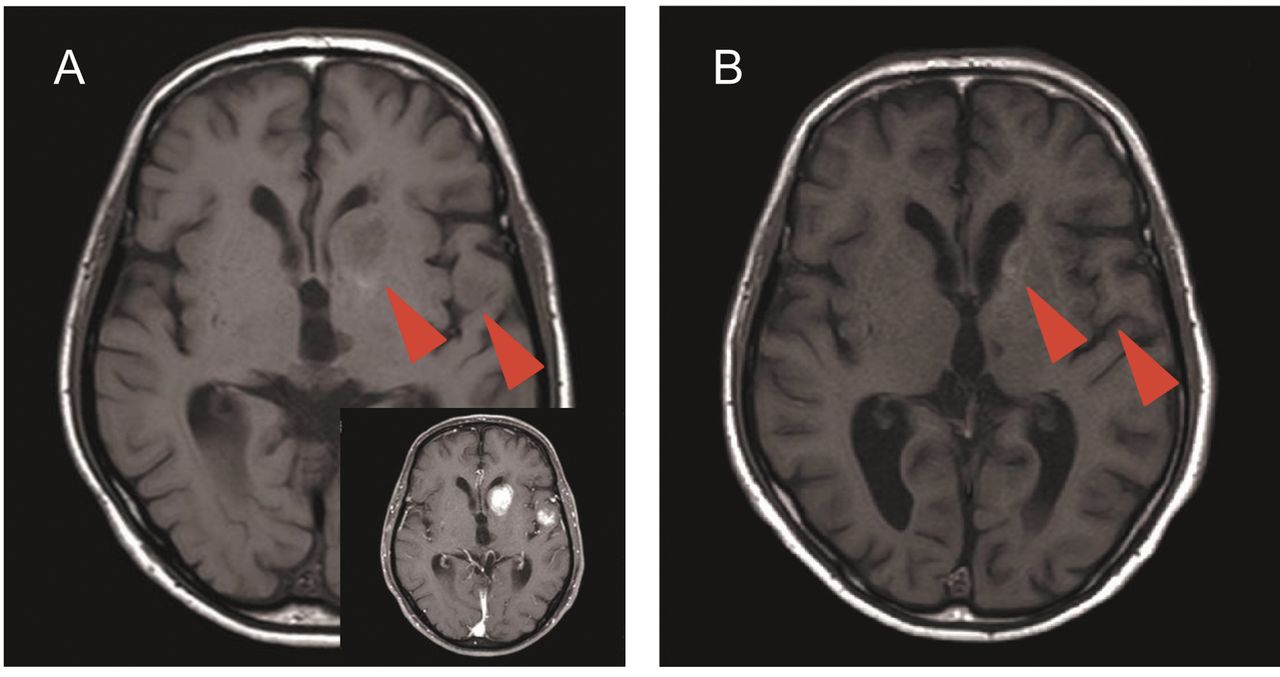
A: T1-Weighted and enhanced brain magnetic resonance imaging at 10 months after cessation of crizotinib showing multiple metastases in the brain. B: A significant decrease in the size of the lesions was achieved after 4 months therapy with alectinib.
The patient was administered crizotinib (250 mg) twice daily. However, 1 week later, he presented with grade 2 nausea according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 (21). Therefore, the drug dose was reduced to 200 mg and a 5-hydroxytryptamine 3 receptor antagonist was administered with crizotinib therapy. Although the symptom was relieved gradually, after 8 months of treatment, signs of nausea reappeared and the patient refused further medication. At this time, no change in the size of the lung tumor was seen in CT and disappearance of 18F-fluorodeoxyglucose uptake (maximum standardized uptake value=5.4) in the vertebral metastasis was obvious in PET/CT (Figure 1E) without any evidence of cervical recurrence or distant metastasis. The patient was carefully monitored without crizotinib and the clinical course was uneventful for 10 months until he presented with gait disturbance. PET/CT and brain magnetic resonance imaging revealed multiple metastases in the brain (Figure 4A). Because it was possible to treat the brain metastases effectively with another ALK inhibitor, alectinib (19, 22), alectinib (300 mg) was administered twice daily. During the follow-up period of 4 months with alectinib treatment, the tumors in the brain were significantly reduced (Figure 4B). The patient has remained alive with stable disease (Figure 1C) according to the Response Evaluation Criteria in Solid Tumors (RECIST) guideline version 1.1 (23).
Discussion
LCNEC is a rare form of lung cancer and its prognosis remains unsatisfactory, especially for advanced-stage disease, as is evident based on the patients described here (24, 25). In contrast to lung adenocarcinoma, there are currently no systematic methods that allow stratification of patients with LCNEC for targeted therapies. Therefore, there is a need for better understanding of the molecular characteristics of LCNEC in order to facilitate optimal therapy selection by oncologists. In this study, we examined ALK expression in seven LCNEC samples. Although the samples were morphologically comparable, only one was identified as being positive for ALK by IHC. The incidence of ALK translocations in LCNEC has not yet been explored to the extent seen with adenocarcinoma. The fact that only a few cases of ALK rearrangement-positive LCNEC have been reported to date (14, 18, 19) suggests that this genetic abnormality may be present in only a minor subset of the disease. Nevertheless, ALK inhibitors may prove to be better therapies for ALK rearrangement-positive lung cancer compared with existing chemotherapy regimens (26, 27). In fact, a very recent study has reported a case of LCNEC with an ALK rearrangement treated by alectinib with a favorable outcome (19). Therefore, we recommend that the ALK rearrangement status should be thoroughly investigated in LCNEC specimens. In this study, we used a sensitive IHC ALK detection method that has shown almost complete concordance with the results obtained with FISH-and PCR-based analyses (16, 28, 29). However, ALK gene rearrangement should still be confirmed at the molecular level because an endogenous full-length ALK protein can also be detected by IHC (16, 30, 31). Our findings are in good agreement with prior studies suggesting that IHC can be used for screening purposes for the routine detection of ALK in LCNEC. We identified KIF5B as a novel ALK partner in the patient with LCNEC studied here. The most frequently detected fusion in ALK rearrangement-positive adenocarcinoma is ALK–EML4, although fusion with other partners, such as KIF5B and TRK, has also been reported (32, 33). The novel gene in our patient resulted from an in-frame fusion between exon 17 of KIF5B and exon 20 of ALK, which is similar to the ALK–KIF5B rearrangement pattern previously identified in pulmonary adenocarcinoma (34).
Another notable finding in this study was that detection of ALK rearrangement was indeed helpful in the management of our patients with LCNEC. Crizotinib is an oral small-molecule tyrosine kinase inhibitor approved for the treatment of ALK-positive non-small-cell lung cancer (5). To date, there has been only one report of ALK rearrangement-positive LCNEC treated with crizotinib, and that patient was found to be resistant to the drug by developing multiple distant metastases after 6 weeks (18). This previous study suggested that ALK rearrangement may not be clinically important in LCNEC, or that neuroendocrine tumors with this genetic alteration may be less responsive to ALK inhibitors than adenocarcinomas. In contrast, considering the aggressive nature of this neoplasm in advanced stages, crizotinib was substantially more favorable as the first-line treatment in our patient. Although data from one patient are insufficient to draw conclusions, we believe that examination of the ALK status will facilitate selection of pulmonary patients with LCNEC who are candidates for ALK inhibitor treatments. More cases will need to be analyzed to determine whether targeted therapy may be a better option than other chemotherapy regimens for these patients.
In conclusion, our IHC and molecular analyses revealed that pulmonary LCNEC is a heterogeneous group of tumors that require a personalized therapeutic approach. Despite the low frequency of ALK rearrangement, further analyses of the molecular characteristics of patients with LCNEC may provide insights into the diagnosis and therapy selection for this refractory tumor.
Acknowledgements
Research reported in this publication was supported by JSPS. KAKENHI Grant Number 16K11190.
Footnotes
Conflicts of Interest
The Authors declare no conflicts of interest.
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from all patients included in this study.
- Received November 4, 2018.
- Revision received November 20, 2018.
- Accepted November 21, 2018.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved