

Abstract
Aim: To evaluate preoperative serum creatinine level as a prognostic parameter in patients with primary epithelial ovarian cancer (EOC). Patients and Methods: In a retrospective cohort study, serum levels of creatinine were evaluated in 498 patients with EOC. Data were extracted from our prospectively maintained database. Results were correlated with clinicopathological parameters and patient survival. Results: The mean pre-therapeutic serum creatinine level in patients with EOC was 0.84±0.40 mg/dI. A serum creatinine level of 1.2 mg/dl or higher was found in 22 (4.4%) patients and associated with poor survival. In a multivariate logistic regression analysis, the serum creatinine level was a significant independent prognostic parameter of overall survival. Conclusion: The preoperative serum level of creatinine may be useful as an additional independent prognostic parameter in patients with EOC.
- Ovarian cancer
- creatinine
- prognosis
Recently, a published study reported preoperative hyponatremia, elevated serum creatinine level, hypoalbuminemia, and thrombocytosis to be associated with perioperative morbidity in patients with epithelial ovarian cancer (EOC) (1). Various studies have also shown a significant prognostic influence of serum albumin level (2) and thrombocyte counts (3), while as far as we are aware of, no data are available on patients with EOC regarding elevated serum creatinine level.
Impaired renal function at diagnosis of a malignant disease has been linked to increased postoperative morbidity and worsened survival (4). Serum creatinine has been investigated as a prognostic parameter in colorectal (5), upper urinary tract/urothelial (6), and prostate (7) cancer, as well as liposarcoma (4) and multiple myeloma (8). It can be hypothesized that an elevated serum creatinine level is indicative of impaired kidney function, reflecting frailty or a poor performance status. These conditions can lead to greater reluctance of treating physicians to plan major surgery, to reduced tolerability of an individual patient of cytoreductive surgery, and a higher probability of discontinuation or the necessity for a reduced dose of chemotherapy. An elevated serum creatinine level can therefore be seen only as surrogate marker for a patient's reduced physical status. Whether or not the serum creatinine level influences a patient's course of disease has not been resolved.
The aim of the present study was to investigate whether an elevated serum creatinine level can serve as an additional, cheap, and readily available prognostic parameter reflecting overall survival in patients with EOC.
Patients and Methods
Patients. A total of 498 patients with EOC were included in the present retrospective cohort study. All patients were treated between 2000 and 2015 at the Department of General Gynecology and Gynecologic Oncology, Medical University of Vienna, Austria. The Institutional Review Board of the Medical University of Vienna approved the present study (IRB approval number: 247/2009). Individual patient data were extracted from our database. At the time of EOC diagnosis, a physical examination was performed as were routine blood tests, including the serum level of creatinine. Patients were treated according to local standards with cytoreductive surgery and adjuvant platinum-based chemotherapy with/without bevacizumab. Surgical staging was performed according to International Federation of Gynecologists and Obstetricians (FIGO) guidelines (9), including hysterectomy, bilateral salpingo-oophorectomy, pelvic/para-aortic lymphadenectomy, appendectomy, omentectomy and additional cytoreductive procedures to resect all gross tumor. All patients with FIGO tumor stages IC to IV and all patients with clear-cell carcinoma received an adjuvant platinum-based chemotherapy. Post-therapeutically, all patients were followed-up four times annually, including pelvic examination, abdominal ultrasound examination, and serum evaluation of cancer antigen 125 (CA-125) for the first 3 years, afterwards twice yearly for 2 years, and thereafter once annually for further 5 years.
As part of our Institutional clinical routine, blood samples were obtained by peripheral venous puncture 24 to 72 h prior to surgery. Serum creatinine was measured using the Creatinine Jaffé Gen. 2 test (COBAS CREJ2; Roche Diagnostics, Indianapolis, IN, USA). Serum creatinine concentrations between 0.50-1.2 mg/dl were considered normal.
Statistical analysis. Values are given as the means with standard deviation (SD). Variables were compared using the Pearson's correlation coefficient, t-test, and one-way ANOVA, where appropriate. Survival probabilities were calculated by the product-limit method of Kaplan and Meier. Differences between groups were tested using the log-rank test. Univariate and multivariate Cox regression models for overall survival were performed including tumor stage (FIGO I vs. II vs. III vs. IV), presence of postoperative residual tumor mass (present vs. absent), histological grade (G1 vs. G2 vs. G3), histological type (serous vs. all other), age, and serum creatinine level. The results were analyzed for the endpoint of overall survival. Only cancer-related death was regarded as an event, patients who died due to other reasons or were alive even with tumor present at the time of last follow-up were censored at the date of last follow-up. Survival times of disease-free patients or those still alive, or dead as a result of other causes, were censored at the last follow-up date. A multivariate model was used with all established clinical prognostic parameters and serum creatinine as a dichotomous variable (< vs. ≥1.2 mg/dl). The value of 1.2 mg/dl was used as a cut-off since serum creatinine levels over 1.2 mg/dl are defined as being pathological. p-Values of less than 0.05 were considered statistically significant. Hazard ratios (HR) and 95% confidence intervals (CI) are provided. For statistical analysis, the Statistical Package for the Social Sciences statistical software was used (SPSS 22.0 IBMCorp., Armonk, NY, USA).
Results
Patient characteristics are shown in Table I. Overall, the mean pre-therapeutic serum creatinine level in patients with EOC was 0.84±0.4 mg/dl. Serum creatinine (≥1.2 mg/dl) was elevated in 22 (4.4%) patients. The association between investigated serum parameters and clinicopathological parameters are shown in Table II. Elevated serum creatinine levels were associated only with patient age (r=0.2, p<0.001).
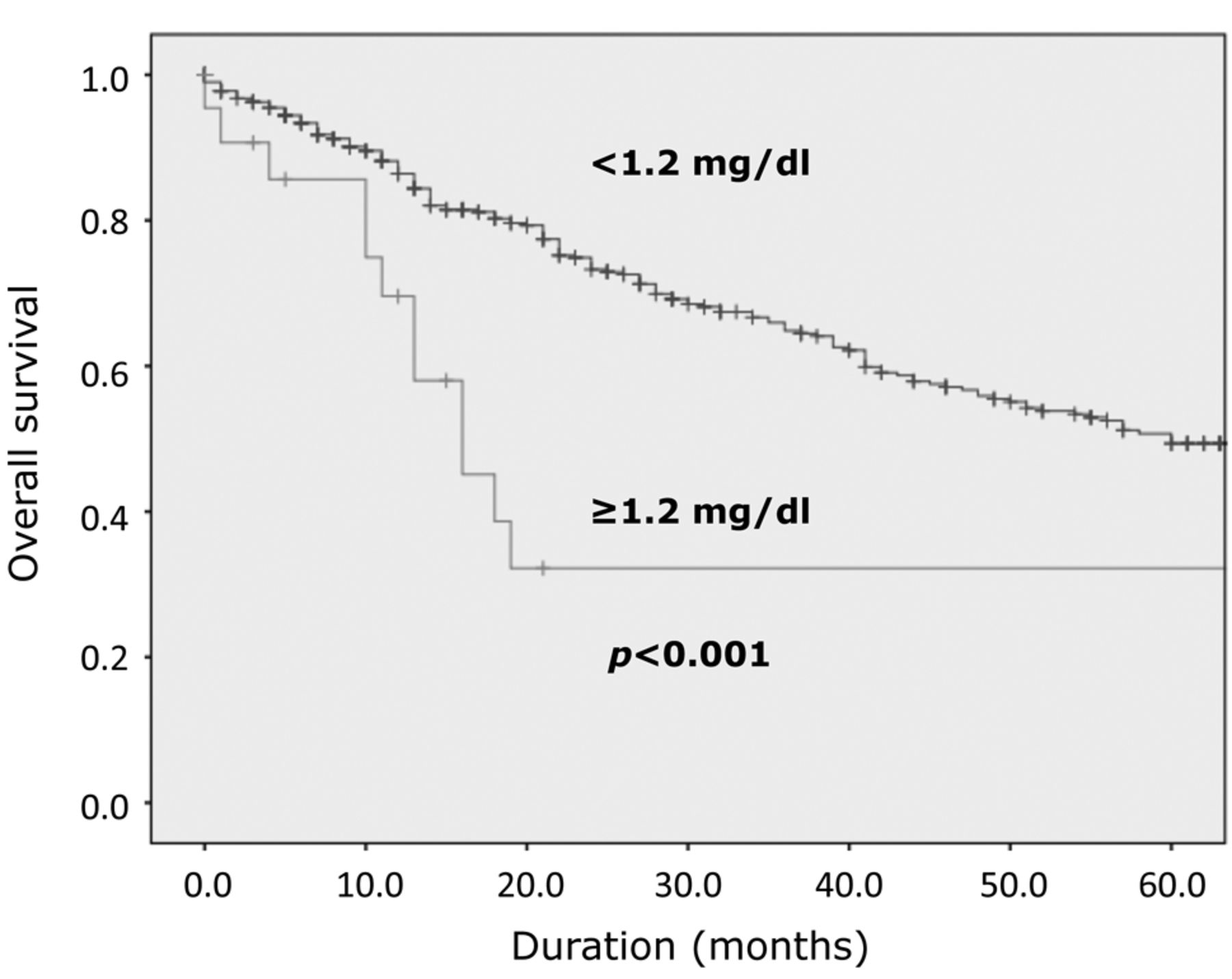
In the univariate analysis, serum creatinine was considered both as a continuous variable and separately as a dichotomous variable using the cut-off of 1.2 mg/dl. Serum creatinine reached statistical significance as both continuous and dichotomous variable, as did all establish clinical prognostic parameters (Table III). Figure 1 shows the overall survival of patients dependent on serum creatinine level using a cut-off of 1.2 mg/dI. In the multivariate analysis, serum creatinine remained significantly and independently negatively associated with overall survival as both a continuous and dichotomous variable. A higher serum creatinine level was predictive of a significantly impaired prognosis.
Study patient characteristics.
Patient characteristics and correlation with the evaluated parameters of the study group.
Discussion
In the present study, a high serum creatinine level was associated with impaired overall survival in patients with EOC. A number of laboratory parameters have been shown to be associated with impaired prognosis in patients with EOC including markers of inflammation, serum tumor markers, thrombocytosis, serum level of angiotensin-converting enzyme and cell-surface markers expressed by the tumor cells (10-14). Interestingly, recently published studies investigated whether medical interventions such as antihypertensive medication or parenteral nutrition influence the prognosis of patients with cancer by altering circulating inflammatory markers or serum albumin levels (15, 16). Our study is in line with the aforementioned data, as the independent prognostic factor ascertained in our study, namely the serum level of creatinine, can be changed by medical interventions. Therefore, this could serve as a potential target in future clinical trials aimed to normalize the preoperative level of creatinine in order to beneficially affect patient prognosis.
Univariate and multivariate overall survival analysis in 498 patients with epithelial ovarian cancer.
Comparable to assessing red blood cell counts, investigating preoperative renal function seems valuable in planning surgery and estimating the patient's risk of postoperative complications. To date, guidelines acknowledge treating that tumor-associated anemia can reduce complications and possibly improve overall survival (17, 18). Based on previously published data and on the results of the present study, it can be hypothesized that it may be clinically useful to assess renal function at the time of EOC diagnosis and eventually improve renal function in the preoperative setting. In the present study, serum creatinine was prognostically relevant when used as a continuous variable, with a cut-off value of 1.2 mg/dl. Thus, we encourage others to use this cut-off value when using serum creatinine as a tool for preoperative optimization of patients with EOC.
Due to the availability of new targeted therapies and its implication for family members, recommendations for genetic testing regarding breast cancer 1 and 2 genes (BRCA1/2) were issued recently (19). Due to the retrospective design of our study, we included patients that were diagnosed with EOC between 2000 and 2015. Therefore, data regarding BRCA mutation was lacking in many of the cases. Another interesting hypothesis, which has to be kept in mind when interpreting the results of our study, is the fact that a high serum creatinine level is associated with renal impairment in general. As patients included in the present study were treated with chemotherapy, it can be hypothesized that the observed worse prognosis might be due to the malignancy of the cancer itself or due to the intolerance to chemotherapy that might lead to renal failure. As we have no data available regarding side-effects of chemotherapy regimens, we cannot support one or the other assumption.

{kind=link}
Kaplan–Meier analysis of overall survival of patients with ovarian cancer dependent on serum creatinine level using a cut-off of 1.2 mg/dI.
In summary, our study showed that the serum level of creatinine is an independent prognostic parameter of overall survival among patients with primary EOC. Our data support the need for preoperative assessment of creatinine. This is of particular interest as this factor could be corrected preoperatively. The prognostic value of preoperative correction of high creatinine level should be tested in further clinical studies.
Footnotes
Conflicts of Interest
None of the Authors have any actual or potential conflict of interest including any financial, personal or other relationships with other people or organizations that could inappropriately influence, or be perceived to influence, their work to disclose.
- Received June 25, 2018.
- Revision received July 15, 2018.
- Accepted July 19, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved