

Abstract
Background/Aim: To investigate whether neutrophil–to–lymphocyte ratio (NLR) might represent an additional biological criterion able to identify patients with worse prognosis within the 8th edition TNM prognostic staging system for breast cancer (BC). Patients and Methods. Pre-treatment NLR was retrospectively analyzed in 475 BC women prospectively followed for a mean time of 3.8 years. The optimal NLR cutoff, identified by ROC analysis, was set at 2. Results: Elevated pre-treatment NLR was associated with worse disease-free survival (DFS) (HR=2.28) and overall survival (OS) (HR=3.39). The prognostic value of NLR was mostly evident in stage I BC (HR for DFS=2.89; HR for OS=1.30), in whom NLR significantly stratified patients who developed distant metastasis (HR= 4.62), but not local recurrence. Conclusion: NLR might provide important information in risk stratification, especially in stage I BC patients in whom the presence of a high NLR might raise the question as to whether they should be more aggressively managed.
- Breast cancer
- prognostic staging
- neutrophil–to–lymphocyte ratio
- progression-free survival
- overall survival
Neutrophils are widely recognized to play fundamental roles at each step of tumorigenesis – from initiation to primary tumor growth and metastasis – owing to their susceptibility to phenotypic changes induced by the tumor microenvironment and being themselves capable of altering the behavior of other cancer-associated immune cells (1, 2). Accordingly, the neutrophil–to–lymphocyte ratio (NLR) – integrating the detrimental effects of neutrophilia and lymphopenia – has been proposed as an easy-to-use and cost effective prognostic biomarker in various cancer types (3), including breast cancer (BC) (4-7).
In the past three years, we have witnessed a rapid growth in the number of studies investigating the association of a high NLR with disease-free (DFS) and overall survival (OS) of BC patients (8-20). The most significant were comprehensively analyzed in recent meta-analyses, which emphasized an association between high NLR and an adverse BC outcome, both in early and recurrent stages (6, 7), with a greater effect on disease-specific outcome in estrogen receptor (ER)- and HER2-negative disease in the study by Ethier et al. (6) and a stronger association in triple-negative BC (TNBC) in that by Liu et al. (7). On the other hand, no subgroup showed an influence on the association between NLR and OS (6).
From these data, it emerges that the prognostic significance of NLR could be predominant in TNBC (14, 16-19), but TNBC sample size in these studies was usually small. More recently, Wariss et al. reported an association between high NLR and adverse OS in more than 2000 BC women, but only in the luminal subtype (21), a finding that is in agreement with preliminary studies suggesting the independent prognostic value of NLR in luminal A BC (22, 23). Thus, the issue of an association between NLR and prognostic features is still unresolved.
In January 2018, the American Joint Commission of Cancer (AJCC) has issued the 8th edition TNM staging system for BC, in which the use of non-anatomic prognostic factors (i.e., grade, hormone receptor expression, and HER2 amplification) has been expanded in assigning prognostic stage groups to complement the anatomic TNM staging system (24). Predictably, patients' stratification according to the prognostic TNM yielded a survival rate classification superior to that achieved using the anatomic stage (25).
Based on the above and being aware of the contradictory results previously reported (13, 20, 26), the present study was designed to investigate the prognostic value of NLR in a cohort of prospectively enrolled BC patients re-staged according to the prognostic TNM, with the aim to evaluate whether NLR might represent an additional biological criterion able to discriminate patients with worse prognosis within the new BC staging system.
Patients and Methods
Starting from January 2007, the PTV Bio.Ca.Re. (Policlinico Tor Vergata Biospecimen Cancer Repository) and the Interinstitutional Multidisciplinary Biobank of the IRCCS San Raffaele Pisana (SR-BioBIM, Rome, Italy) are actively involved in the recruitment of ambulatory patients with primary or metastatic cancer, who are prospectively followed under the appropriate Institutional ethics approval, as part of a Clinical Database and Biobank project. Among these, a cohort of 475 consecutive BC patients in whom prognostic biomarker factors and pre-treatment differential blood cell counts were available was selected for this study. Inclusion criteria were: age above 18 years, an Eastern Cooperative Oncology Group (ECOG) performance status ≤2 and adequate hematological, hepatic and renal functions. Concurrent infectious, inflammatory or autoimmune diseases were all considered as exclusion criteria for the current analysis.
Breast surgery was performed in all 475 women (26.7% mastectomy, 73.3% conservative surgery followed by standard radiation therapy). Among them, 67 (14.1%) and 392 (82.5%) women received neoadjuvant and adjuvant therapies, respectively. Adjuvant chemotherapies, both anthracycline and non-anthracycline containing, were instituted in 142 (36.2%) and 117 (29.9%) patients with and without lymph node involvement, respectively. Among women with node-negative disease, 125 (39%) underwent adjuvant endocrine therapy only (tamoxifen or aromatase inhibitor). Patients with HER2/neu positivity were all treated with trastuzumab-containing regimens. First-line chemotherapy was instituted in 16 patients with stage IV BC. All patients were prospectively followed for a mean time of 3.8 years.
The study was performed in accordance with the principles embodied in the Declaration of Helsinki. All patients gave written informed consent, previously approved by our Institutional Ethics Committees.
Blood sampling and assessment of NLR. Fasting serum samples were obtained prior to any treatment from each recruited patient. Routine hematology studies were immediately performed on fresh blood, then samples were aliquoted and stored at −80°C in the facilities of the PTV Bio.Ca.Re. or the SR-BioBIM.
Complete and differential blood cell counts were assessed on EDTA anti-coagulated whole blood using a Coulter LH750 hematology analyzer (Beckman Coulter, Miami, FL, USA). NLR was calculated as the ratio of the neutrophils to lymphocytes absolute counts obtained from the same blood sample taken at baseline. All measurements were ascertained while blinded to the sample origin and to study endpoint.
Assessment of prognostic indexes. Grading was assessed according to the Nottingham grading system (Elston-Ellis modification of the Scarff-Bloom-Richardson grading system) for BC (24). Immunohistochemical analyses were performed on formalin-fixed, paraffin-embedded tumor sections for hormone receptor (27), HER2/neu expression and proliferation index (Ki67). HER2/neu positivity was defined according to the American Society of Clinical Oncology – College of American Pathologists (ASCO – CAP) guidelines as an immunohistochemical staining of 3+ or 2+ with evidence of gene amplification at FISH (28). Immunohistochemical detection of Ki67 was performed on the Ventana BenchMark XT automated staining platform (Roche Diagnostics GmbH, Mannheim, Germany) according to manufacturer's instructions. Ki67 proliferative index in surgical specimens was assigned by the pathologist on the basis of the percentage positive on at least 500 neoplastic cells counted in the peripheral area of the nodule. A cut–off value of ≥20% was used in all association analyses, according to the recommendations of the St Gallen International Expert Consensus on the primary therapy of early BC 2013 (29).
Statistical analysis. Sample size of the study was based on the agreement to inclusion criteria and willingness to provide informed consent rather than on sample size calculations. However, estimation was later performed and showed that, the recruited population was capable of yielding a power >90%, at a two-sided 5% significance level. This was based on the assumption of a true hazard ratio (HR) of at least 2 (based on previous meta-analyses on breast cancer (6, 7)), an accrual period of no less than 5 years and a median survival of 3 years.
Data are presented as percentages, mean (SD), or median and interquartile range (IQR). The NLR cutoff value was generated by receiver operating characteristic (ROC) curve analyses performed by MedCalc Statistical Software version 13.1.2 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2014). Area under the curve (AUC) was calculated to investigate whether NLR could distinguish between recurrent and non-recurrent patients. The NLR value with the best Youden index was selected as the cutoff value. DFS and OS represented the study endpoints. DFS was calculated from the date of enrollment until relapse of disease. OS was calculated from the date of enrollment until death from any cause. If a patient had not relapsed or died, DFS or OS were censored at the time of the last follow-up. Survival curves were calculated by the Kaplan–Meier method and the significance level was assessed according to the log-rank test using a computer software package (Statistica 8.0, StatSoft Inc., Tulsa, OK). Cox-proportional hazards analysis was performed by MedCalc Statistical Software version 13.1.2 to evaluate the association between pathological staging, NLR and survival outcomes. For administrative censoring, follow-up was ended the date of December 31st, 2017. All tests were two-tailed and only p-values lower than 0.05 were regarded as statistically significant.
Results
Clinical-pathological characteristics of the recruited population are summarized in Table I. BC was re-staged according to the 8th edition of the AJCC anatomic and prognostic TNM staging systems. Patients' distribution into the two different TNM groups is reported in Table II. As shown, BC re-staging according to the prognostic system resulted in a significant patient relocation. In particular, 65.4% (n=121) and 4.9% (n=9) of the 185 patients with anatomic stage II were reclassified as stage I and III, respectively. Similarly, 19.2% (n=20) and 20.2% (n=21) of the 104 patients with anatomic stage III were reclassified as stage I and II, respectively. Only one patient with stage I was reclassified as stage II according to the prognostic staging system (Table II). Consequently, the proportion of patients with stage I significantly increased from 30.7% to 57.3% (p<0.0001).
Median pre-treatment NLR was 2.0 (IQR=1.54 to 2.72 (10th – 90th percentile boundaries: 1.20-4.18)). Based on value distribution, patients were then categorized as having definitely negative (≤1.2), probably negative (≤1.5), possibly negative (≤2.0), possibly positive (>2.0), probably positive (>2.7), or definitely positive (>4.2) NLR values. ROC curves were then generated to identify the optimal NLR cutoff. Bayesian analysis is summarized in Table III, showing that a cutoff level of 2 yielded the best performance with a positive likelihood ratio of 1.45 (95%CI=1.2-1.8) and a negative likelihood ratio of 0.62 (95%CI=0.4-0.9). Univariate association analysis showed that patients with NLR >2 were more likely in an advanced stage of disease (p=0.001), owing to larger tumors (p=0.001), nodal involvement (p=0.017), or distant metastasis (p=0.040), but no association was observed with molecular types or individual prognostic factors (data not shown).
Clinical follow-up is currently ongoing. At the time of administrative censoring, 411 (86.5%) of the 475 BC patients were clinically free of disease, whereas 64/475 (13%) patients had local recurrence (n=22 (4.6%), 2 died of disease) or distant metastasis (n=42 (8.9%), 10 died of disease). Overall, there was a significant association between elevated pre-treatment NLR and BC recurrence (46% vs. 66%, p=0.002). In particular, 50% (11 of 22) and 74% (31 of 42) of BC patients with NLR above the cutoff had loco-regional or distant recurrence, respectively, compared to 46% of patients who remained free of disease (Chi-square=12.4; p=0.002).
Univariate Cox proportional hazards survival analysis showed that an elevated pre-treatment NLR was associated with a worse DFS (HR= 2.28 (95%CI=1.40-3.72)). Figure 1 demonstrates the Kaplan–Meier DFS curves for the entire cohort stratified on the basis of pre-treatment NLR. As shown, patients with NLR >2 had a worse 5 year survival rate compared to patients with NLR below this cutoff (74% vs. 89%, log-rank=3.24, p=0.0012). A detailed DFS analysis in prognostic stage subgroups is summarized in Table IV, showing that the prognostic value of NLR was mostly evident in early stages, particularly stage I BC (HR=2.89 (95%CI=1.21-6.89)). Of interest, NLR significantly stratified BC patients who developed distant metastasis either in the entire cohort (HR=3.29 (95%CI=1.79-6.03)), or in stage I BC (HR=4.62 (95%CI=1.45-14.73)). Conversely, NLR had no value in the prediction of local recurrence (whole cohort: HR=1.24 (95%CI=0.54-2.88); stage I BC: HR=1.39 (95%CI=0.34-5.65)) (data not shown). Figure 2 demonstrates the Kaplan–Meier DFS (Panel A) and distant metastasis-free survival (DMFS) (Panel B) curves for stage I BC patients stratified on the basis of pre-treatment NLR.
Clinical-pathological characteristics of breast cancer (BC) patients.
Stage distribution of 475 primary breast cancer patients according to the 8th edition of the AJCC anatomic and prognostic staging systems.
Receiver Operating Characteristics (ROC) and Bayesian analysis of neutrophil–to–lymphocyte ratio.
Five-year cumulative survival rates of breast cancer women at different stage of disease (classified according to the 8th edition of the AJCC prognostic staging system).
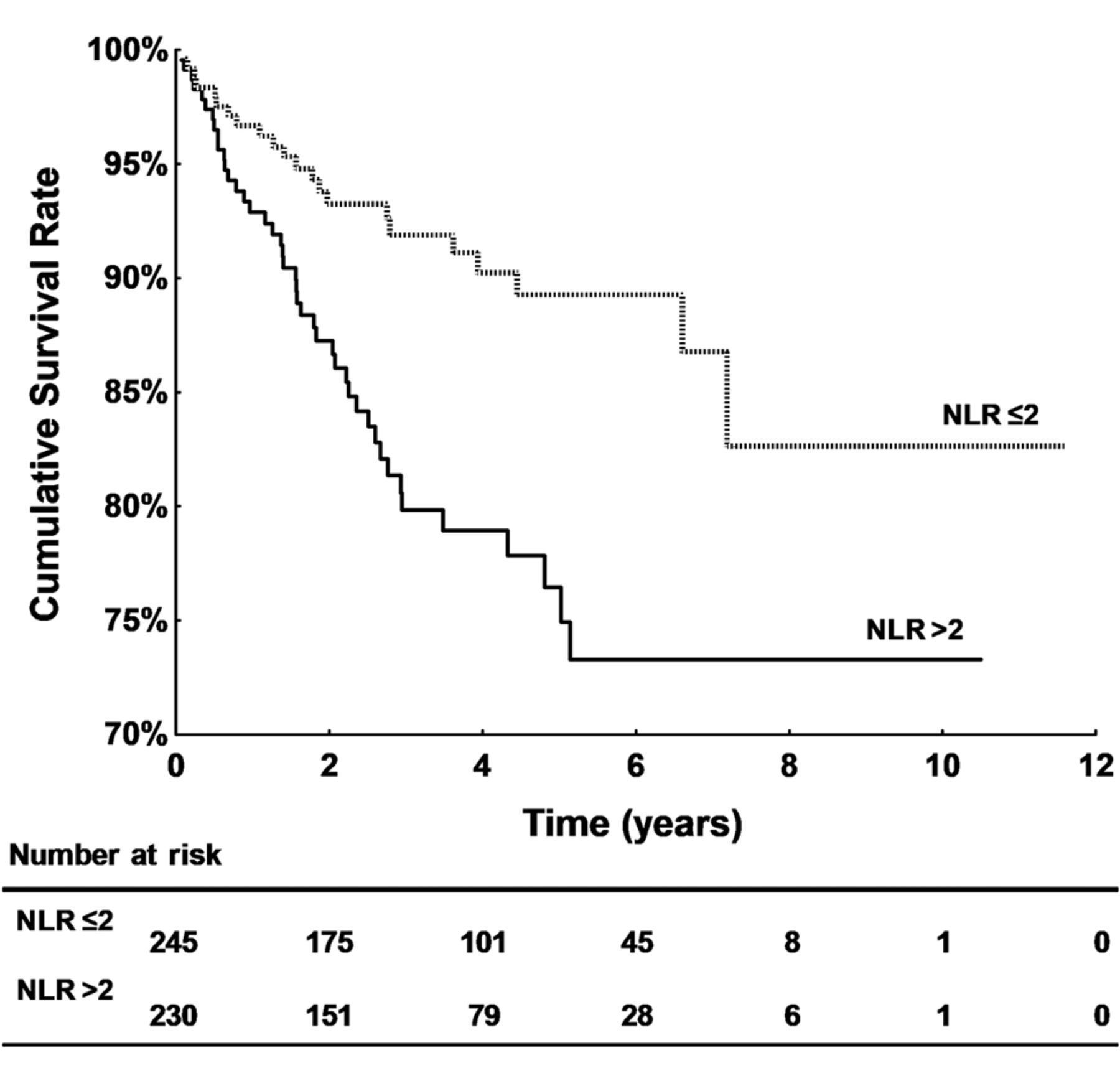
Kaplan–Meier curves of disease-free survival (DFS) of patients with breast cancer. Comparison between patients with low (dotted line) and high (solid line) neutrophil-to-lymphocyte ratio (NLR).
Finally, the prognostic significance of NLR for OS was evaluated. As shown in Table IV and Figure 3A, elevated pre-treatment NLR had a negative prognostic value in terms of OS (HR= 3.39 (95%CI=1.09-10.5)), with a survival rate of 95% compared to 99% of BC women with NLR values below the cutoff. Also, in this case, high NLR was associated with a worse OS mostly in patients with prognostic stage I BC (HR=1.30 (95%CI=1.03-1.64)) (Figure 3B).
Discussion
The results reported here confirm and extend previous studies on the prognostic role of NLR in BC. In particular, while confirming that a high NLR associated with a worse DFS and OS – with HRs similar to those reported by other groups (6, 7) – no association was observed between NLR and molecular types or individual prognostic factors, with the exceptions of tumor size and lymph node involvement, which were significantly associated with high NLR at univariate analysis. This finding is in agreement with the results obtained in a recent study conducted in a cohort of Italian women with early BC, demonstrating an association with T2 and N1 stage, but not with all other prognostic variables (30). Other studies, mostly involving BC patients of Asian race, have reported variable associations with hormone receptors (6, 16, 23, 31), HER-2 expression (6, 23), or molecular type (17, 19, 21, 22, 32, 33), although with conflicting results (10, 13, 20, 26, 34). To explain these discrepancies, Wei et al. advocated the fact that studies from Eastern countries had a positive result with perfect homogeneity, contrarily to that achieved in studies from Western countries, advocating the use of race-related cutoff values in future studies (5). On the other hand, Orditura et al. properly pointed out that the survival of BC Asian is longer than that of BC Caucasian women (30), which might be due to differences in the genetic backgrounds of Asians and Caucasians, as well as social-environmental factors, including lifestyle and dietary habits. However, regardless of the underlying reason, no consensus has been reached, yet, on which BC patient cluster can mostly benefit from NLR inclusion in the clinical workout for BC.
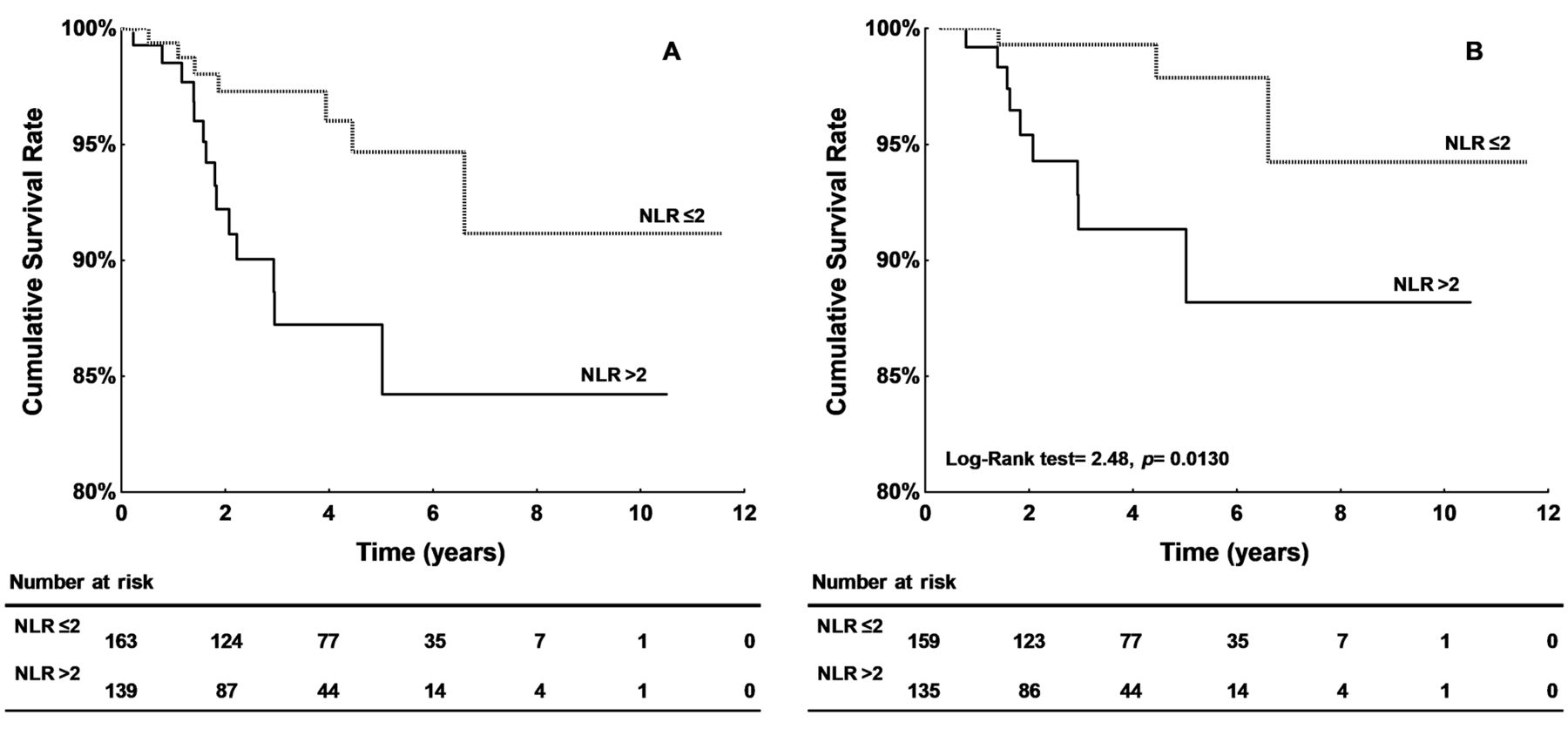
Kaplan–Meier survival curves of patients with prognostic stage I breast cancer. Comparison between patients with low (dotted line) and high (solid line) neutrophil-to-lymphocyte ratio (NLR). A: Disease-free survival. B: Distant metastasis-free survival.

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curves of overall survival of patients with breast cancer. Comparison between patients with low (dotted line) and high (solid line) neutrophil-to-lymphocyte ratio (NLR) in the overall population (A) and prognostic stage I BC women (B).
Indeed, BC is universally recognized as a heterogeneous disease composed of distinct biological subtypes with variable prognosis and therapeutic response (29, 35-37) and, although clinical decision making based on validated prognostic factors has largely contributed to decrease mortality, BC is still the leading cause of cancer death among females worldwide (38). Thus, in an attempt to improve survival stratification, the AJCC expert panel has extended the use of non-anatomic prognostic factors and biomarkers to assign a prognostic BC stage TNM in addition to the traditional anatomic TNM (24).
In this context, we hypothesized that the prognostic value of NLR could be modified in the newly proposed prognostic staging. Thus, we sought to analyze the DFS and the OS of BC patients after re-staging according to the 8th edition of the TNM. The results obtained showed that increasing rates of patients with high NLR – at a 2-point cut-off established by ROC analysis – could be steadily demonstrated from stage I to stage IV, both in the anatomic (p=0.001) and prognostic (p=0.001) TNM. Moreover, Cox proportional hazard survival analyses showed that an elevated pre-treatment NLR was associated with a worse DFS (HR=2.28) and OS (HR=3.39). This was true for the entire cohort of patients, as well as the subgroup of BC women with prognostic stage I (DFS: HR=2.89; OS: HR=1.30), but not in stages II to IV, in which the small number of patients might have weakened the statistical power. In the present study, in fact, re-staging according to the prognostic system resulted in a significant patient relocation to prognostic stage I, which included, at last, nearly 60% of the recruited population.
One final issue is the demonstration, for the first time to our knowledge, that NLR may represent a negative prognostic factor for DMFS, but not for loco-regional recurrence. Actually, the finding of an association between high NLR and poor DMFS (as shown in the Kaplan–Meier curves reported in Figure 2B) is in agreement with a recent study demonstrating that an elevated NLR – at a cutoff similar to that calculated in our study (1.97 vs. 2.0) – was an independent prognostic factor related to poor DMFS in Italian women with stage I and IIA BC (30). However, no data were reported regarding other outcome measures, in particular for loco-regional recurrence (30). Here, we demonstrated that the association observed between elevated pre-treatment NLR and BC recurrence was primarily due to the high proportion of patients with NLR >2 who developed distant metastases (74%), while the percentage of patients with high NLR was similar between patients who had loco-regional recurrence (50%), or those who remained free of disease (46%). Accordingly, NLR significantly associated with a worse DMFS, but not with local recurrence-free survival, both in the entire cohort of primary BC and in stage I disease.
There are, of course, certain limitations to our study that need to be acknowledged. First, the relatively small sample size might have weakened the statistical power especially in subgroup analyses. Moreover, NLR analysis was conducted as a retrospective procedure, although all eligible consecutive patients within the designated timeframe were included and all measurements were performed at time of recruitment. In addition, tests were run by a single laboratory under ongoing quality control protocols, which minimized the difference in sample analyses. On the other hand, the strength of our analysis is represented by the use of samples collected and processed in the context of two large Biobanks using shared standard operating procedures. Finally, the presence of a shared clinical database ensured the homogeneity and correct definition of the prognostic stage, as advocated by the AJCC expert panel.
Conclusion
To date, numerous surrogate biomarkers of inflammation have been evaluated either in vivo or in vitro for BC, but none has entered common use in a clinical setting. Among these, NLR might represent an attractive choice, thanks to its ease of use and low cost, especially in low–middle income regions where the public health decision-making cannot afford more costly solutions. Its prognostic value, however, should be regarded with caution and detailed clinical evaluation is needed before the ultimate prognostic significance of NLR in BC can be determined. Additional studies are required to prospectively evaluate the clinical value of pre-treatment NLR in BC, or its predictive significance for treatment response (31, 32, 39) and/or adverse events (40). Nevertheless, we believe that its determination might provide important information regarding risk stratification, especially in stage I patients in whom the presence of high NLR might raise the question as to whether they should be more aggressively managed.
Acknowledgements
The Authors express deep gratitude to all patients and their families for providing the opportunity to conduct the present research project. The Authors also wish to thank Laura Detto, RN and Elena Manganelli, RN, from the San Giovanni Hospital-Addolorata and Lorena Perrone, RN, Emanuela Durante, RN, Sabrina Amorosi, RN, and Daniela Lo Giudice, RN, from the Medical Oncology Unit, Tor Vergata Clinical Center, who enthusiastically supported the researchers and contributed to the overall success of the project. This work has been partially supported by the European Social Fund, under the Italian Ministry of Economic Development, Grant “HORIZON 2020” PON I&C 2014-2020 – NET4HEALTH (CUP B88I17000350008).
Footnotes
* These Authors contributed equally to this study.
This article is freely accessible online.
Conflicts of Interest
All Authors declare no conflict of interest in connection with this paper.
- Received June 26, 2018.
- Revision received July 1, 2018.
- Accepted July 5, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved