

Abstract
Background/Aim: Although there is an increasing number of studies on laparoscopic resection of early gastric cancer (EGC), as of 2018 no standardized strategy exists. We reviewed available literature dealing with laparoscopic intragastric (intraluminal) surgery (LIGS) conducted for patients with EGC to better define indications, benefits and limitations of this particular minimally invasive technique. Materials and Methods: PubMed, MEDLINE, Science Direct, Scopus, Web of Science, Google Scholar and ResearchGate were the search engines investigated. Only LIGS for EGC was entertained; studies conducted for other gastric diseases were excluded. Suitable articles written in all languages were included in the review. Results: As of 2018, we found 19 studies dealing with LIGS for EGC: studies on 72 humans and four pigs were identified. Among 72 human participants, there were 59 mucosal, five submucosal and one subserosal cancer. Conclusion: Based on our review, LIGS appears as a cogent option to endoscopic resection for treating superficial EGC.
- Early gastric cancer
- laparoscopy
- intragastric surgery
- intraluminal surgery
- intragastric mucosal resection
- intragastral resection
- review
In the past two decades, better knowledge on pathobiology of gastrointestinal stromal tumor (GIST) and early gastric cancer (EGC), as well as the more frequent detection of these two diseases, have increased the interest in minimally-invasive resection techniques (1). On the one hand, endoscopists have developed techniques such as endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD) and endoscopic full-thickness resection (EFTR); on the other hand, due to the evolution of laparoscopy, gastrointestinal surgeons approach GC by switching progressively from traditional interventions to minimally invasive segmental resections (1). Among the new possibilities, the combination of laparoscopy with endoscopy, the so-called hybrid laparoscopic approach, represents one of the most interesting procedures. With reference to dissection and resection of the tumor, the hybrid approach includes two main types of procedures: in the former, laparoscopy resects the tumor under endoscopic guidance, in the latter endoscopy and laparoscopy cooperate on an equal basis (1). Endoscope-assisted laparoscopic wedge resection and laparoscopic intragastric (intraluminal) surgery (LIGS) belong to the first group, whereas laparoscopic endoscopic cooperative surgery (LECS), laparoscopy-assisted EFR, clean non-exposure technique and non-exposed endoscopic wall-inversion surgery form the second (1-20). Irrespective of the adopted choice, common objectives of all techniques are an easier approach to the gastric lesion, shorter length of hospital stay with minor economic impact and respect for oncological principles. Regarding LIGS, as of 2018, pertinent studies enrolled patients with both benign and malignant lesions, making the actual evaluation of this practice in GC difficult (2-20). Furthermore, most work combined LIGS with other minimally invasive treatments, rendering the appraisal even more laborious (2-20). Herein, we offer a systematic review of the literature dealing with LIGS performed for EGC only: to date, as far as we are aware, no report of such a dedicated effort has been published.
Materials and Methods
We systematically reviewed world literature dealing with LIGS for EGC; studies or data on LIGS conducted for other gastric diseases were excluded. With this intent, seven popular search engines were investigated (PubMed, MEDLINE, Science Direct, Scopus, Web of Science, Google Scholar and Research Gate). “Intragastric surgery“, “laparoscopic intragastric surgery“, “minimally invasive intragastic surgery“, “robotic intragastric surgery“, “EGC and “GC“ were the key words utilized for searching. Suitable articles written in any language from 1994 until 2018 were included in the review.
Results
We found 19 studies dealing with LIGS for patients with EGC (2-20). Table I summarizes the principle features of the studies included in this review.
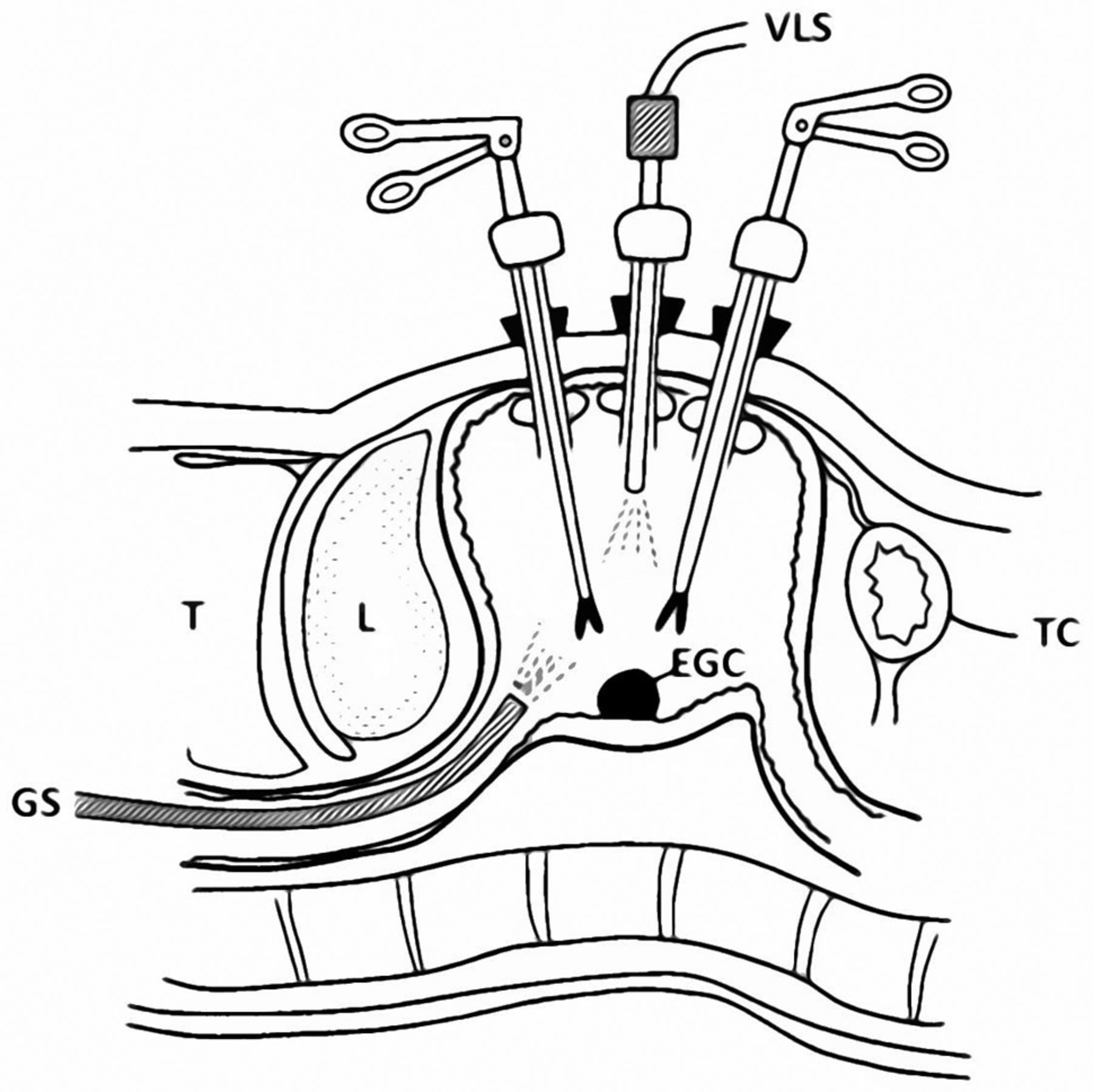
Surgical technique: original description and following variants. The first to pioneer LIGS was Ohashi in 1994 (2). He introduced this new technique for three patients affected with different gastric lesions: giant polyp, submucosal tumor (leiomyoma), and mucosal EGC (2) (Figure 1). All the lesions measured 2 cm in diameter and were located at the cardia, fornix and on the posterior wall of gastric body. LIGS resulted from a combination of laparoscopy with endoscopy and can be briefly described as follows (Figure 1): general anesthesia, peroral insertion of a gastroscope to visualize the gastric lesion, placement and inflation of a balloon (inserted along with a nasogastric tube) in the duodenum to prevent air flowing from the stomach to the intestine, insertion and fixation of three trocars in the stomach (three different methods are possible) under gastroscope guidance, laparoscopic mucosal resection, specimen extraction by gastroscope via the mouth or by a bag through the trocar, bleeding control and closure of the abdomen. Ohashi outlined two main features of this technique: lesions located in any part of the stomach were amenable to LIGS except those of the anterior gastric wall because of the technical difficulty; the resected gastric portion could be left untreated as a mucosal defect since gastroscopic examination performed on all patients 1 to 2 weeks after the operation demonstrated complete healing in all cases (2, 3). In 1996, however, Lai and colleagues preferred to suture mucosal defects through a minilaparotomy (4). Since then, the two approaches to mucosal defects (conservative vs. operative) varied through articles, sometimes leaving the mucosal defect untreated according to Ohashi's method (12), other times comparing both options (8, 10). However, there are also cases in which no mention was provided (13). In 2009, Yumiba et al. prospectively demonstrated that mucosal defect healing was faster and more advantageous in economic terms following closure with a continuous suturing of 4-0 Vicryl than an observational method (p≤0.014) (10). In addition to absorbable suture material, fibrin coating also represented an occasional method for sealing (9).
Concerning the depth of dissection following mucosal excision, differently from submucosal tumors, where it is deepened to the muscular layer, in the case of EGC, it is confined to submucosal plane (7). In 2009, however, Wong and coauthors performed a deeper dissection: combining LIGS with endoscopy (endolaparoscopic intragastric tumor excision) to treat 12 patients with gastric lesions (including two tumors with provisional diagnosis of EGC), they associated an endoscopic submucosal resection with laparoscopic seromuscolar dissection (16). As for the trocar types, occasionally intragastric access was unconventionally gained through percutaneous endoscopic gastrostomy (10) or a 5-mm radially expandable sleeve (8). In 2007, Hirano and coauthors first employed robotic intragastric surgery (da Vinci Surgical System) in a porcine model with a tentative EGC sited along the posterior wall of the cardia (20); although the experiment was successful in terms of operative time (approximately 41 minutes only) and absence of complications, to date no robotic attempt on humans has been reported.
Main features of enrolled patient populations. Altogether, 72 patients with EGC patients were reported to have undergone LIGS (2-18). Age and sex were not always reported; among the detailed data, the age ranged between 59 and 82 years (3, 13). Regarding the mucosal depth of EGC invasion, there were 59 cases of T1a and five of T1b cancer; information was lacking for seven patients. Additionally, one lesion with provisional diagnosis of EGC had invaded into the subserosa (pT2b or pT3 according to the sixth or seventh edition of the American Joint Commitee on Cancer (AJCC) tumor node metastasis staging system for GC, respectively] (16). Tumor size, where declared, ranged from 0.5 to 3 cm (5, 16). The posterior wall of the gastric body was the most frequent site of EGC in 32 definite cases; the anterior wall of the gastric stump and cardia were described in one and three cases, respectively (3, 13, 17, 18). Besides the 72 human participants, LIGS was also adopted for four porcine models (19, 20).
Clinical and oncological outcome. Surgery-related complications included three cases of stenosis at the gastric cardia (treated with repeat endoscopic dilatations) (5, 6), one perforation (necessitating repair though laparotomy) (9), tub cases of bleeding flowing from mucosal defect (treated conservatively in the former and with open conversion in the latter) (12, 14) and one hemorrhage from an abdominal port site managed with re-laparoscopy (16).
Surgical margins of the specimen showed infiltration (R1) in three cases. One R1 case derived from a T1b cancer of the antrum: the authors entertained distal gastrectomy as corrective surgery, but a decision had not yet been undertaken at the time of publication (11). Another R1 lesion originated from a T1a EGC: in this patient, reoperation was not immediately performed in expectation of cauterization effects. However, from endoscopic examination at the 28-month follow-up, it recurred as EGC stump and distal gastrectomy was performed (14). A further R1 cancer ensued from a cardial ulcer of 3 cm in diameter which showed dysplasia on preoperative endoscopic biopsy; however, final pathology revealed a well-differentiated adenocarcinoma invading into the subserosa (pT2b or pT3 according to the sixth or seventh edition AJCC classification) (16). Hence, in this case, the authors were misled by preoperative findings and conducted LIGS erroneously; as oncological salvage, they adopted laparoscopic-assisted total gastrectomy with an uneventful recovery.
{kind=link}
Illustration of laparoscopic intragastric surgery as originally conceived by Ohashi in 1994. VLS: Videolaparoscopy; EGC: early gastric cancer; TC: transverse colon; GS: gastroscope; T: thorax; L: liver.
One recurrence was found near the cardia of a patient 2 years after LIGS was carried out for mucosal cardial EGC; as the lesion was only 5 mm in diameter, the patient was successfully treated by endoscopic laser irradiation (5). Another mucosal recurrence developed 2 years after the initial surgery and was managed with gastrectomy; in this case, however, we were unable to find details as to whether the initial intervention was LIGS or laparoscopic wedge resection (5, 6).
Of interest, in 2005, Ludwig and colleagues combined LIGS with sentinel lymph node biopsy in three patients with T1a cancer: no tumor cells were found in dissected lymph nodes (15).
Discussion
Laparoscopic intragastric (intraluminal) surgery, also termed laparoscopic endoluminal surgery, laparoscopic intragastric mucosal resection or laparoscopic intragastral resection in the reported studies was conceived by Ohashi to provide a minimally invasive successful option for treating those gastric lesions (including EGCs) that were problematic for EMR (2-20). It has been reported that many EMR specimens were histologically positive for cancer at the surgical margin in up to 26% of cases (14). Thereafter, due to advances in EMR (such as the introduction of insulated-tip electrosurgical knife) and development of ESD and EFTR allowing en-bloc resections of much larger EGCs and reduction of the recurrence rate, employment of LIGS came to a standstill (12). Nevertheless, to date, it still represents a cogent surgical treatment for superficial EGC located at the posterior wall of the stomach as well as in cardial or pyloric regions where EMR and ESD are more difficult to perform (9). Furthermore, the concomitant accomplishment of lymph node dissection and sentinel lymph node biopsy constitutes an advantageous oncological feature (15). However, such a promising technique is not exempt from limitations, complications or potential inconveniences. First of all, it demands surgical skills and a necessary learning curve (12). Second by, lesions located at the anterior gastric wall are excluded from indication for obvious anatomical reasons (laparoscopic trocars are passed through the ventral gastric wall) (2-20). Thirdly, surgery-related complications (such as bleeding, perforation and stenosis), as well as oncological incompleteness (R1 and recurrent cases), can inadvertently take place (5, 6, 9, 11, 12, 14, 16). 0Finally, although very low and more probable with other hybrid laparoscopic techniques (such as LECS, inverted LECS, laparoscopy-assisted EFR and non-exposed endoscopic wall-inversion surgery, the risk of scattering of cancer cells from gastric lumen to peritoneal cavity remains a possibility (19, 21-25). Such a dreaded adverse event can potentially happen when the integrity of the gastric wall is compromised: this is mainly due to the fact that EGC can intragastrically exfoliate following the sixth metastatic route as previously demonstrated (26-31). Any phase of intervention can be affected: the beginning, when the gastric wall is punctured with ports or wires; the in-between course, especially in the case of perforation but also because laparoscopic devices touching and capturing the floating intragastric malignant cells might cause consequent intraperitoneal dissemination; and in the end phase, laparoscopic collection of the specimen might cause tumor implantation in gastric wall defects or abdominal port sites in the case of bag rupture or contaminated laparoscopic devices (32-34). To prevent or reduce the risk of such mishaps, careful endoscopic guidance during laparoscopic intragastric maneuvers, minimal handling of the tumor, as well as preoperative intragastric lavage and postoperative intraperitoneal washing, represent oncologically appropriate prophylactic measures (21-25).
Conclusion
Among minimally invasive hybrid techniques, LIGS represents a valid option for treating superficial EGC. Randomized controlled trials are welcome to better define the surgical oncological highlights and weak points of this interesting procedure.
Main features of the available studies dealing with laparoscopic intragastric surgery for early gastric cancer (EGC).
Footnotes
Conflicts of Interest
The Authors declare no conflicts of interest in regard to this study.
- Received January 12, 2018.
- Revision received February 9, 2018.
- Accepted February 13, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved