

Abstract
The purpose was to evaluate efficacy and safety of carbon ion radiotherapy (C-ion RT) in patients with locally advanced olfactory neuroblastomas (ONBs). This study was a sub-analysis of the Japan Carbon-Ion Radiation Oncology Study Group Study (1402 HN, UMIN000024473). Clinical data of T4 ONBs treated with C-ion RT at four Institutions between November 2003 and December 2014 were retrospectively reviewed. Twenty-one patients underwent C-ion RT. Seven patients had T4a and 14 had T4b tumours without cervical node metastases. The median follow-up period was 39 (range=5-111) months. The 3-year overall survival and local control rates were 88.4% and 83.0%, respectively. Grade 4 late toxicity was observed in three patients, including ipsilateral optic nerve disorder (n=2) and ipsilateral retinopathy (n=1). C-Ion RT is effective and can be a curative modality for T4 ONBs. Prospective multicenter studies are warranted to confirm these findings.
- Olfactory neuroblastoma
- cancer of the head and neck
- carbon ion radiotherapy
- radiotherapy
- multicenter study
Olfactory neuroblastoma (ONB) of the head and neck is a rare malignant tumour that arises from the olfactory neuroepithelium in the upper nasal cavity with extension into the skull base, into the orbit and to the intracranial space (1, 2). Surgery is considered a curative treatment for localized ONB, while postoperative radiotherapy (RT) is necessary for advanced ONBs. Definitive RT alone is considered insufficient therapy for ONBs (3). In advanced cases, intracranial extension may pose a surgical challenge (4). Surgical resection followed by postoperative RT is associated with reduced local recurrence (5).
Although ONB has been traditionally regarded as a radioresistant tumour, RT has widely been used as part of the treatment algorithm in adjuvant and definitive settings.
Compared to photons, carbon ions (C-ions) offer a higher linear energy transfer and greater relative biological effectiveness (RBE) and therefore provide a higher probability of tumour control. The physical characteristics of C-ions, such as their Bragg peak and small lateral scattering, are theoretically superior to those of photons in that C-ions can allow a more localized delivery of the radiation dose.
This study is the first report for ONBs treated by C-ion RT. C-Ion RT for various head and neck radioresistant malignancies has shown excellent results. Jingu et al. reported clinical results of 37 patients with malignant melanoma of the head and neck who received C-ion RT with concurrent chemotherapy. The 3-year local control (LC) and overall survival (OS) rates were 81.1% and 65.3%, respectively (6). Koto et al. reported 3-year LC and OS rates of 76.9% and 59.1%, respectively, in 22 patients with locally advanced sinonasal adenocarcinoma + reated with C-ion RT (7). Therefore, C-ion RT might be a useful and potentially curative option for unresectable head and neck tumours, including ONBs.
In November 2003, following a clinical trial, the Ministry of Health, Labour and Welfare in Japan approved C-ion RT as a highly advanced medical technology. As of the end of 2014, there were four C-ion facilities functioning in Japan (Hospital of the National Institute of Radiological Sciences, Hyogo Ion Beam Medical Center, Gunma University Heavy Ion Medical Center and the SAGA-HIMAT Foundation). We conducted a retrospective multicentre study to assess the clinical outcomes of C-ion RT for head and neck malignancies [Japan Carbon-Ion Radiation Oncology Study Group (J-CROS) study: 1402 HN, UMIN000024473]. In this article, we report the results pertaining to a subgroup of patients with locally advanced T4 ONBs.
Patients and Methods
Eligibility. J-CROS 1402HN was a retrospective multicentre study conducted across four C-ion facilities in Japan. Patients provided informed consent for use of their personal information for research purposes. This study was approved by the Institutional Review Boards at each of the participant institutes and was carried out in accordance with the Declaration of Helsinki.
Patients with head and neck malignancies, including ophthalmic tumours, who received C-ion RT between November 2003 and December 2014 were included (UMIN000024473). The inclusion criteria were as follows: (a) histologically-confirmed malignancy, (b) no bone or soft-tissue tumours, (c) N0/1 M0 status, (d) medically inoperable tumours or refusal for surgery by the patient, (e) definitive intent, (f) measurable tumours, and (g) Eastern Cooperative Oncology Group performance status of 0-2 (8). Patients who had previously undergone irradiation for the same lesion were excluded. TNM classification of tumours was performed according to the seventh edition of the International Union Against Cancer (UICC) (9).
Nine-hundred and eight patients were enrolled in total. Of them, 21 patients with T4 ONBs (T4a: 7 and T4b: 14) were included in this analysis.
Evaluation of clinical outcome. LC was defined as no evidence of tumour regrowth in the planning target volume (PTV), including in the marginal region of the PTV. Regional control was defined as no evidence of regional lymph node recurrence or head and neck mucosal skip lesions outside the PTV. In normal tissues, acute and late reactions after C-ion RT were reclassified according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0 (10).
Statistical analyses. All survival times were calculated from the first day of C-ion RT. LC, OS, and cause-specific survival (CSS) rates were determined using the Kaplan–Meier method. Statistical analyses were performed using SPSS software, version 23 (IBM Corp., Armonk, NY, USA).
Results
Cohort characteristics. The patient and tumour characteristics for 21 patients are shown in Table I. All patients were re-staged according to the seventh edition of the Tumour-node-metastasis staging system of the UICC (9). Disease status in all 21 patients was classified as N0M0.
Treatment characteristics. C-Ion doses are expressed as photon-equivalent doses in Grays (Gy) (RBE) and were defined as the physical dose multiplied by the C-ion RBE. The biological flatness of the spread-out Bragg peak (SOBP) was normalized using the surviving fraction of human salivary gland tumour cells at the distal SOBP region where the carbon ion RBE was assumed to be 3 (11).
Patients and tumour characteristics.
Treatment characteristics.
Treatment characteristics of C-ion RT in all patients are shown in Table II. Schedule selection was dependent on the institution and not on the patient. The target reference point dose was defined as the isocenter, and the PTV encompassed the minimally 90% dose line of the reference point dose. None of the patients were administered prophylactic neck irradiation.
Neoadjuvant chemotherapy was administered to four patients: ifosfamide, cisplatin and etoposide for two patients; cisplatin and etoposide for one patient; and uncertain agent(s) in the case of one patient. Three patients with recurrence and one newly diagnosed patient had received chemotherapy prior to C-ion RT. None of the patients had received adjuvant chemotherapy.
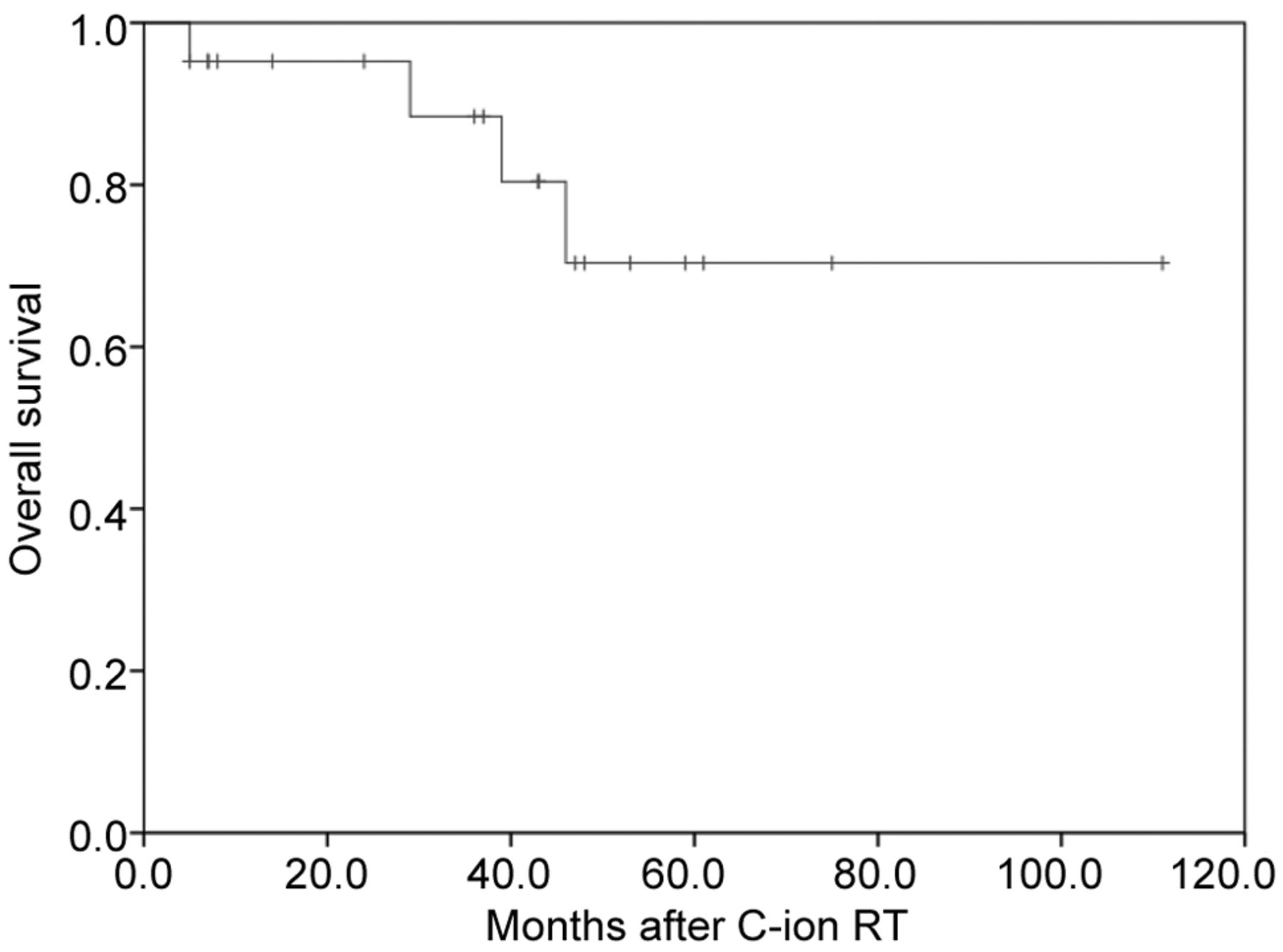
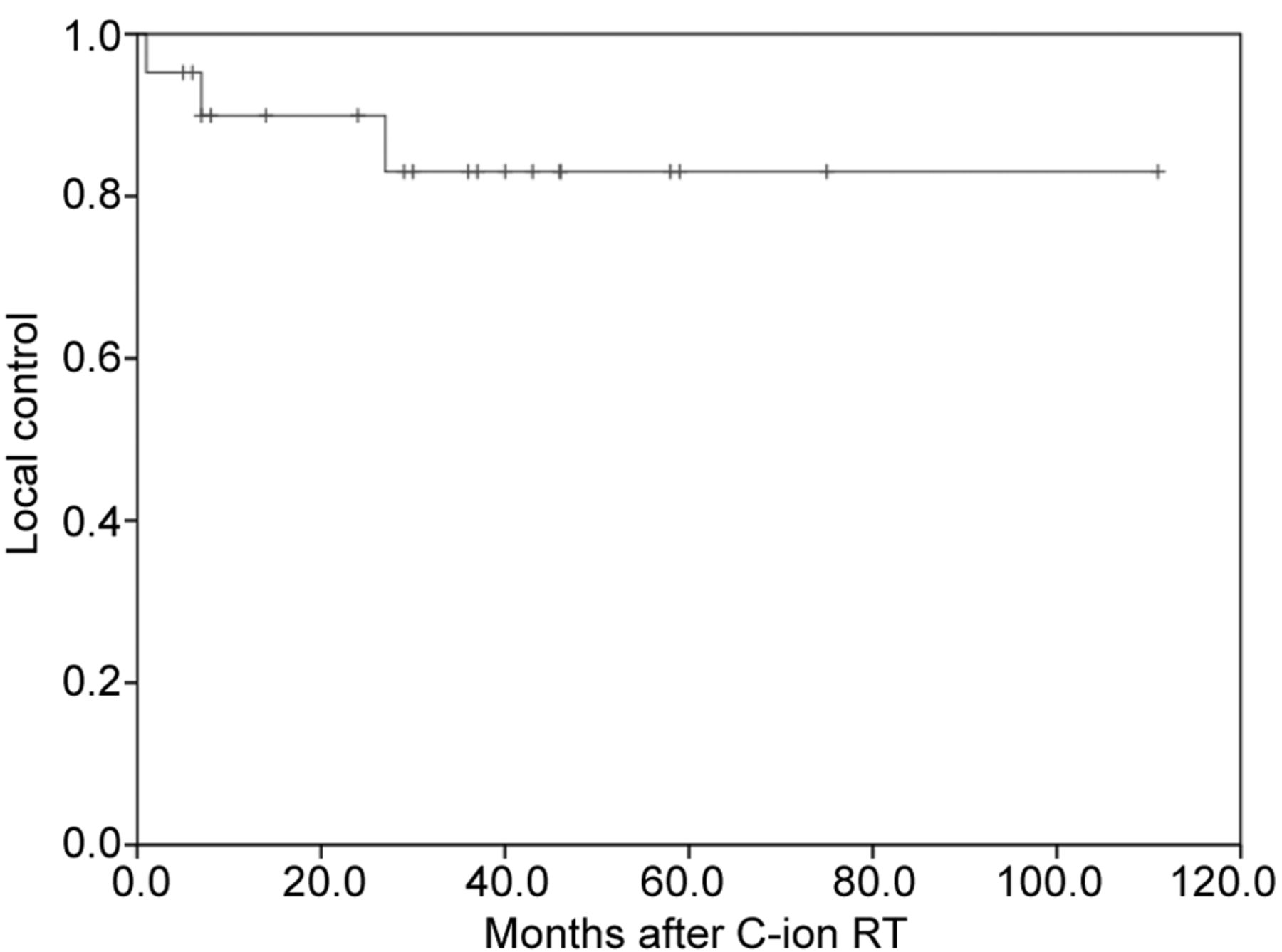
LC and survival. The median follow-up period was 39 (range=5-111) months. Three patients developed local recurrence within the PTV. The 3-year LC rate was 83% (Figure 1). The LC rate was not significantly correlated with the gross tumor volume (GTV) and C-ion RT dose. As of last follow-up, two patients had died of ONB and two of unrelated causes. Six patients developed distant or nodal metastases (bone in two patients; cervical nodes in two patients; lung in one patient; data not available in one patient). The 3-year OS and CSS rates were 88.4% and 88.4%, respectively (Figure 2).

Local control rate after carbon ion radiotherapy (C-ion RT) in patients with locally advanced olfactory neuroblastoma (n=21). Both 3- and 5-year local control rates were 83.0%.
{kind=link}
{kind=link}
Overall survival after carbon ion radiotherapy (C-ion RT) in patients with locally advanced olfactory neuroblastoma (n=21). The 3- and 5-year survival rates were 88.4% and 70.3%, respectively.
The number of late toxicity (grade 2 or more).
Acute and late toxicity to normal tissues. A total of four patients developed grade 3 or higher C-ion RT-related acute toxicity. Grade 3 mucositis was observed in two patients. None of the patients experienced grade 4 or higher acute toxicity. The late toxicities are shown in Table III. With regard to visual function, three patients developed ipsilateral blindness (grade 4) and one developed grade 3 ipsilateral visual impairment. The causes of blindness were optic neuropathy in two patients and retinopathy in one patient. The median period between the initiation of C-ion RT and the occurrence of ipsilateral blindness was 16 (range=9-29) months. The GTV was 39.3 (range=34.9-62.6) cc in three patients with blindness, and the tumours were in close proximity to the orbit. Except for eye disorders, grade 3 or more late toxicity was not encountered.
Discussion
ONB is a very rare disease that has been consistently associated with poor outcomes. Given the rarity of ONB, most published series were retrospective and had a small number of patients (12-15). In our knowledge, prospective clinical outcomes of ONB have not been reported. Ozsahin et al. reported 5-year OS and LC rates of 64% and 70%, respectively, with multimodality therapy including surgery, RT and chemotherapy for T1–T4 ONBs (16). McLean et al. reported 5-year OS rate of 58% in an ONB population of 21 patients with multimodality therapy including surgery, RT and chemotherapy (17). In the present study, all patients had T4 ONBs; the OS and LC at 3 and 5 years were 88.4% and 70.3%, and 83.0% and 83.0%, respectively. These OS and LC values in a population of inoperable T4 ONBs in our study seemed favourable to those achieved with multimodality therapy in populations comprising all stages of ONBs (Table IV).
Treatment outcomes in recent reports.
The reference period for our study exceeded 10 years; advances in surgical techniques and extended use of anticancer treatment over this period may have influenced patient outcomes. Modalities of RT have also evolved from 2D simulation to computed tomographic simulation (3DCRT) and, more recently, to use of intensity modulated RT (IMRT) technique. Mori et al. reported excellent results (5-year OS: 88% and 5-year progression-free survival rate 74%) with multimodality therapy used 3DCRT and IMRT (18). Nishimura et al. reported a 5-year OS rate of 93% and 5-year LC rate of 84% with use of proton beam RT; however, half of all patients were operable state of Kadish A and B, which precludes a direct comparison with our results (19). Both proton beam RT and multimodality using IMRT and 3DCRT were considered effective treatments for ONBs. C-Ion RT might be one of effective treatments for locally advanced ONBs.
To our knowledge, this is the first report on use C-ion RT for locally advanced ONBs. Currently, there is no consensus on C-ion dose and fractionation. This study was a retrospective multicentre study, therefore, dose fractionation schedules of C-ion RT were not unified. Approximately 70% of patients were treated with 57.6-64.0 Gy (RBE)/16 fractions, while the remaining patients were treated with 65.0 or 70.2 Gy (RBE)/26 fractions. In the three patients that developed local recurrence, the prescribed doses were 60.8 Gy (RBE)/16 fractions, 64.0 Gy (RBE)/16 fractions and 65.0 Gy (RBE)/26 fractions, respectively. There seems to be no clear correlation between local recurrence and dose-fractionation schedule. It is difficult to determine the optimal dose based on our data.
Nalavenkata et al. reported a high incidence of neck metastases (15.9%) and significantly lower OS in patients with delayed neck disease (73.8%) compared with that in the absence of delayed neck disease (91.8%) (20). In contrast, other studies appear to suggest that prophylactic neck irradiation may not be necessary in node-negative patients (15, 21). Although cervical node irradiation was not prescribed in this study, two patients experienced ipsilateral cervical node metastasis (33 and 57 months after C-ion RT). After cervical node resection, these two patients were still alive. Although the small number of patients makes it difficult to draw any definitive conclusions, we believe that cervical node resection is important in the event of nodal metastasis after C-ion RT.
In a study by Noh et al., none of the 17 patients with ONB developed cervical node metastases with systemic chemotherapy in the absence of cervical RT (15). However, a recent meta-analysis indicated that chemotherapy did not accrue any additional survival benefit in patients with ONBs (5). In our study, four patients received neo-adjuvant chemotherapy. Of these, one patient was treatment-naïve and three patients had disease recurrence. The present study does not allow for a valid assessment of the usefulness of chemotherapy for ONBs.
A few reports have referred to late toxicities. Noh et al. reported grade 3 or higher late toxicities of retinopathy, osteonecrosis and brain necrosis after multimodality therapy (15). Mori et al. reported a 17.6% incidence of grade 2 or more late adverse events (hypopituitarism and eye disorders) with use of 3DCRT and IMRT in 17 patients with ONBs (18). In this study, grade 3 or higher late toxicities occurred in four patients. Of these, two developed grade 4 ipsilateral optic nerve disorder, one grade 4 ipsilateral retinopathy, and one grade 3 ipsilateral retinopathy. The GTV of the three patients who developed blindness was 39.3 (range=34.9-62.6) cc and was larger than the median GTV 37.9 (range= 7.7-89.2) cc of all patients. Regarding optic neuropathy, which was a major cause of visual impairment, it was reported that a maximum C-ion RT dose of 52 to 57 Gy (RBE) to the optic nerve was a significant negative prognostic factor (22, 23). Anatomically, ONB develops from the olfactory epithelium and is in close proximity to the orbit. However, in cases where the tumor invades the orbit and is close to the optic nerve, it is difficult to reduce the C-ion RT dose to the optic nerve. In these patients, probability of visual impairment was predictable, and C-ion RT was performed only with sufficient informed consent prior to the treatment. Other than eye toxicity, none of the other patients developed grade 3 or higher late toxicity.
The present study had several limitations. Firstly, the number of enrolled patients was small due to the rarity of ONBs. Secondly, this study was performed using retrospective data; therefore, several different doses and fractionations of C-ion RT were included. Since April 2016, an integrated treatment schedule using 16 fractions over 4 weeks with a total dose of 57.6 or 64.0 Gy (RBE) has been applied in a multicenter prospective registry study of Japan. Thirdly, the present study could not use the Kadish classification (24) and the Dulguerov and Cakcaterra staging system (25). J-CROS 1402HN was designed as a retrospective multicentre study conducted across four C-ion facilities in Japan. We re-classified a total of 908 patients with various head and neck malignant tumours according to the seventh edition of the UICC TNM classification (9). Kadish C stage corresponds to T3 and T4 stage of the Dulguerov and Cakcaterra staging system. T3 stage of the Dulguerov and Cakcaterra staging system indicates tumour invasion into the orbit or frontal fossa without dural invasion. It is further subdivided into T4a and T4b stages by the seventh edition of the UICC TNM classification. T4 of the Dulguerov and Cakcaterra staging system corresponds to T4b by the seventh edition of the UICC TNM classification.
In conclusion, C-ion RT is an effective and potentially curative option for locally advanced ONBs, as an alternative to current multimodality therapy. Prospective multicentre studies are warranted to confirm these findings.
Footnotes
This article is freely accessible online.
Conflict of Interests
The Authors have no conflicts of interest directly relevant to the content of this article.
- Received November 27, 2017.
- Revision received December 14, 2017.
- Accepted December 18, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved