

Abstract
Background/Aim: Mitochondrial transcription factor A (mtTFA) is necessary for both the transcription and maintenance of mitochondrial DNA (mtDNA). The present study investigated the clinical significance of mtTFA in patients with right- and left-sided colorectal cancer (CRC). Patients and Methods: Surgical specimens from 237 CRC patients were immunohistochemically stained with polyclonal anti-mtTFA antibody. The relationships among the mtTFA expression, clinicopathological factors and prognosis were evaluated. Results: Thirty-five (60.3%) of 58 right-sided CRC patients and 82 (45.8%) of 179 left-sided CRC patients showed high mtTFA expression. The mtTFA expression significantly correlated with lymph node metastasis, distant metastasis, the TNM stage and lymphatic invasion in left-sided CRC patients and did not correlate with any factors in right-sided CRC patients. Univariate and multivariate analyses revealed the mtTFA expression to be a significant prognostic factor in left-sided CRC patients but not in right-sided CRC patients. Conclusion: These results suggest that a high mtTFA expression is a useful marker for tumor progression and a poor prognosis in left-sided CRC patients.
- Mitochondrial transcription factor A
- colorectal cancer
- mitochondrial DNA
In Japan, colorectal cancer (CRC) was estimated to be the most frequent cause of cancer-related deaths in females and the third-most frequent cause of cancer related deaths in males in 2014 (1). CRC is also one of the most lethal cancers in the world. With recent advances in chemotherapy, the overall survival of metastatic CRC has improved compared to 10 years ago. However, the prognosis of CRC still remains relatively poor. Therefore, the identification of prognostic factors that can select CRC patients at high risk for recurrence and that can predict chemosensitivity are needed.
The right-sided segment of the large bowel, including the appendix, cecum, ascending colon and transverse colon, arises from the embryonic midgut and receives blood flow from the superior mesenteric artery. In contrast, the left-sided segment of the large bowel from the splenic flexure to the upper anal canal arises from the embryonic hindgut and receives blood flow from the inferior mesenteric artery. This gives rise to differences in the clinicopathologic, cytogenetic and molecular features between right- and left-sided CRC (2). Microsatellite instability (MSI) and chromosomal instability (CIN) are the two most frequently mentioned of these genetic differences. MSI-high tumors have been reported to be more frequent in right-sided CRC (3-5), while CIN has been reported to be more frequent in the left-sided CRC (3-5). CpG island methylator phenotype (CIMP) results from hypermethylation of cytosine at the CpG island in the gene promoter, which leads to tumor suppressor gene silencing and carcinogenesis. CIMP was found to be significantly associated with right-sided CRC (6), and independently associated with a markedly poor prognosis in overall CRC patients (7).
Mitochondrial transcription factor A (mtTFA) is a member of the high mobility group (HMG)-box protein family (8) and stimulates the transcription of mitochondrial genes by binding to the mitochondrial displacement loop (D-loop) region (9, 10). mtTFA is involved in not only the transcription of mtDNA but also in its replication, recognition of mtDNA damage, stabilization of mtDNA and, indirectly, in the repair of mtDNA (11).
Several clinical studies have examined the status of the mtTFA expression in endometrioid adenocarcinoma (12, 13), CRC (14) and pancreatic ductal adenocarcinoma (15, 16). Our previous study in a small population indicated that high mtTFA expression in CRC significantly correlated with lymph node metastasis, distant metastasis and advanced TNM staging. The survival of patients with high mtTFA expression was significantly worse than that of patients with low mtTFA expression. High mtTFA expression seems to be a useful marker for tumor progression and a poor prognosis in patients with CRC (14).
However, the significance of mtTFA expression in right- and left-sided CRC patients has not yet been evaluated. Therefore, the present study investigated the difference in the clinical significance of mtTFA expression between right- and left-sided CRC patients.
Patients and Methods
Patients. A total of 58 right-sided CRC patients and 179 left-sided CRC patients who underwent surgery at the Department of Surgery 1, University Hospital of Occupational and Environmental Health (UOEH), Japan, from 1997 to 2003 were recruited to this study. All of the intended procedures in the present study, including the use of specimens from human subjects, were approved by the Ethics Committee of UOEH. The clinical data of these patients are summarized in Table I. No patients had received chemotherapy or radiotherapy before surgery. The clinicopathological findings were determined according to the UICC tumor-node-metastasis (TNM) classifications (17).
Anti-mtTFA antibody. Regarding the immunohistochemical staining of mtTFA, the anti-mtTFA polyclonal antibody was generated by multiple immunizations of a New Zealand white rabbit using synthetic peptides, as described previously (18). This antibody has been described in previous manuscripts (13, 14, 16).
Immunohistochemical staining of mtTFA and the evaluation of mtTFA. Immunohistochemical staining of mtTFA was performed on formalin-fixed 2-μm sections of tissues embedded in paraffin. These sections were deparaffinized in xylene and then rehydrated. Endogenous peroxidase was blocked with 0.3% hydrogen peroxidase in methanol for 10 min. After washing with phosphate-buffered saline (PBS), the sections were preincubated with 10% rabbit serum albumin in PBS for 10 min at room temperature. The slides were then incubated with the anti-mtTFA antibody for 2 h at room temperature (dilution 1:400). Antibody binding was visualized using the EnVision+ Dual link system with diaminobenzidine as the chromogen (Dako Cytomation, Kyoto, Japan). The slides were counterstained with methyl green and mounted. Immunostained slides were analyzed independently by two researchers. Differences were resolved by simultaneous viewing. The expression of mtTFA in the CRC samples was evaluated according to the methods previously described (13, 14). The cases were judged as “(−)” or “(±)” when no immunostaining was identified or when only minimal occasional staining (<5%) was present, respectively, focally positive (+) when staining of at least 5% but less than 50% of the tumor cells showed immunoreactivity, and diffusely positive (++) when at least 50% of the tumor cells showed immunoreactivity. Finally, the cases were classified into two groups based on low (− or ±) or high (+ or ++) expression.
Immunohistochemical staining of ssDNA and the evaluation of the apoptotic Index. Immunohistochemical staining of single-stranded DNA (ssDNA) was performed on formalin-fixed 2-μm sections of tissues embedded in paraffin. These sections were deparaffinized in xylene and then rehydrated. After endogenous peroxidase was blocked, the sections were preincubated with 10% goat serum albumin in PBS for 15 min at room temperature. The slides were then incubated with the ssDNA antibody (IBL, Gunma Japan) for 60 min at a room temperature (dilution, 1:100). Antibody binding was visualized using the EnVision+ Rabbit/IIRP (Dako Cytomation) with diaminobenzidine as the chromogen. The slides were counterstained with Mayer hematoxylin and mounted. ssDNA staining was evaluated in each section by counting the frequency of labeled cells in 5 high-power fields containing 100 tumor cells each. The apoptotic index (AI) was defined as the percentage of tumor cells with nuclei immunoreactivity among the total tumor cells.
Immunohistochemical staining of Ki-67 and the evaluation of the MIB-1 index. Immunohistochemical staining of Ki-67 was performed on formalin-fixed 2-μm sections of tissues embedded in paraffin. These sections were deparaffinized in xylene and then rehydrated. After endogenous peroxidase was blocked, the slides were subjected to microwave treatment in 10mM citrate buffer (pH 6.0) for 10 min. After washing with PBS, the sections were preincubated with 10% rabbit serum albumin in PBS for 10 min at room temperature. Immunohistochemical staining for Ki-67 antigen was performed using a monoclonal mouse anti-human Ki-67 antibody Clone MIB-1 (Dako Japan). The slides were then incubated with Ki-67 antibody for 1 h at room temperature (dilution 1:50). After washing with PBS, the slides were treated with anti-mouse immunoglobulin for 20 min and were then incubated with streptavidin-biotinylated horseradish peroxidase complex (LSAB kit/HRP: Nichirei, Tokyo, Japan) for 10 min. The slides were incubated in PBS containing diaminobenzidine and 1% hydrogen peroxidase for 10 min, counterstained with Mayer's hematoxylin, and mounted (19). The proliferative activity of the tumor cells was assessed by the MIB-1 index, which was determined as the percentage of tumor cells showing positive staining of nuclei reactive among the total tumor cells counted (19).
Clinicopathological assessment. The tumors were staged by two pathologists who had no prior knowledge of the results of the assays, according to the UICC tumor-node-metastasis (TNM) classifications 7th edition (17). Clinicopathological factors such as age, gender, tumor size, histological type, depth of invasion, lymph node metastasis, distant metastasis and staging were analyzed for their association with the mtTFA expression.
Statistical analyses. The relationships between the parameters were also assessed statistically using the c2 test with the Stat View-J software package (version 5.0, SAS institute, Inc., Cary, NC, USA). The Kaplan-Meier method was applied to determine the survival, and statistical significance was calculated using the log-rank test. Univariate and multivariate analyses of the survival were performed using the Cox proportional hazards model. Statistical significance was established at the p≤0.05 level.

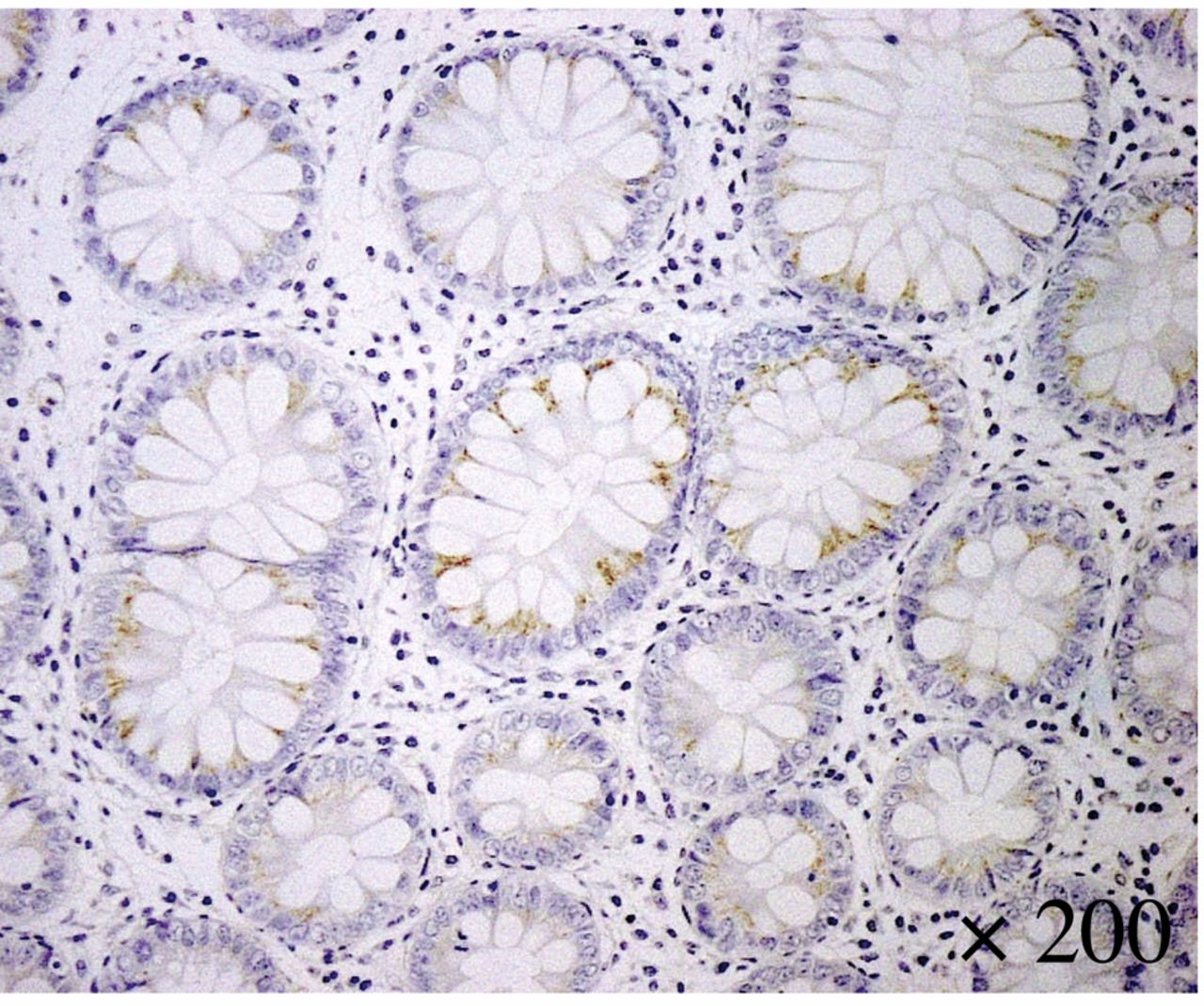
Immunohistochemical staining of mtTFA in normal colonic mucosa (×400).
Results
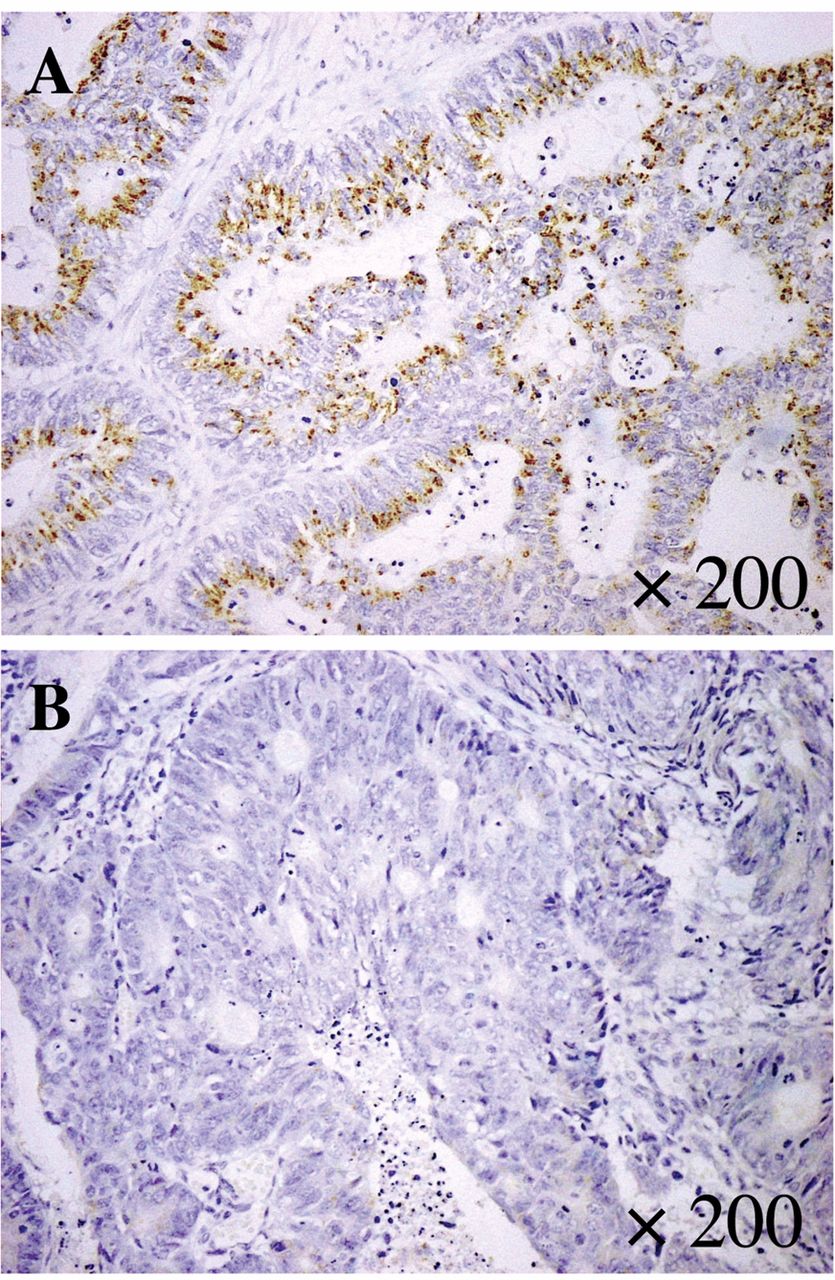
Table I shows the profiles of the 237 patients diagnosed with primary right-sided (58) and left-sided (179) CRC recruited for the present study. Immunohistochemical staining of endogenous mtTFA was performed on 58 right-sided and 179 left-sided CRC specimens. The expression of mtTFA was observed in the cytoplasm of the normal colonic mucosa (Figure 1). Positive signals (++) for mtTFA were observed in the cytoplasm of cancer cells (Figure 2A). Negative signals (−) for mtTFA were observed in the cytoplasm of cancer cells (Figure 2B). Thirty-five (60.3%) of the 58 right-sided CRC patients and 82 (45.8%) of the 179 left-sided CRC patients had high mtTFA expression.

Immunohistochemical staining of mtTFA in colorectal cancer specimens. Positive expression (++) of mtTFA (A) and negative expression (−) of mtTFA (B) (×400).

{kind=link}
{kind=link}
{kind=link}
The prognostic significance of mtTFA expression was analyzed using the Kaplan-Meier method in the patients with right-sided CRC (n=58) (A) and left-sided CRC (n=179) (B). The patients were divided into low and high groups according to the previous classification (14). The patients in the low mtTFA (mtTFA-L) group showed a significantly better prognosis in comparison to those in the high mtTFA (mtTFA-H) group in the patients with left-sided CRC (p=0.0143) (B) but not in the patients with right-sided CRC ((p=0.2018) (A).
Characteristics of the patients with right-sided or left-sided colorectal cancer.
The patients were divided into high- and low-MI groups, with the mean value of 43.6% as the cut-off value. A total of 125 patients (27 right-sided CRCs, 98 left-sided CRCs) had a high-MI, and 112 (31 right-sided CRCs, 81 left-sided CRCs) had a low-MI. The patients were also divided into high- and low-AI groups, with the mean value of 5.1% as the cut-off value. A total 124 patients (40 right-sided CRCs, 84 left-sided CRCs) had a high-AI, and 113 patients (18 right-sided CRCs, 95 left-sided CRCs) had a low-AI.
Based on the evaluation of the mtTFA immunostaining, the mtTFA expression significantly correlated with lymph node metastasis, distant metastasis, TNM stage and lymphatic invasion in left-sided CRC patients (Table II). In contrast, the mtTFA expression did not correlate with any factors in right-sided CRC patients (Table II).
Kaplan-Meier analyses for the overall survival based on the mtTFA expression were also performed (Figure 3). The median follow-up time was 93.06 months (range=1.0-185 months). The survival of patients with low mtTFA expression was not significantly better than that of those with high mtTFA expression (p=0.2018, Figure 3A) in right-sided CRC patients. However, the survival of patients with low mtTFA expression was significantly better than that of those with high mtTFA expression (p=0.0143, Figure 3B) in left-sided CRC patients.
Association between mtTFA expression and clinicopathological factors, A. I. and M. I. in the patients with right- or left-sided colorectal cancer.
Univariate analysis for clinicopathological factors, apoptotic index, MIB-1 index and the expression of mtTFA in the patients with right-sided or left-sided colorectal cancer.
In right-sided CRC patients, a univariate analysis indicated that the TNM stage, depth of invasion, lymph node metastasis, distant metastasis, lymphatic invasion and histological type were significant prognostic factors (Table III), and a multivariate analysis indicated that the depth of invasion, lymph node metastasis and distant metastasis were significant independent prognostic factors (Table IV). In contrast, in left-sided CRC patients, a univariate analysis indicated that the TNM stage, depth of invasion, lymph node metastasis, distant metastasis, lymphatic invasion, vessel invasion, histological type, MIB-1 index, apoptotic index, tumor size and the mtTFA expression were significant prognostic factors (Table III) and a multivariate analysis indicated that lymph node metastasis, distant metastasis, vessel invasion, MIB-1 index and the mtTFA expression were significant independent prognostic factors (Table IV).
Discussion
The findings regarding the prognosis of right-sided versus left-sided colorectal cancer are conflicting at present. Some studies have revealed a poor survival with a right-sided primary tumor location (20-24), while others have revealed poor or a similar survival based on a left-sided primary tumor location (25, 26). As the criteria for the recruitment of patients differ among these previous manuscripts, it may be difficult to evaluate and compare the results of these reports. While some studies evaluated the patients with Stage I-III disease (25, 26), other studies evaluated those with Stage I-IV (20, 21, 23). Furthermore, some studies have evaluated patients with colon cancer (20, 21, 25), while others have evaluated those with colorectal cancer (26, 27). In our study, there was no significant differences in the survival between right- and left-sided CRC patients (p=0.7504) including Stage I-IV disease. It is important to clarify the differences in prognostic factors or factors predictive of the therapeutic effect based on the location of CRC.
Multivariate analysis for clinicopathological factors, apoptotic index, MIB-1 index and the expression of mtTFA in the patients with right-sided or left-sided colorectal cancer.
Several reports have shown that a high mtTFA expression correlates with a worse prognosis by affecting tumor progression. In patients with endometrioid adenocarcinomas, the mtTFA expression was found to be significantly associated with the surgical stage, myometrial invasion, lymphovascular space invasion, cervical invasion and lymph node metastasis (13). In addition, this previous study indicated that the 10-year overall survival rate of the endometrioid adenocarcinoma patients with a high mtTFA expression was significantly worse than that of patients with a low mtTFA expression by a univariate, but not a multivariate, survival analysis (13). In pancreatic ductal adenocarcinoma, Yamauchi et al. indicated that the mtTFA expression played a pivotal role in worsening the postoperative clinical course through the induction of anti-apoptotic effects in pancreatic ductal adenocarcinoma cells (15). Other reports have indicated that the combination of mtTFA and survivin expression is an independent, novel and powerful marker for a poor prognosis in pancreatic ductal adenocarcinoma patients after surgery (16). Our previous small-scale study indicated that the survival of CRC patients with a high mtTFA expression was significantly worse than that of patients with a low mtTFA expression (14). In the present study, our data suggested that a high mtTFA expression might be a useful marker for tumor progression and a poor prognosis in left-sided CRC patients, but not in right-sided CRC patients.
Some studies have described the regulatory mechanism for the expression of mtTFA (28-33). An in vivo genomic footprinting study suggested that NRF-2 and Sp1 are probably involved in the regulation of the mtTFA gene in rat hepatoma (28). The in vitro methylation of the NRF-1 binding site suppressed the promoter activity of mtTFA (29). The overexpression of PGC-1 related coactivator (PRC) in oncocytic tumors induced mitochondrial biogenesis through NRF-1, resulting in an increase in mtTFA and mtDNA transcript levels (30). Another study described the redox regulation of NRF-1 phosphorylation and nuclear translocation by phosphatidylinositol 3,4,5-triphosphate kinase/AKt signaling, which controls the mtTFA induction by an anti-oxidant pro-survival network (31). Also, arsenic causes several human cancers. Chronic exposure to arsenic causes the increased cell survival, DNA damage and increased expression of mtTFA in human prostate epithelial cells (32). The expression of cytochrome c oxygen, mtTFA, NRF-1 and PGC-1apfha was increased in arsenic-induced Bowen's disease (33). The regulatory mechanism for mtTFA is not fully understood. However, the regulation of the mtTFA expression may be important as CRC patients with a low mtTFA expression have a favorable prognosis. More extensive studies about the regulation of mtTFA are needed.
Kurita et al. indicated that cellular expression of the antiapoptotic factor BCL2L1 was down-regulated following the transfection of siRNA knockdown of mtTFA in ovarian cancer cell lines (34). In addition, BCL2L1 promoter activity was increased after the transfection of a mtTFA expression plasmid but decreased after siRNA knockdown of mtTFA (34). mtTFA also regulates the BCL2L1 gene expression in ovarian cancer. Furthermore, increased apoptosis is observed in mtTFA-knockout mice, suggesting that mtTFA plays an important role in apoptosis (35). These studies suggested that mtTFA might be a molecular target of cancer therapy. The strong expression of mtTFA in patients with metastatic CRC was detected in 8 of 33 complete response/partial response patients (24.2%) and 18 of 26 stable disease/progressive disease patients (69.2%), indicating that mtTFA expression was significantly correlated with the response to chemotherapy (p<0.01) (36). The median overall survival of metastatic CRCs was significantly longer in patients without mtTFA expression than in those with it (36). This report suggested that the immunohistochemical study of mtTFA may be useful for predicting the clinical outcome of metastatic CRC patients treated with the FOLFOX regimen.
In conclusion, we found that a high mtTFA expression in tumor specimens may be a useful marker for both the progression of the tumors and for a poor prognosis of patients with left-sided CRC.
Acknowledgements
The Authors would like to thank Ms. Yuko Ueda for her technical assistance. This study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science and Culture of Japan.
Footnotes
Conflicts of Interest
The Authors declare that there are no conflicts of interest regarding the publication of this paper.
- Received September 29, 2017.
- Revision received October 17, 2017.
- Accepted October 18, 2017.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved