

Abstract
Background: Young women with endometrial cancer (EC) have an increased risk of synchronous ovarian cancer. The prognosis of women with synchronous endometrial and ovarian cancer (SEOC) is good. A high proportion of affected women have hereditary non-polyposis colon cancer syndrome (HNPCC). Case presentation: We present the case of a 45-year-old woman with histologically proven endometrioid adenocarcinoma of the endometrium (pT1B, G2, R0 without lymphovascular space invasion). She underwent laparoscopic hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy. Final histology revealed a synchronous bilateral endometrioid ovarian cancer (pT1A, G2, R0). HNPCC analysis by immunohistochemistry showed no microsatellite instability in MSH2, MSH6, MLH1, and PMS2. No adjuvant therapy was administered, clinical follow-up with regular gynecological examinations was recommended. In a systematic literature review, 2,904 cases of women with SEOC were identified with 1,035 (36%) of them being premenopausal or <50 years of age. The proportion of women with SEOC among all reported EC cases was 842/23,498 (3%) and the proportion of young women with SEOC among all reported EC cases was 261/23,498 (1%). In summary, microsatellite instability and subsequent mutations in mismatch repair genes compatible with HNPCC were identified in 6/15 (40%) women analyzed. The mean recurrence-free and overall survival times of young women with SEOC were 1.9 (min 0.2, max 3) and 4.0 (min 0.2, max 22.1) years, respectively. Conclusion: Young women with EC have a high risk of synchronous ovarian cancer. Thus, in young women with EC, bilateral salpingo-oophorectomy or careful histological assessment of both ovaries are recommended in order to confirm or rule out SEOC. HNPCC testing should be offered to all women.
- Ovarian cancer
- endometrial cancer
- synchronous cancer
- HNPCC
- young women
- cancer syndrome
- review
Endometrial cancer (EC) is the most common female pelvic malignancy with a life-time risk of 4% (1). It is usually diagnosed at an early stage and has a good prognosis accounting for only 2% of cancer-related deaths (1, 2). The most common age at the time of diagnosis is between 65 and 75 years with a mean age of 69 years (3). However, young women may also be affected by EC. Specifically, around 10% of women diagnosed with EC are <50 years of age with a range of 7 to 20% reported in the literature (1-4). This subset of women with EC is characterized by an elevated risk of synchronous ovarian cancer and an increased prevalence of hereditary non-polyposis colon cancer syndrome (HNPCC). This has important consequences for the management, prognosis, and genetic counselling of young women with EC.
In the general population of women with EC, synchronous ovarian cancer is a rare finding. In a Surveillance, Epidemiology, and End Results Program (SEER) database analysis of 56986 women with ovarian cancer, for example, Williams et al. identified 1709 (3%) cases of synchronous endometrial and ovarian cancer (SEOC) (5). Young women with EC, however, have a significantly higher risk of SEOC with a range of 11 to 29% reported in the literature (4, 6-11). The typical histology of SEOC is endometrioid adenocarcinoma in both the endometrium and the ovary, which is found in >70% of cases (12). Based on this high rate of histological congruence among SEOC cases, a monoclonal origin has been suggested (13). Specifically, Anglesio et al. proposed that the disseminating cells of SEOC may be restricted to physically accessible and microenvironment-compatible sites, i.e. the endometrium and the ovary, with a limited capacity for further dissemination (13). Others have confirmed a high rate of monoclonality among SEOC cases (14).
In case of SEOC, ovarian involvement may be interpreted as metastatic disease or synchronous primary ovarian cancer based on histology and immunohistochemistry. Immunohistochemistry is usually applied to distinguish between an ovarian metastasis of EC and primary ovarian cancer. Endometrioid adenocarcinomas of the endometrium typically express estrogen and progesterone receptors. Other frequently altered genes are KRAS, PTEN, and β-catenin (15). A subset progresses into high-grade carcinoma which is accompanied by loss of receptor expression and accumulation of TP53 mutations. Low-grade serous carcinoma of the ovary is also associated with KRAS mutations, but in contrast to EC typically expresses mutated BRAF (16). Another useful marker to differentiate between EC and ovarian cancer is PAX-8, because primary ovarian cancer but not EC metastases, express PAX-8 (17). The exact differential diagnosis between an ovarian metastasis and a second primary ovarian cancer, however, is difficult. In the series of Walsh et al., for example, the majority of cases (23/26 [88%]) were classified as synchronous primaries and only 3/26 (12%) were considered ovarian metastases of EC (12). To the contrary, Oranratanaphan et al. diagnosed synchronous primary ovarian cancer in 14/63 (22%) and ovarian metastases in 49/63 (78%) cases (4). Akbayir et al. described a 16/28 (57%) versus 12/28 (43%) distribution, respectively (7). This discrepancy in the literature underscores the difficulty of distinguishing between ovarian metastasis of EC and a second primary ovarian cancer, especially in cases of two endometrioid adenocarcinoma histologies. These difficulties in the differential diagnosis of SEOC are, however, important, because an exact distinction between ovarian metastasis and primary ovarian cancer has prognostic and therapeutic implications. For example, Oranratanaphan et al. reported a 5-year disease-free survival rate of 64% compared to 41% in the synchronous and metastatic groups, respectively and the 5-year overall survival rate was 92% versus 48% (4). In addition, patients with EC and metastatic disease in the adnexae would be classified as FIGO stage III cases and thus be eligible for adjuvant platinum-based chemotherapy with or without radiotherapy. On the other hand, patients with an EC and a second primary FIGO stage 1A ovarian cancer would be adequately treated with clinical follow-up alone (18).
Hereditary non-polyposis colon cancer syndrome (HNPCC) is an autosomal dominant genetic syndrome conferring a 85 to 90% life-time risk of colon cancer, a 40-60% life-time risk of EC, and a 6 to 12% life-time risk of ovarian cancer (19, 20). In unselected populations of women with EC, HNPCC is found in 9 to 11% of women (21). Young women with EC, especially those with SEOC, may even have a higher prevalence of HNPCC, although the exact rate of HNPCC in this subpopulation of women with EC is unknown.
To highlight the clinical and genetic characteristics, management, and prognosis of young women with SEOC, we report the case of a 45-year-old woman with histologically verified endometrioid adenocarcinoma of the endometrium and synchronous endometrioid ovarian cancer. In addition, we present a systematic review of the literature with case reports and case series of young women with SEOC and discuss common characteristics shared by these women.
Case Report
We present the case of a 45-year-old woman with histologically verified endometrioid adenocarcinoma of the endometrium and synchronous endometrioid ovarian cancer. In November 2016, the patient was diagnosed with therapy-resistant menstrual bleeding disorder. Dilatation and curettage was performed and histology revealed a moderately differentiated endometrioid adenocarcinoma of the endometrium. In December 2016, she underwent total laparoscopic hysterectomy and bilateral salpingo-oophorectomy. Intraoperative assessment of the depth of infiltration revealed an International Federation of Gynecology and Obstetrics (FIGO) stage 1B EC with tumor invasion into the outer third of the myometrium. Subsequently, staging surgery with laparoscopic pelvic lymphadenectomy was performed in the same session. Intraoperative frozen section analysis of the pelvic lymph nodes showed no evidence of pelvic lymph node metastases. The intraoperative and postoperative course of the patient was uncomplicated. The final histological report confirmed a moderately differentiated endometrioid adenocarcinoma of the endometrium (FIGO pT1B, G2, R0 without lymphovascular space invasion). In addition, a synchronous, bilateral, moderately differentiated endometrioid carcinoma of the ovaries (pT1A, G2, R0) was found. Figure 1 shows hematoxylin-eosin stains of the endometrial and ovarian tumor specimens. Figure 2 shows immunohistochemical studies with estrogen receptor, progesterone receptor, and PAX-8 expression for both tumor specimens. The patient had no family history of colon cancer, EC, breast, or ovarian cancer. HNPCC assessment by immunohistochemistry was performed and showed no microsatellite instability in the MSH2, MSH6, MLH1, and PMS2 proteins (Figure 3). No adjuvant therapy was administered. Follow-up with regular clinical gynecological examinations was recommended. The patient is well and alive without evidence of recurrent disease at the time of this report.

Hematoxylin-eosin stain of an endometrial cancer specimen sampled in 2016 demonstrating endometrioid adenocarcinoma of the endometrium (A) and a synchronous ovarian cancer specimen with endometrioid adenocarcinoma of the ovary (B). Black bar represent 100 μm.

Immunohistochemical stains of an endometrial cancer specimen demonstrating the expression of estrogen receptors (A) progesterone receptors (B) an ovarian cancer specimen demonstrating the expression of estrogen receptors (C), progesterone receptors (D) and PAX-8 (E). Black bars represent 50 μm.
Literature Review
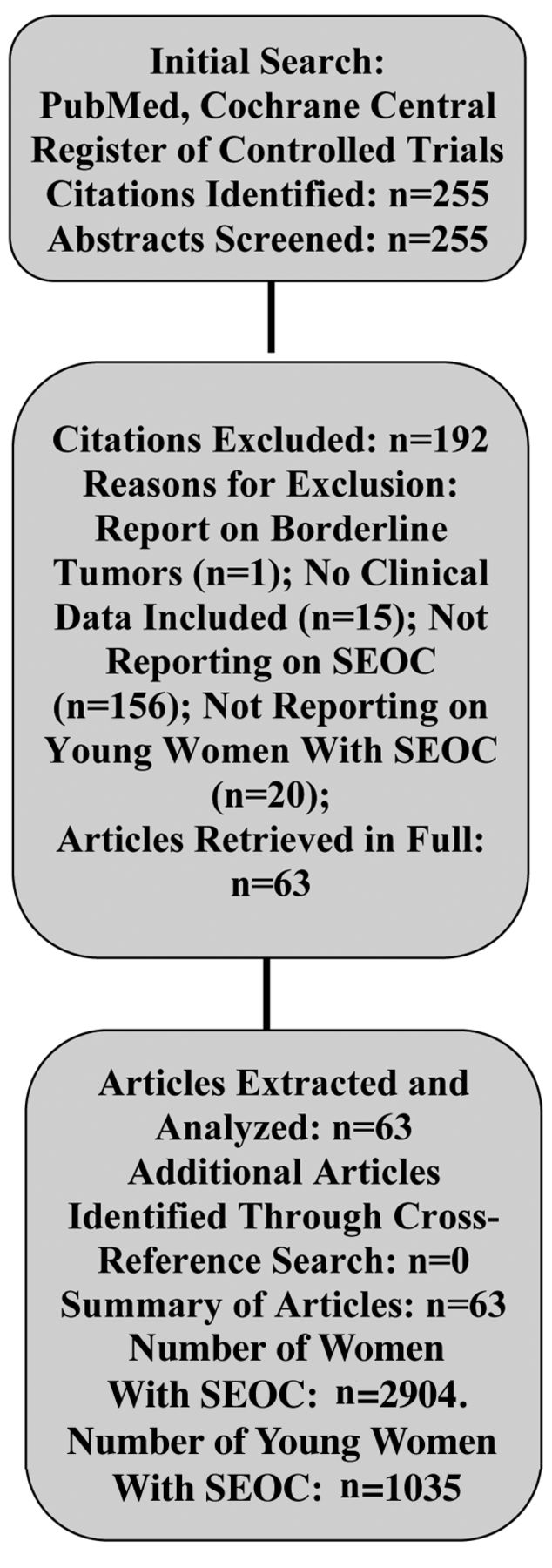
In a systematic literature search of the databases PubMed and Cochrane Central Register of Controlled Trials (search date 23-12-2016) using the search terms “synchronous[All Fields] AND endometrial[All Fields] AND (“ovarian neoplasms”[MeSH Terms] OR (“ovarian”[All Fields] AND “neoplasms”[All Fields]) OR “ovarian neoplasms”[All Fields] OR (“ovarian”[All Fields] AND “cancer”[All Fields]) OR “ovarian cancer”[All Fields]), we identified 255 studies. After screening all abstracts of these studies, 63 citations were identified reporting on young women with SEOC, defined for the purpose of this review as <50 years of age or premenopausal (4-10, 12, 13, 22-75). Studies not reporting on women with SEOC and studies reporting on women with benign ovarian tumors were excluded. Therefore, in summary, 63 studies were retrieved in full and analyzed for this review. Among these studies, we found 16 case reports, 8 retrospective cases series, 38 retrospective cohort studies, and one prospective cohort study. Figure 4 shows a diagram of the literature search. Table I shows the study characteristics and outcomes of patients with SEOC described in all 63 studies. In summary, 2904 women with SEOC were reported with 1035 (36%) of them being premenopausal or <50 years of age. In 28 of 63 studies, the number of EC cases, among which women with SEOC were identified, was reported. The proportion of women with SEOC among all reported EC cases was 842/23498 (3%) and the proportion of young women with SEOC among all reported EC cases was 261/23498 (1%). Among women with SEOC, most cases of EC and ovarian cancer were early stage tumors with 72% of EC cases classified as FIGO stage I disease and 70% of ovarian cancer cases classified as FIGO stage I disease. The predominant histologic type of SEOC was endometrioid adenocarcinoma in both the endometrium and the ovary. This combination was found in 694/1163 (60%) of SEOC cases.
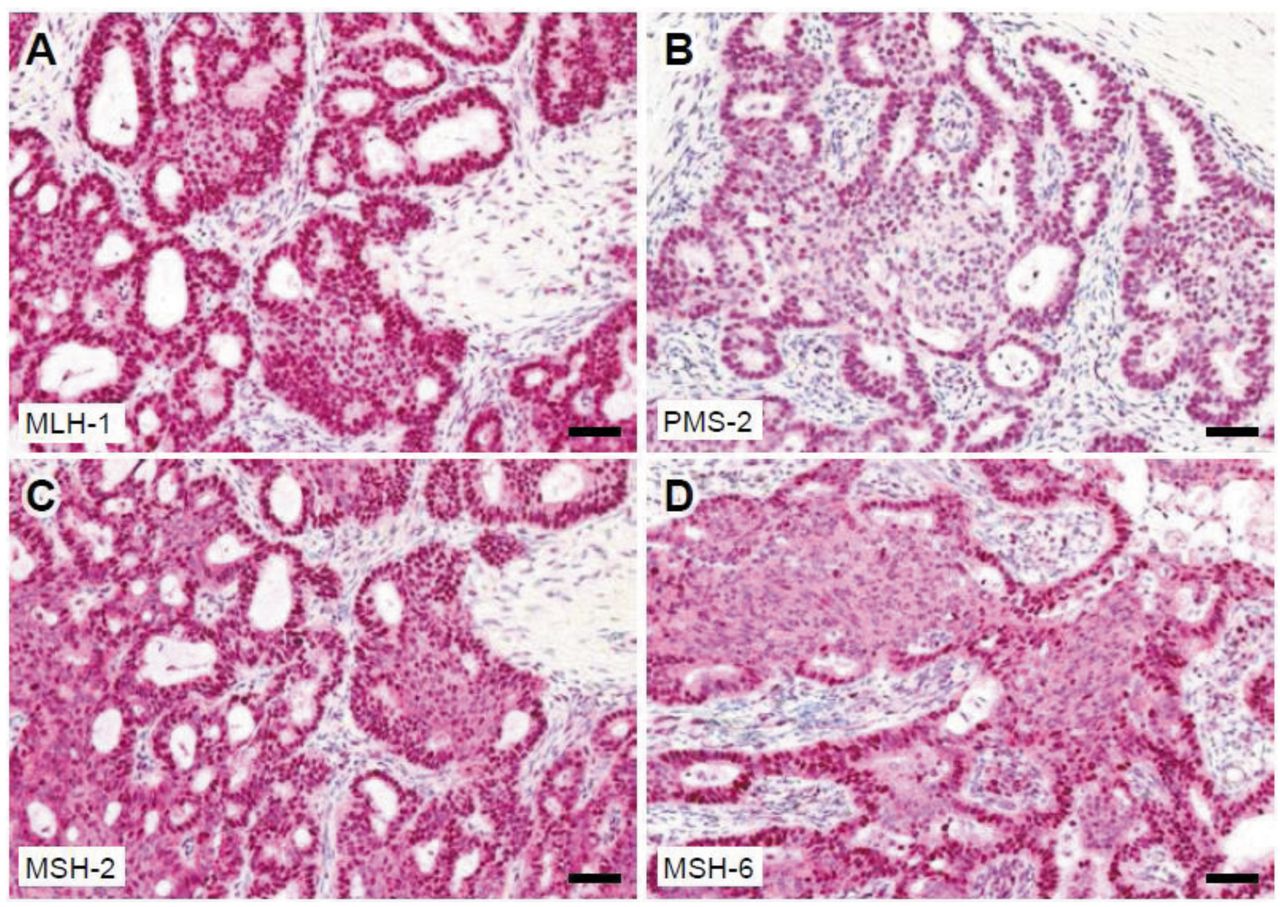
Immunohistochemical stains of an endometrial cancer specimen demonstrating the expression of MLH-1 (A), PMS-2 (B), MSH-2 (C) and MSH-6 (D). Black bars represent 50 μm.
The largest cohort of young women with SEOC was published by Williams et al. (5). In this population-based analysis of the SEER database, the authors identified 530 (39%) women <50 years of age among a population of 1355 SEOC cases. They compared the prognosis of women with SEOC and women diagnosed with ovarian cancer alone and found a 25% reduction in the risk of death. Interestingly, this effect was not only seen in early stage cases, but also in women with late stage cases suggesting a favorable prognosis for SEOC independent of tumor stage. In this study, no separate analysis of young women with SEOC regarding prognosis and stage distribution was performed. The five largest monocentric retrospective cohort studies with more detailed clinical data investigated between 157 (47) and 84 (30) SEOC cases. In these studies, the proportion of young women with SEOC varied considerably with 10% (9/93) (39), 17% (21/123) (61), 23% (36/157) (47), 48% (30/63) (4), and 51% (43/84) (30).
The only prospective cohort study recruiting women with SEOC was a Gynecologic Oncology Group (GOG) study published by Zaino et al. (29). In this study, 74 women with SEOC confined to the pelvis were prospectively enrolled, thus ensuring homogenous clinicopathologic characteristics and treatment regimens. A high proportion of women had microscopic spread of tumor in the pelvis or abdomen (23/74, 31%). Despite this fact, the probability of recurrence after 5 years was only 15% and the overall probability of surviving 5 and 10 years was 86% and 80%, respectively. The presence of microscopic metastasis in the pelvis or abdomen, however, discriminated two groups of patients with strikingly different probabilities of recurrence. Specifically, the 5-year recurrence rate was 27% for patients with compared to 10% for patients with microscopic metastases in the pelvis or abdomen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow diagram of the literature search algorithm.
The bulk of studies identified in this systematic review were retrospective cohort studies with <50 patients with SEOC (6-10, 12, 22, 24, 25, 28, 31, 34, 37, 38, 42, 44, 49, 51, 52, 55, 56, 58, 59, 61, 62, 65, 67-71), cases series of individual patients (13, 23, 35, 36, 43, 45, 66, 73), and case reports (26, 27, 32, 33, 41, 46, 50, 53, 54, 57, 60, 63, 64, 72, 74, 75). As expected, the heterogeneity among these studies with low numbers of patients was high. However, as shown in Table I, most patients had early stage disease of the endometrial and ovarian cancers and the predominant histology was synchronous endometrioid adenocarcinoma.
HNPCC analysis was performed in only 15/2904 young women with SEOC. Microsatellite instability and subsequent mutations in mismatch repair genes were identified among 6/15 (40%) of tumors analyzed (Table II). Mutations in the MSH2, MSH6, MLH1, and PMS2 genes were identified in 3, 1, 3, and 1 cases, respectively. Recurrence-free survival time and overall survival time were reported for 7 and 77 young women with SEOC, respectively. The mean recurrence-free survival time was 1.9 (min 0.2, max 3) years and the mean overall survival time was 4.0 (min 0.2, max 22.1) years.
Discussion
In this case report and review of the literature, we describe a young woman with synchronous endometrioid adenocarcinoma of the endometrium and both ovaries. HNPCC analysis showed no microsatellite instability in MSH2, MSH6, MLH1, and PMS2. We identified 2904 cases of women with SEOC in the literature with 1035 (36%) of them being premenopausal or <50 years of age. HNPCC analysis was only reported for 15 of these women with 6/15 (40%) demonstrating microsatellite instability and subsequent mutations in mismatch repair genes compatible with HNPCC. These data demonstrate that young women with EC have a high risk of synchronous ovarian cancer and a high proportion of HNPCC. Thus, in young women with EC, bilateral salpingo-oophorectomy or careful histological assessment of both ovaries are recommended in order to confirm or rule out SEOC. HNPCC testing should be offered to all women with SEOC.
Our data are comparable with previously reported studies on young women with SEOC. Based on our analysis, 3% of women with EC are young, i.e. premenopausal or <50 years of age, and a third of these women have SEOC. In accordance, our pooled analysis of the literature identified a proportion of 36% of young women among all women diagnosed with SEOC. This is compatible with the data of Williams et al. (5). They performed a population-based analysis of 1355 women with SEOC and identified 530 (39%) cases of premenopausal women (5). Together, these data show that young women with EC have a surprisingly high risk of SEOC. When managing young women with EC, treating physicians should be aware that a third of them will have synchronous ovarian cancer. It seems therefore reasonable to perform bilateral salpingo-oophorectomy or at least careful histological assessment of both ovaries by targeted biopsies in order to confirm or rule out SEOC.
Clinical studies describing women with synchronous endometrial and ovarian cancer.
Clinical studies describing mutational analysis and survival data among young women with synchronous endometrial and ovarian cancer.
The typical histology of SEOC is endometrioid adenocarcinoma of both the endometrial and the ovarian tumors, which has been described in up to 70% of cases (12). Our analysis confirms that the majority of SEOC cases are diagnosed at an early stage and display synchronous endometrioid adenocarcinomas in both endometrium and ovary. Specifically, we found that 72% of EC cases and 70% of ovarian cancer cases were classified as FIGO stage I disease. Endometrioid adenocarcinoma in both the endometrium and the ovary was found in 694/1163 (60%) of cases. This unusually early presentation of ovarian cancer, which is otherwise typically diagnosed at a late disease stage, may be interpreted as a chance finding during surgery for EC. An alternative explanation is a possible monoclonal origin of SEOC. For example, Anglesio et al. performed targeted and exome sequencing in 18 women with SEOC and found evidence of a clonal relationship in 17 of them (13). Others have confirmed these findings by subjecting cancer tissue from five SEOC cases to whole-exome massively parallel sequencing, demonstrating that the endometrial and ovarian tumor cells displayed strikingly similar repertoires of somatic mutations and gene copy number alterations in all investigated cases (14). These data suggest that in women with SEOC, the endometrium and the ovary represent microenvironment-compatible sites with preferential dissemination of tumor cells.
The prognosis of women with SEOC is good based on a high proportion of early stage cases and favorable histologies. In addition to these favorable clinicapthologic characteristics, the prognosis of women with SEOC seems to be better than that of women with single ovarian cancer, independent of tumor stage (5). This may be due to genetically-based restrictions of tumor dissemination in women with SEOC (13). In our analysis of survival data in the literature, the mean recurrence-free survival time of young women with SEOC was 1.9 years and the mean overall survival time was 4.0 years. These survival data underscore that young women with SEOC still have a compromised outcome and guideline-compatible treatment regarding surgical staging and adjuvant treatment should be applied. In order to optimize the long-term outcome of young women with SEOC, the high risk of HNPCC should be recognized. Our data underscore the strong association of SEOC and HNPCC in young women. Specifically, we found that microsatellite instability and subsequent mutations in mismatch repair genes compatible with HNPCC are present in 40% of women. This is significantly higher than what has been reported in unselected populations of women with EC, where HNPCC is found in 9-11% of women (21). Therefore, despite the low number of SEOC patients in the literature analyzed for HNPCC mutations, HNPCC screening in all women with SEOC seems reasonable.
In conclusion, we found that young women with EC have a high risk of synchronous ovarian cancer and a have high risk of HNPCC. Thus, in young women with EC, bilateral salpingo-oophorectomy or careful histological assessment of both ovaries are recommended in order to confirm or rule out SEOC. HNPCC testing should be offered to all women with SEOC.
Footnotes
This article is freely accessible online.
Conflicts of Interest
Authors declare that they have no conflict of interest.
- Received January 10, 2017.
- Revision received February 12, 2017.
- Accepted February 20, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved