

Abstract
Background/Aim: Germline mutations in any of the succinate dehydrogenase (SDH) genes result in destabilization of the SDH protein complex and loss of SDHB expression at immunohistochemistry. SDHA is lost together with SDHB in SDHA-mutated tumours, but its expression is retained in tumours with other SDH mutations. We investigated whether SDHA/SDHB immunohistochemistry is able to identify SDH-related tumours in a retrospective case series of phaeochromocytomas (PCCs) and paragangliomas (PGLs). Materials and Methods: SDHA and SDHB immunostaining was performed in 13 SDH gene-mutated tumours (SDHB: n=3; SDHC: n=1; SDHD: n=9) and 16 wild-type tumours. Protein expression by western blot analysis and enzymatic activity were also assessed. Results: Tumours harbouring SDH gene mutations demonstrated a significant reduction in enzymatic activity and protein expression when compared to wild-type tumours. SDHB immunostaining detected 76.9% of SDH mutated PCCs/PGLs (3/3 SDHB-mutated samples; 1/1 SDHC-mutated sample; 6/9 SDHD-mutated samples). In three SDHD-related tumours with the same mutation (p.Pro81Leu), positive (n=2) or weakly diffuse (n=1) SDHB staining was observed. All wild-type PCCs/PGLs exhibited SDHB immunoreactivity, while immunostaining for SDHA was positive in 93.8% cases and weakly diffuse in one (6.2%). SDHA protein expression was preserved in all tumours with mutations. Conclusion: SDHA and SDHB immunohistochemistry should be interpreted with caution, due to possible false-positive or false-negative results, and ideally in the setting of quality assurance provided by molecular testing. In SDHD mutation, weak non-specific cytoplasmic staining occurs commonly, and this pattern of staining can be difficult to interpret with certainty.
- Phaeochromocytoma
- paraganglioma
- immunohistochemistry
- succinate dehydrogenase
- SDHB
- SHDA
Succinate dehydrogenase (SDH), also referred to as mitochondrial complex II, plays an important role in cellular metabolism. SDH is involved in both the Krebs cycle, catalyzing the oxidation of succinate to fumarate, and the respiratory chain where it transfers electrons to coenzyme Q (1). It is encoded by four separate genes (SDHA, SDHB, SDHC, SDHD, collectively referred to here as SDHx), any of which may be mutated to cause hereditary phaeochromocytomas (PCCs) and paragangliomas (PGLs) (2).
The link between SDH and neuroendocrine tumours was discovered in 2000, when germline mutations in the SDHD gene were described in patients with familial PGL (3). These mutations were later recognised in patients with apparently sporadic PCC/PGL (2). Subsequently, germline mutations in the SDHB and SDHC genes were identified, as well as mutations in the gene encoding for the SDHA subunit (4). Initially, the latter was not associated with the occurrence of PCC/PGL, but with early onset of Leigh syndrome (4). Assembly of the SDH complex requires two factors: SDHAF1 and SDHAF2 (5, 6). SDHAF1 mutations are related to infantile leukoencephalopathy, while SDHF2 mutations are involved in the development of PGL but not of PCC (5, 6).
SDH genes are tumour-suppressor genes. They are generally affected by point-mutations (missense, nonsense, frameshift and splicing) and transmitted via an autosomal dominant pattern of inheritance, with varying degrees of penetrance. Genotypic alterations more often concern SDHD (7% of PCC/PGL) and SDHB (5% of PCC/PGL) genes. Mutations in the SDHC, SDHAF2 and SDHA genes are less frequent (1).
Germline mutations in any of the SDHx genes, as well as hypermethylation of the SDHC promoter region (7, 8), result in loss of SDHB protein expression, which is retained in wild-type and non-SDH-related tumours (9). Consequently, immunohistochemistry has been proposed for triage genetic testing in order to reduce time and costs. Recent findings indicate that SDHB immunohistochemical status strongly correlates with PCC/PGL clinical outcome, thus emphasising the role of SDHB immunohistochemistry as a prognostic marker (10-12). Loss of both SDHB and SDHA immunoreactivity is evident only in SDHA-mutated tumours, whereas SDHA expression is retained in the context of other SDHx mutations (4). In a retrospective case series, we investigated whether SDHx-related tumours can be identified by SDHA/SDHB immunohistochemistry.
Patients and Methods
Patients with PCC/PGL. Over the past 6 years, 106 patients were diagnosed with PCC/PGL at the Endocrinology Section of the University of Florence, Italy. For the present study, we selected 13 patients with SDHx mutation and 16 with wild-type SDHx, randomly chosen within the cohort. Following the protocol approved by our Local Ethical Committee (Prot. N. 2011/0020149), tissue specimens and blood samples were collected for DNA and mRNA analyses, as well as biochemical and morphological assays. All patients gave their informed consent. After surgery, tissues were immediately frozen in liquid nitrogen and stored at −80°C.
Genetic analysis. DNA was extracted from the peripheral blood leukocytes of each patient using the NucleoSpin Blood L kit (Macherey-Nagel, Düren, Germany) and analysed for germline mutations of SDHA (all exons), SDHB (all exons), SDHC (all exons), SDHD (all exons), SDHAF1 (all exons), SDHAF2 (all exons), Myc-associated factor X (MAX) (all exons), transmembrane protein (TMEM) 127 (all exons), von Hippel Lindau (VHL) (all exons), and rearranged during transfection (RET) (exons 5, 8, 10, 11, 13, 14, 15 and 16). For each gene, coding regions and exon-intron boundaries were amplified by polymerase chain reaction (PCR) as previously described (13). PCR products, purified with a commercial PCR purification kit (Qiagen, Milan, Italy), were subjected to 2% agarose gel electrophoresis with ethidium bromide staining and subsequently sequenced with a genetic analyser (ABI PRISM 310; Applied Biosystems, Milan, Italy).
Tissue homogenates and lysates. Unless specified, all reagents were purchased from Sigma (Sigma-Aldrich, Milan, Italy). Homogenates were prepared as previously described (14). Briefly, dissected tissues (50-150 mg) were finely chopped, re-suspended in a solution containing 120 mM KCl, 20 mM HEPES, 2 mM MgCl2, 1 mM EGTA, 5 mg/ml bovine serum albumin, and homogenized in a hand-held glass/glass homogenizer. The homogenates were centrifuged at 800×g for 10 min at 4°C and the enzyme assays were carried out on the supernatant. For western blot analysis, chopped tissues were lysed in a buffer (50 mM Tris-HCl, pH 7.5, 120 mM NaCl, 1 mM EGTA, 6 mM EDTA 15 mM Na4P2O7, 20 mM NaF, 1% Triton X-100 and protease inhibitor cocktail) homogenized in a hand-held glass/glass homogenizer and kept for 30 min on ice. Lysates were clarified by centrifugation at 10,000 × g for 15 min at 4°C. Supernatants were quantified for protein content (Coomassie Blue reagent; Bio-Rad, Hercules, CA, USA). All procedures were performed on ice or at 4°C.
SDH activity. Tissue homogenates (50 μg) were incubated in a phosphate buffer containing sodium azide, 2,6-dichlorophenolindophenol (DCPIP), sodium succinate, and phenazine methosulfate. Complex II specific activity was assessed by photometry, using a Victor3 1420 Multilabel Counter (Packard Instruments, Perkin-Elmer, Waltham, MA, USA), by measuring the decrease in absorbance due to oxidation of DCPIP at 600 nm (14).
Western blot. Samples of clarified lysates (30 μg of proteins) were separated by sodium dodecyl sulphate–polyacrylamide gel electrophoresis, and transferred onto polyvinylidene difluoride (Immobilon, Millipore, MA, USA), as previously described (15). Bound antibodies were detected using ECL reagents (Immobilon, Millipore, MA, USA) and analysed with a Biorad ChemiDoc Imaging System for dedicated chemiluminescent image acquisition (Imaging and Analysis Software by Bio-Rad, Quantity-One). The polyclonal anti-SDHB was from Sigma (HPA002868; Sigma-Aldrich, St. Louis, MO, USA), and the monoclonal anti-SDHA from Abcam (clone 2E3GC12FB2AE2; Abcam, Cambridge, UK). The polyclonal anti-actin and all the secondary antibodies, namely anti-rabbit, anti-mouse and anti-goat immunoglobulin G conjugated to horseradish peroxidase, were supplied by Santa Cruz Biotechnology (Santa Cruz, CA, USA).
Immunohistochemistry. Specimens were obtained by surgical resection in all cases and fixed in 10% formalin before being processed in paraffin. Haematoxylin-eosin stained sections from each specimen were reviewed by two pathologists to confirm the histological diagnosis.
For immunohistochemical analysis, a representative 3-μm section for each lesion was selected. All sections were deparaffinised in Bio-Clear (Bio-Optica, MiIan, Italy) and hydrated with series of graded ethanol concentrations to distilled water.
Antigen retrieval was performed by calibrated water bath capable of maintaining the epitope retrieval solution EDTA (pH 9.0) at 97°C for 20 min. Sections were then allowed to cool to room temperature for 20 min.
In order to block endogenous peroxidase activity, slides were treated with 3.0% hydrogen peroxidase in phosphate-buffered saline (PBS) for 10 min and, after washing with PBS (Dako Wash Buffer 10x) two or three times, was incubated with rabbit polyclonal anti-SDHB (1:800; Sigma-Aldrich, St. Louis, MO, USA) overnight at 4°C. Serial sections of the same specimen were immunostained with mouse monoclonal anti-SDHA (1:2000; Abcam) for 20 min at room temperature.
Immunohistochemical analysis was performed using DAKO EnVision™ FLEX (DAKO, Carpenteria, CA, USA) and 3.3’diaminobenzidine as the chromogen. Sections of PCC were used as positive control for SDHB and SDHA. Negative control was performed by substituting the primary antibody with a non-immune serum at the same concentration. Control sections were treated in parallel with the samples. The sections were lightly counterstained with Mayer's haematoxylin.
In accordance with Gill and co-authors, definite granular cytoplasmic staining was scored as positive and faint cytoplasmic blush as weakly diffuse (16). Cases lacking cytoplasmic staining in the presence of an internal positive control of non-neoplastic cells were classified as negative.
Statistical analysis. Statistical analysis was performed using one-way analysis of variance (ANOVA) followed by the Bonferroni's post-test for multiple comparisons. A value of p<0.05 was considered significant. Data are reported as means±SD of at least three experiments.
Succinate dehydrogenase A (SDHA) and SDHB immunohistochemical (IHC) results in a series of SDHx-mutated tumours.
Results
Genetic analysis. Our cohort of 29 patients consisted of 13 (44.8%) with PCC, five males and eight females aged between 20 to 80 years (mean=49.5 years), and 16 (55.2%) with PGL, six males and 10 females aged between 15 and 72 years (mean=46.3 years).
Both wild-type (n=16) and SDHx-mutated tumours (n=13) were identified. Among the 13 SDHx-mutated tumours, the SDHB gene was involved in three (23.1%) cases (two missense cysteine-to-valine replacement mutations in position 191 and one splicing mutation), the SDHC gene in one case (7.7%) (a non-sense mutation with protein translation interrupted in position 42) and SDHD gene in nine (69.2%) cases (five missense mutations, four proline-to-leucine replacements in position 81 and one glycine-to-aspartate in position 106, three non-sense mutations with protein translation interrupted in position 109, and one splicing mutation). With regard to anatomical location, the SDHB-mutated cases were carotid body (n=2) and abdominal tumours (n=1). The SDHC-mutated case was an abdominal tumour, whereas the SDHD-mutated cases were carotid body (n=5), abdominal (n=3) and adrenal (n=1) tumours. In our series, no tumours harbouring SDHA genetic mutations were identified (Table I).
SDH activity and western blot analysis. All SDHx-mutated PCCs/PGLs exhibited significantly decreased SDH activity, ranging from 60% to 90% (Figure 1A). On western blot analysis, levels of SDHA protein expression were similar in all tissue samples (Figure 1B). Enzymatic activity and SDHB expression levels were significantly reduced in tumours harbouring SDHx mutations (Figure 1B and C).
Succinate dehydrogenase A (SDHA) and SDHB immunohistochemical (IHC) results in a series of wild-type tumours.
Immunohistochemistry. SDHB immunostaining detected 10/13 (76.9%) SDHx-mutated PCCs/PGLs: 3/3 SDHB-mutated, 1/1 SDHC-mutated and 6/9 SDHD-mutated samples. In three SDHD-mutated tumours with the same mutation (p.Pro81Leu), the SDHB staining pattern was positive (n=2; 15.4%) or weakly diffuse (n=1; 7.7%) (Table I and III; Figure 2). SDHA protein expression was preserved in all mutated tumours (n=13/13) (Table I).

Succinate dehydrogenase (SDH) activity and expression in phaeochromocytomas/paragangliomas. A: The histogram represents SDH activity expressed as the percentage of the activity measured in tissue homogenates. B: Blot shown is representative of samples from patients with mutated and wild-type (wt) SDHx. C: SDHB expression values were normalized to those of actin. Bars are the mean±S.D. of three independent experiments, *p<0.05 compared to control. Enzymatic activity and protein expression were significantly lower in tumours with SDHx mutations than in wild-type tumours.
All 16 wild-type PCCs/PGLs exhibited SDHB immunoreactivity, while SDHA was positive in 15 (93.8%) cases and weakly diffuse in one (6.2%) (Tables II and III).
Comparison of immunohistochemistry with gene sequencing underlined the high specificity of SDHB staining (100%), with 84.6% sensitivity. Furthermore, positive predictive values reached 100% and negative predictive values 88.9%.
Discussion
Ascertaining whether an individual carries a genetic predisposition for developing PCC/PGL provides important clinical information on the patient's risk of presenting malignant or multifocal lesions, as well as other benign and malignant neoplasms (17-19). The literature provides much evidence to suggest that immunohistochemical staining for SDHB can reliably identify patients with SDHB, SDHC and SDHD gene mutations (9, 16), regardless of the underlying type of mutation (missense, nonsense, splicing, or frameshift). Consequently, immunohistochemistry has been proposed as a screening/triaging test (9, 16, 20). Because of the rarity of sporadic SDHx mutations, loss of SDHB immunoreactivity suggests the presence of a germline mutation in the SDH complex and thus indicates the patient for appropriate genetic testing. On the other hand, in 85% of the PCC/PGL cases in which SDHB expression is expected to be maintained, immunohistochemistry can exclude the need for genetic testing. This approach may be highly beneficial as well as economically sustainable (20).

{kind=link}
{kind=link}
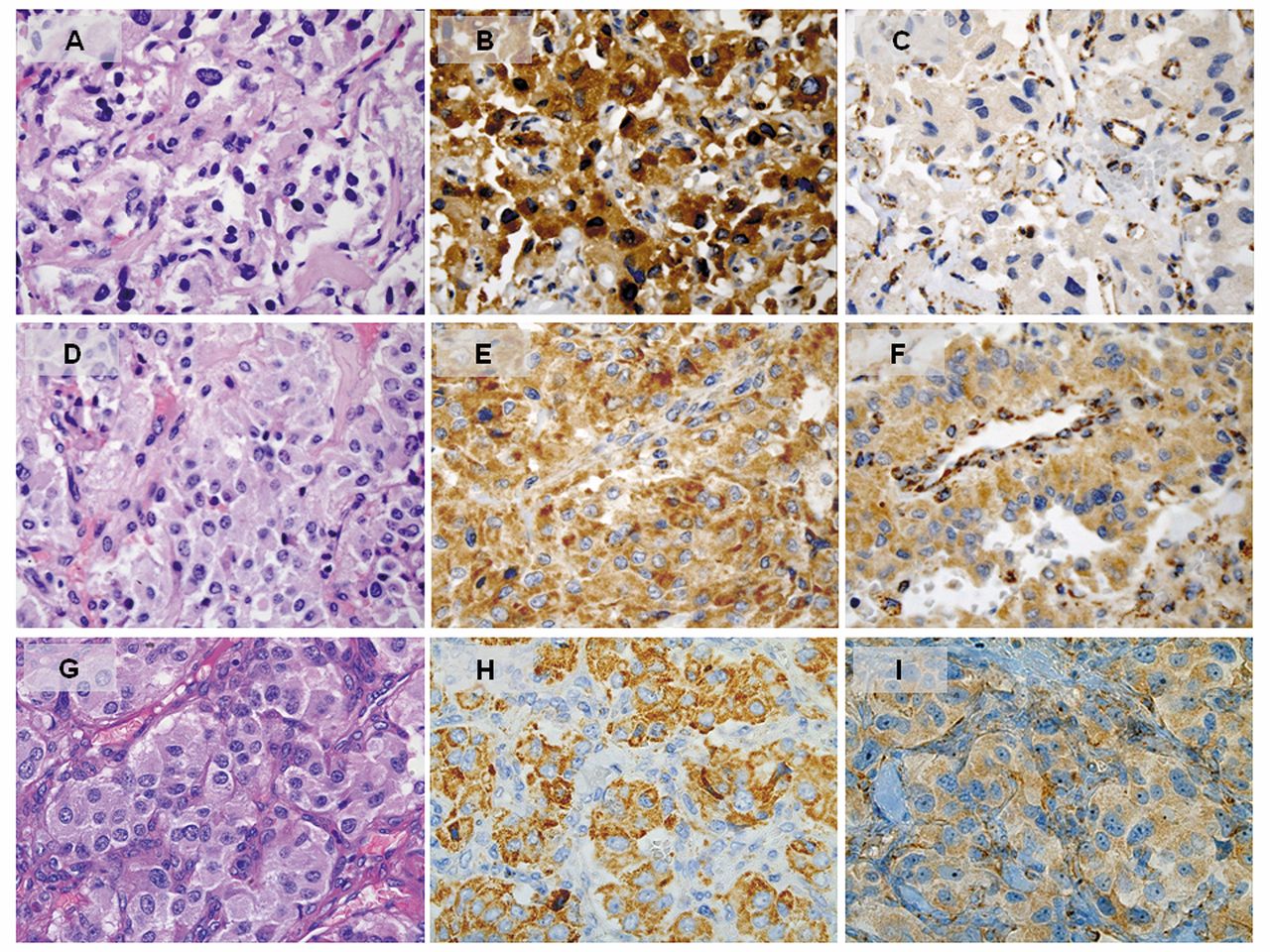
SDHD-mutated (p.Gln109X) extra-adrenal paraganglioma (PGL) (A; haematoxylin-eosin, ×40) immunoreactive for SDHA (B) and negative for SDHB; note that the normal cells of the intratumoural fibrovascular network retain SDHB positivity (C). SDHD-mutated (p.Pro81Leu) extra-adrenal PGL (D; haematoxylin-eosin, ×40) positive for SDHA (E) and negative for SDHB (F). Carotid body tumour (G; haematoxylin-eosin, ×40) harbouring SDHD mutation (p.Pro81Leu) with positive staining for SDHA (H) and weak non-specific cytoplasmic staining for SDHB (I).
Comparison of immunohistochemistry with gene sequencing showed succinate dehydrogenase B staining to be highly specific (100%), with 84.6% sensitivity. Positive and negative predictive values were 100% and 88.9%, respectively.
The results of our study focus attention on the possible pitfalls in identifying patients with SDHx germline mutations by means of immunohistochemistry, particularly in the presence of SDHD gene mutations. Reproducibility in the interpretation of immunohistochemical results is crucial if this technique is to be used as a tool for genetic screening. We adopted the three-category grading system proposed by Gill and collaborators for evaluation of SDHB immunostaining (16). This method seems to improve interobserver concordance when compared to the two-category grading system suggested by van Nederveen and collaborators, which distinguishes between SDHB-positive and SDHB-negative tumours (21). In a study of 43 PCC/PGL cases, including wild-type (n=30) and RET (n=3), VHL (n=4), SDHB (n=3) and SDHD (n=3) mutation-associated tumours, SDHB immunostaining identified only the SDHx-mutated tumours. SDHB was positive in the wild-type, RET-mutated tumours and in two out of the four VHL-mutated tumours. The two other cases associated with VHL mutations, showing weakly diffuse cytoplasmic blush, were considered negative. However, when the criteria put forward by Gill and co-workers were applied and the granular staining pattern considered, the two VHL-mutated cases were deemed as SDHB-positive (20). It is well-known that VHL-mutated PCCs/PGLs may display decreased SDHB expression, thus justifying the weakly diffuse staining at immunohistochemistry (10, 16, 22). Therefore if immunohistochemistry is negative, but no SDHx mutation is detected, VHL testing should be recommended. On the contrary, if immunohistochemistry is positive with no mutation in other candidate genes (i.e. VHL, MEN2), then SDHD mutation should be considered if history is suggestive.
In our series, false-negative cases harboured the same mutation in the SDHD gene (c.242 C>T). Immunostaining was positive in two cases and weakly diffuse in one. These data are in line with previous studies (10, 16, 21). Papathomas and co-authors investigated interobserver variability among seven expert endocrine pathologists using a web-based virtual microscopy approach in a large multicentre PCC/PGL cohort (n=351) and identified two SDHD-mutated extra-adrenal PGL which five observers considered SDHB-positive (10). However, no correlation was found between a weakly diffuse staining pattern and SDHD mutation. It has been proposed that SDHD gene mutations can induce misfolding of the subunits of the SDH complex, with loss of enzymatic activity, while exhibiting an abnormal pattern of immunoreactivity (21). Owing to the possibility of positive or weakly diffuse SDHB immunoreactivity in tumours harbouring SDHD mutations, SDHD staining may be a complementary tool to identify patients with SDHD mutation (23). In the current study, we obtained a positive predictive value of 100% and a negative predictive value of 88.9% for the presence of SDH mutations, employing the same commercially available antibody to SDHB (polyclonal anti-rabbit, HPA002868) used by van Nederveen et al., although at a different concentration (1:500 vs. 1:800) (9). Similar results were also reported using the 21A11 mouse monoclonal antibody to SDHB (16).
In order to correctly evaluate immunohistochemical results, SDHB immunohistochemistry must be performed following well-defined, standardized protocols and in laboratories subject to internal and external quality control. Good practice requires inclusion of internal positive controls (i.e. sustentacular cells and endothelia). Moreover, SDHB and SDHA immunohistochemistry is not always an all-or-none phenomenon and the staining pattern may be heterogeneous. In these cases, SDHx genetic testing is recommended (10).
In previous studies, the percentage of SDHB-negative PCCs/PGLs without SDHx mutations ranged between 5.6% (2/36) (16) and 15.7% (3/19) (21). Failure of genetic analysis to identify SDHx gene mutations, which may be attributable to large-scale deletions or implicate non-transcribed regions, introns or promoters, and epigenetic modifications have been given as explanations for these false-positive results (21). Loss of SDHB immunohistochemical expression has been observed in gastrointestinal stromal tumours as part of the Carney-Stratakis syndrome and the Carney triad (24-26). Recently, two groups working independently reported an aberrant DNA methylation pattern at the SDHC gene locus (SDHC epimutation) in tumours of patients with Carney triad, suggesting its epigenetic inactivation with functional impairment of the SDHx complex as a plausible alternative mechanism of tumorigenesis in Carney triad (7, 27). Based on these observations, in patients affected by gastrointestinal stromal tumours showing loss of SDHB expression, close follow-up is recommended to monitor any possible development of PGL or chondromas of the lung (24, 25). If SDHx genetics does not reveal any mutation in SDHB-immunonegative tumours, SDHC promoter methylation or VHL/NF1 testing can be applied (10).
Our study has a few limitations, including a small sample size. However, in line with previous reports, our study confirms that SDHA protein immunohistochemical expression is maintained in tumours with SDHB, SDHC and SDHD gene mutations. We also observed a wild-type tumour which was SDHA-negative. Nevertheless, this result should not be considered a false-positive because SDHB expression was preserved.
In conclusion, SDHB immunostaining is a useful tool in identifying PCC/PGL associated with mutations of the SDHx genes. Rigorous scoring guidelines are mandatory in clinical reporting if standards of reproducibility are to be improved. One controversial issue is the interpretation of weakly diffuse SDHB immunostaining, from both the technical and diagnostic perspective. This category is most frequently associated with SDHD mutations. A better understanding of the genetic basis of tumorigenesis of PCCs/PGLs may explain unexpected immunohistochemical results.
- Received December 6, 2016.
- Revision received January 19, 2017.
- Accepted January 24, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved