

Abstract
Background/Aim: The TNM staging system for esophageal cancer is designed to predict survival based on pathological stage in patients who have been treated with surgery alone. However, pathological stage can vary considerably after neoadjuvant therapy due to tumor responses. Patients and Methods: We reviewed 110 patients with esophageal squamous cell carcinoma (ESCC) who underwent neoadjuvant chemoradiotherapy (nCRT) followed by surgery, and investigated the effects of nCRT on TNM stage and its prognostic significance. Results: A comparison of pre-treatment clinical and pathological stages (cStage and ypStage, respectively) resulted in 75 (68%) of the patients being down-staged. Good responders (over two-thirds of the primary tumor reduced by nCRT) comprised 100%, 83%, 69%, 52% and 50% of patients with ypStages 0, I, II, III and IV, respectively (p=0.001). In addition, 62 (83%) and 20 (57%) of patients with and without down-staged tumors, respectively, were pathological good responders (p=0.004). We found that cStage did not significantly correlate with survival, whereas univariate analysis significantly associated ypStages III/IV (p=0.003) and down-staged tumors (p=0.04) with overall survival (OS). Multivariate analysis selected ypStage III/IV (HR=3.26; 95% CI=1.52-6.99; p=0.002) and no down-staging (HR=2.06; 95%CI=1.16-3.64, p=0.01) as independent covariates for OS. Conclusion: nCRT could lead to down-staged ESCC tumors for many patients and a good prognosis. The correlation between ypStage and pathological response to nCRT indicated that ypStage could stratify survival and serve as a prognostic predictor after trimodal therapy.
- Chemoradiotherapy
- esophageal cancer
- esophageal surgery
- multimodal treatment
- neoadjuvant chemoradiation
- prognosis
- staging
- squamous cell carcinoma
A multidisciplinary approach comprising of surgery, radiotherapy and chemotherapy is needed for local control of esophageal cancer and to improve the survival of patients (1, 2). The prognosis is generally worse for poor, than for good responders to neoadjuvant chemoradiotherapy (nCRT), and dependent on tumor responses (3).
The TNM staging system (4) was designed to predict and stratify survival based on pathological stage in patients with esophageal cancer who have been treated with surgery alone (5, 6). The pathological TNM stage (ypStage) after neoadjuvant therapy is significantly influenced by tumor responses, and it is quite different from clinical stage (cStage) before treatment due to various degrees of tumor responses. Thus, whether TNM staging is appropriate to guide the prognosis of patients who receive nCRT and then undergo surgery remains controversial (7-11). Thus, the effects of nCRT upon TNM stage and the ability of such effects to predict prognosis need to be clarified in patients with esophageal cancer treated using a trimodal approach.
The present study compares cStage and ypStage (UICC 7th edition) (4), and investigates the effects of nCRT on the staging system and their prognostic significance in patients with esophageal squamous cell carcinoma (ESCC) treated by nCRT followed by uniform surgery comprising transthoracic esophagectomy with lymph node dissection in at least the thoracic and abdominal fields.
Patients and Methods
Preoperative assessment. Patients underwent a physical examination, standard laboratory tests, chest radiography, esophagography, upper gastrointestinal endoscopy and biopsy, and computed tomography (CT) imaging of the neck, chest and abdomen. Patients were also assessed by systematic 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) imaging after 2006.
Primary tumors that appeared superficial on endoscopy, with only slight wall deformation on esophagography and could not be identified on CT images, were clinically staged as T1 (cT1). Endoscopically determined advanced cancers with obvious wall deformation on esophagography and wall thickening on CT images were clinically staged as T2 (cT2). Tumors with obvious wall deformation determined by esophagography and scuffing, or an obviously irregular esophageal external wall on CT images were clinically staged as T3 (cT3). Obvious displacement and deformation of an adjacent organ caused by a primary tumor and the absence of a fat layer between the two, determined on CT images, was clinically staged as T4 (cT4).
Lymph nodes were considered positive for metastatic disease on CT images if they were spherical, and had a maximal transverse diameter >10 mm. Visible lymph nodes that were <10 mm on CT images were regarded as metastasis-positive only if focal 18F-FDG uptake on PET-CT images was obvious compared with normal mediastinal activity.
Patients' characteristics. We reviewed 110 consecutive patients (male, n=96; female, n=14; mean age=63.0±8.0 years) with locally advanced ESCC in the thoracic esophagus or gastroesophageal junction, who underwent nCRT followed by transthoracic esophagectomy without macroscopic residual tumor at our institution between September 2003 and March 2013. The Institutional Review Board at Hiroshima University approved this study.
Patients received nCRT and underwent surgery if they had resectable cancer in the esophagus or gastroesophageal junction, a tumor that was more deeply invasive than cT2, positive for lymph node metastasis, or resectable supraclavicular lymph node metastasis (cM1 LYM). Three patients with cT4 primary tumors that had been reduced and thus rendered potentially resectable after nCRT underwent esophagectomy. Table I shows the clinical characteristics of the patients before nCRT. All histological tumor types were diagnosed as squamous cell carcinoma from biopsy samples obtained before treatment. The cStages of cancer were II, III and IV in 26 (23.6%), 72 (65.5%) and 12 (10.9%) patients, respectively.
Neoadjuvant chemoradiotherapy and surgery. Neoadjuvant CRT comprised concurrent radiotherapy (40 Gy) and chemotherapy with 5-fluorouracil plus either docetaxel, or cisplatin or a combination of both, as described (12-14). Patients with elevated serum creatinine were treated with nedaplatin instead of cisplatin. Thirty-two (29.1%), 56 (50.9%), 18 (16.4%) and 4 (3.6%) patients were respectively treated with the following combinations: docetaxel/5-fluorouracil, cisplatin/5-fluorouracil, docetaxel/cisplatin/5-fluorouracil, and nedaplatin/5-fluorouracil.
Surgery for all patients proceeded 4-8 weeks after the completion of nCRT. All patients underwent transthoracic esophagectomy and at least two–field lymph node dissection (thoracic and abdominal fields), and esophageal cancer in the upper and middle third of the thoracic esophagus or lymph node metastasis in the superior mediastinum was essentially treated by cervical lymphadenectomy. The gastric tube was subsequently lifted via the posterior mediastinal or retrosternal route for cervical anastomosis with the esophagus.
Evaluation of pathological tumor effects. The pathological responses of primary tumors were graded according to the response evaluation criteria for the effects of radiation and/or chemotherapy published by the Japan Esophageal Society as follows: 0, no recognizable cytological or histological therapeutic effect; 1, slightly effective, with apparently viable cancer cells accounting for at least one-third of the tumor tissue; 2, moderately effective with viable cancer cells accounting for less than one-third of the tumor tissue; 3, markedly effective, with no evidence of viable cancer cells (pathological complete response, pCR) (15). We defined grades 2 and 3 as good responses and grades 0 and 1 as poor responses.
If the primary tumor was pathologically absent after nCRT but lymph node metastasis remained, for example, ypT0N(+), the stage was calculated by assuming that ypT is equal to the lowest number and that ypN essentially determines the stage (16). Down-staging was defined as a reduction in the pathological stage (ypTNM) compared with the pre-treatment clinical stage (cTNM).
Statistical analysis. Categorical variables were analyzed using the χ2 test. Survival data were analyzed using the Kaplan–Meier method and compared using the log rank test. Recurrence-free survival was defined as the amount of elapsed time from the date of surgery until the first event (recurrence or death from any cause) or the most recent follow up. Overall survival was defined as the amount of elapsed time from the date of surgery until death from any cause or the most recent follow up. At the time of the outcome analysis, 50 patients remained alive and the survivors were followed up for a median of 63.4 (range=38.0 to 135.9 months) months after surgery. The effects of various clinical parameters on survival were evaluated using univariate analysis, and independent influences were assessed using multivariate Cox proportional hazards analysis. All data were statistically analyzed using SPSS software (version 20.0, IBM, NY, USA).
Results
Effects of neoadjuvant chemoradiotherapy upon TNM staging. Table II shows the pathological parameters after trimodal therapy. The pathological responses of primary tumors to nCRT in 1 (0.9%), 27 (24.5%), 43 (39.1%) and 39 (35.5%) patients were graded as 0, 1, 2 and 3 (pCR), respectively, according to the criteria of the Japan Esophageal Society (15). The pathological depth of the primary tumors was ypT0, 1, 2, 3 and 4 in 39 (35.5%), 13 (11.8%), 20 (18.2%), 34 (30.9%) and 4 (3.6%) patients, respectively. Regional lymph node metastasis was ypN0, N1, N2 and N3 in 60 (54.5%), 33 (30.0%), 15 (13.6%) and 2 (1.8%) patients, respectively, and ypM1 lymph node metastasis was found in 6 (5.6%) patients. Accordingly, the pathological stages of cancer were 0, I, II, III, and IV in 30 (27.3%), 12 (10.9%), 39 (35.5%), 23 (20.9%) and 6 (5.5%) patients, respectively.
A comparison of clinical tumor and pathological stages before and after treatment showed that nCRT resulted in down-staged T, N and M status for 72 (65.5%), 52 (47.3%) and 8 (7.3%) patients, respectively. Therefore, nCRT resulted in down-staged TNM status in 75 (68.2%) patients.
Patients' characteristics before neoadjuvant therapy.
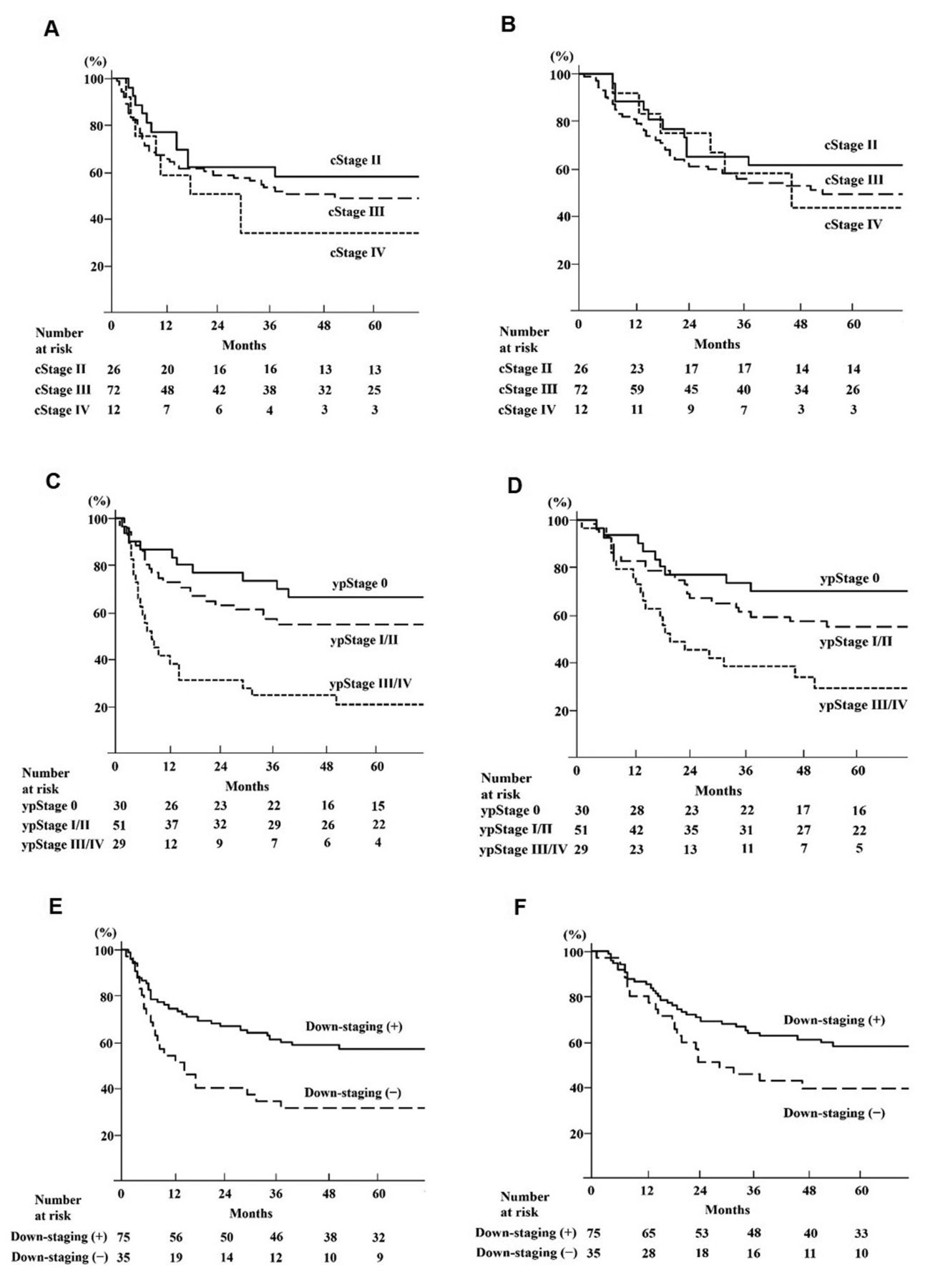
Relationship between pathological primary tumor response and TNM stage. Table III shows the relationship between pathological primary tumor response and ypTNM stage. Thirty (100%), 10 (83.3%), 27 (69.2%), 12 (52.2%) and 3 (50%) patients with ypStage 0, I, II, III and IV tumors, respectively, responded well to nCRT (over two-thirds of the primary tumor reduced to Grades 3 and 2 according to the Japan Esophageal Society response evaluation criteria, n=82, 74.5%; p=0.001). The pathological response of the primary tumor significantly correlated with down-staging, because tumors with a pathological good response were down-staged in 62 (82.7%) patients and not in 20 (57.1%) (p=0.004). Survival according to TNM staging. Figure 1 (a and b) shows that the five-year recurrence–free survival rates for patients with cStages II, III and IV were 57.7%, 48.3%, and 33.3%, respectively (II vs. III, p=0.64; II vs. IV, p=0.24; III vs. IV, p=0.27). The five-year overall survival rates for patients with cStages II, III and IV were 61.5%, 49.3% and 43.7%, respectively (II vs. III, p=0.72; II vs. IV, p=0.71; III vs. IV, p=0.87). Therefore, survival did not significantly correlate with cStage.
Pathological staging after neoadjuvant chemoradiotherapy.
Figure 1 (c and d) shows survival data analyzed based on ypStage. We combined ypStages I and II, and III and IV, and created three groups comprising ypStages 0, I/II and III/IV, because the survival rates of ypStages I and II, and III and IV were essentially comparable and few patients had ypStage IV tumors. The five-year recurrence–free survival rates for patients with ypStage 0, I/II and III/IV tumors were 66.3%, 54.9% and 20.1%, respectively (ypStage 0 vs. I/II, p=0.27; 0 vs. III/IV, p=0.0001; I/II vs. III/IV, p=0.001). The five-year overall survival rates for patients with ypStage 0, I/II and III/IV tumors were 70.0%, 54.5% and 28.4%, respectively (ypStage 0 vs. I/II, p=0.24; 0 vs. III/IV, p=0.001; I/II vs. III/IV, p=0.01).
Relationship between TNM stage and pathological primary tumor response.
Figure 1 (e and f) shows that the five-year recurrence–free survival rates for patients with and without down-staged tumors were 57.0% and 31.4%, respectively (p=0.01). The five-year overall survival rates for such patients were 58.0% and 39.3%, respectively (p=0.04).
Prognostic significance of TNM staging. Table IV shows associations between several perioperative factors and survival. Univariate analysis selected performance status (PS), histological type, ypStage and down-staging as being significantly associated with recurrence-free and overall survival, but not age, sex, tumor location and cStage.
Factors with p<0.05 in the univariate analysis and cStage were then included in separate multivariate analyses that included either down-staging or ypStage along with the other factors to avoid confounding. These analyses selected ypStage (0 vs. III/IV) and down-staged tumors (+ vs. −) as independent covariates for both recurrence-free (HR=3.80; 95%CI=1.83-7.86; p=0.001 and HR=2.50; 95%CI=1.43-4.37; p=0.001, respectively) and overall (HR=3.26; 95%CI=1.52-6.99; p=0.002 and HR=2.06; 95%CI=1.16-3.64; p=0.01, respectively) survival.
Discussion
The 7th editions of the American Joint Commission on Cancer (AJCC) and the Union for International Cancer Control (UICC) Staging Manuals were published 2010 (4). Through the Worldwide Esophageal Cancer Collaboration, a database comprising 4,627 patients with cancer of the esophagus and gastroesophageal junction that were treated only by surgery was assembled from information derived from 13 institutions in a total of five Asian, European and North American countries. A cancer staging system was then generated from the database (5, 6). The value of the system lies in its ability to reflect and predict survival. However, pathological stage changes according to tumor responses to neoadjuvant therapy (ypStage), compared with pStage after surgery alone. Thus, whether the TNM staging system can also predict the prognosis of patients who also undergo neoadjuvant therapy required clarification.
Several studies have assessed associations between prognosis and TNM staging of esophageal cancer with neoadjuvant therapy, but the conclusions have been contradictory (7-11). Some studies included more patients with adenocarcinoma than squamous cell carcinoma (7-10), or evaluated patients given neoadjuvant chemotherapy (9) or used an earlier TNM staging classification (6th edition) (7, 10, 11). The present study included only patients with locally advanced ESCC who underwent nCRT with 40 Gy radiation followed by uniform surgery with adequate lymph node dissection (transthoracic esophagostomy with lymph node dissection in at least the thoracic and abdominal two fields). We then evaluated the pathological responses of primary tumors according to current TNM staging in the UICC 7th edition, as well as associations between TNM stage and prognosis.
Although the prognoses of patients with cStages II, III and IV were similar, univariate and multivariate analyses selected ypStage as a significant variable that could stratify recurrence-free and overall survival. An extremely poor prognosis was associated with ypStage III/IV, in which residual primary tumor and lymph node metastasis resulted from a poor response to nCRT. Thus ypStage, rather than cStage could serve as a prognostic predictor after trimodal therapy for ESCC. Clinical stage was not associated with prognosis, and thus the main objectives of initial staging would be to identify the resectability of locally advanced ESCC with neoadjuvant therapy and provide a baseline from which to compare responses to treatment.

{kind=link}
Survival after neoadjuvant chemoradiotherapy followed by surgery. a. Recurrence–free survival associated with cStage II vs. III (p=0.64), II vs. IV (p=0.24), III vs. IV (p=0.27). b. Overall survival associated with cStage II vs. III (p=0.72), II vs. IV (p=0.71), III vs. IV (p=0.87). c. Recurrence–free survival associated with ypStage 0 vs. I/II (p= 0.27), 0 vs. III/IV (p=0.0001), I/II vs. III/IV (p=0.001). d. Overall survival associated with ypStage 0 vs. I/II (p=0.24), 0 vs. III/IV (p=0.001), I/II vs. III/IV (p=0.01). e. Recurrence–free survival with (+) vs. without (−) down-staging (p=0.01). f. Overall survival with (+) vs. without (−) down-staging (p=0.04).
Tumor regression significantly correlates with ypT or ypN status after nCRT (17, 18). Furthermore, although the ratio of pCR achieved by the surrounding stroma and the regional lymph nodes is high after nCRT for esophageal cancer, residual malignancy frequently involves both the mucosa and the submucosa. The most frequent overall type of regression comprises a mixture of concentric regression and regression toward the lumen (19). The pathological primary tumor response significantly correlated with ypStage in the present study, and nCRT resulted in down-staged T, N and/or M status compared with clinical and pathological stage in many patients with ESCC.
Univariate and multivariate analyses of prognostic factors.
Multivariate analysis selected down-staging as the independent predictor for prognosis. The results of several studies have similarly indicated that down-staging is a good prognostic marker for patients with esophageal cancer treated by neoadjuvant therapy followed by surgery (9, 20). Therefore, accurate clinical staging and a comparison with ypStage based on cStage are also important for prognostic prediction of ESCC after nCRT followed by surgery. The significant role of nCRT is to down-stage initial bulky tumors and metastatic lymph nodes, thus resulting in better survival for patients who achieved a lower pathological stage after nCRT.
Other factors such as PS and histological type determined from biopsy specimens were also significant independent prognostic factors in the present study. Histological grade has already been identified as important for stage grouping in the AJCC staging system (4). Increasing histological grade is associated with incrementally decreasing survival for patients with early-stage esophageal cancers. To distinguish G1 (well-differentiated) from G2 (moderately-differentiated) and G3 (poorly-differentiated) is important for patients with stage I and II squamous-cell carcinoma cancers in this staging system (5). Furthermore, PS also is an independent prognostic factor for patients with advanced esophageal cancer who undergo chemotherapy, definitive CRT and trimodal therapy (21-23). Thus, these factors are also important prognostic factors for ESCC with trimodal therapy.
We attempted to validate the TNM staging system using more finely subdivided stages in a relative small patient cohort. Thus, larger studies are needed to confirm these findings and establish a more optimal staging system to accurately predict the survival of patients with esophageal cancer who undergo neoadjuvant therapy followed by surgery.
In conclusion, nCRT could lead to down-staged advanced ESCC and a better prognosis for many patients. Survival was stratified by ypStage, which correlated with the pathological response to nCRT. Therefore, ypStage rather than cStage could serve as a prognostic predictor after nCRT and surgery.
Footnotes
Conflicts of Interest
The Authors have no commercial support or conflicts of interest to disclose.
- Received August 20, 2017.
- Revision received September 9, 2017.
- Accepted September 11, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved